This prospective cohort work was conducted on 90 participants aging from 18 to 80 years old, both genders. Patients with stable angina pectoris (chronic coronary syndrome) were defined according to recent ESC guidelines [16] as chest pain or discomfort (angina) suspected to be due to myocardial ischemia. The work had been conducted from October 2022 to October 2023 following approval from the Ethics Committee from Minia University Hospitals, Minia, Egypt. All participants provided well-informed written consent.
Criteria for exclusion were patients who had a history of ACS (Prior STEMI, NSTEMI or unstable angina), cardiomyopathy (of any etiology) with LVEF less than 55%, atrial fibrillation (Afib), significant valvular heart disease, poor image quality, acute autoimmune or infectious disorders, malignancies, dysfunction of thyroid and severe renal or hepatic insufficiency.
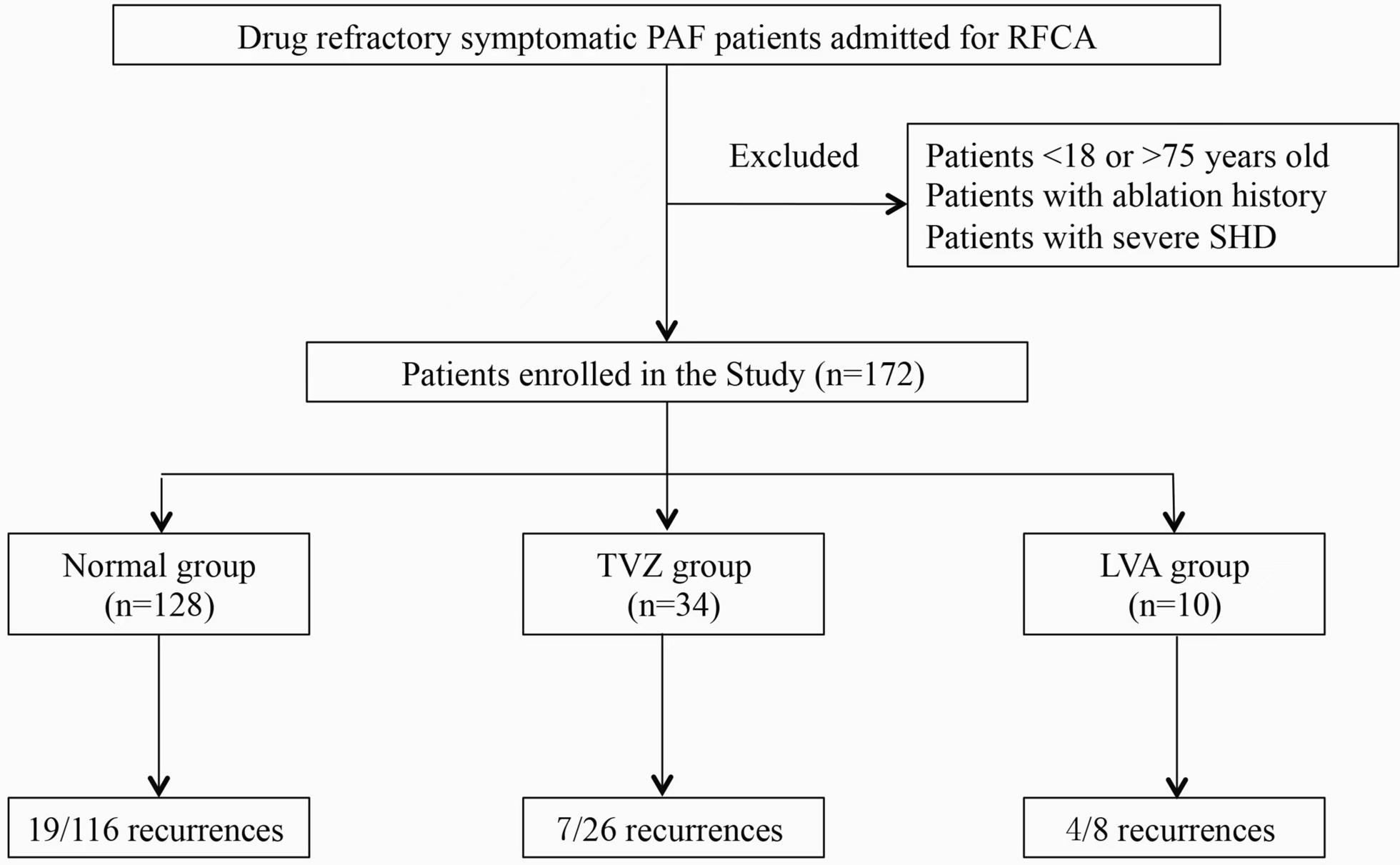
Participants had been divided into three groups: Group I (n = 30): control group that scheduled by normal coronary angiography and group II (n = 60): case group which subdivided into two subgroups equally: IIa: case group with simple lesion (Gensini score < 20) and group IIb: case group with complex lesion (Gensini score of ≥ 20).
Each participant underwent comprehensive taking of history, clinical examinations, laboratory tests [full blood picture (CBC), renal and hepatic function tests].
Soluble suppression of tumorigenicity 2 assay
Blood samples were withdrawn from all participants utilizing tubes containing EDTA. Prompt centrifugation was followed by storage of the separated plasma samples until analysis as done in our previous work [17]. Analysis of plasma sST2 levels was conducted using ELISA assay kits supplied by Elabscience, USA (catalog No.E-EL-H6082) based on sandwich ELISA technique. The assay calibration was carried out following the guidelines provided by the manufacturer, and subsequent data were normalized to a standard curve using microplate ELISA reader (EMR-500, USA).
Three-dimensional speckle-tracking analysis
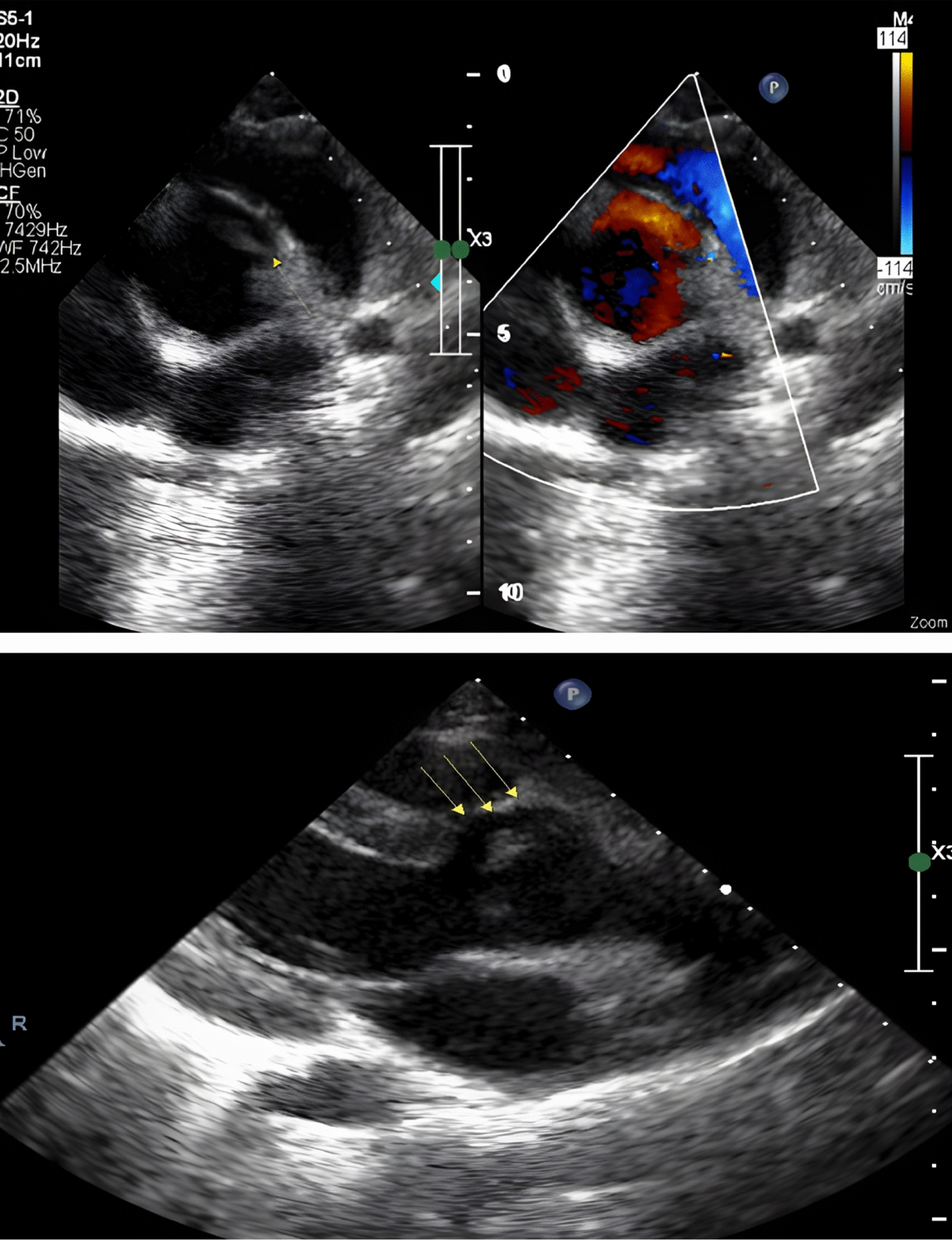
Baseline 3D echocardiography had been conducted before coronary angiography using Echo-machine GE Vivid E95 and 4Vc-D probe. Images were obtained from individuals in the left lateral decubitus posture and linked to an ECG using the echocardiography standards. A rate of frame greater than 25 frames per second was maintained for 3D-STE. Automated measurement of LVEF was conducted using 4D auto LVQ. The program autonomously identifies the endocardial boundary of the cavity of LV and computes the volumes of the LV. If the investigator observed the auto endocardial border detection to be incorrect, the left ventricular endocardial borders were altered manually using a point-click approach in a multiplanar layout consisting of three transverse and three apical planes. Then, this was a secondary automated refinement of the detection of boundaries depending on the obtained findings. After evaluating the left ventricular volumes and EF, an automated mapping of the epicardial boundary was shown to determine the specific area of interest needed for measuring left ventricular mass and myocardial deformation. This trace of epicardium was calibrated manually to involve the whole thickness of the left ventricle wall utilizing the same point-click technique. The LV’s global peak systolic strain, GCS, GAS and GLS were identified as the strain parameters.
Coronary angiography
CAD was identified when any of the primary coronary arteries, such as left main (LM) coronary and left anterior descending (LAD), left circumflex (LCX) coronary and right coronary arteries, were blocked due to occlusion above 50% of the lumen diameter. When the biochemical condition of a participant is unclear, skilled cardiologists may utilize the score of Gensini to evaluate the CAD severity [18].
Gensini score
The score of Gensini [19] was measured by multiplying the severity coefficient, that was allocated to each stenosis of coronaries depending on the degree of constricting of the vessel (decreases of 25%, 50%, 75%, 90%, 99% and total blockage were assigned scores of Gensini of 1, 2, 4, 8, 16 and 32, correspondingly), by the coefficient that was established by the functional importance of the myocardial region supplied by this particular segment. This was done in order to arrive at the Gensini score. The LM coronary artery, 5; the LAD coronary artery proximal segment, 2.5; the LAD coronary artery mid-segment, 1.5; the LAD coronary artery apical segment, 1; the 1st diagonal branch, 1; the 2nd diagonal branch, 0.5; the CX artery proximal portion, 2.5 (if Lt coronary artery dominancy exist 3.5); the CX artery distal portion, 1 (if dominant, 2); the obtuse marginal branch, 1; the posterolateral branch, 0.5; the Rt coronary artery proximal portion, 1; the Rt coronary artery mid-segment, 1; the Rt coronary artery distal portion, 1; and the posterior descending artery, 1. A majority of studies classified a score of Gensini ≥ 20 as severe atherosclerosis.
Sample size calculation
The sample size calculation was performed using EpI-Info 2002 software statistical package designed by World Health Organization (WHO) and by Centres for Disease Control and Prevention (CDC).
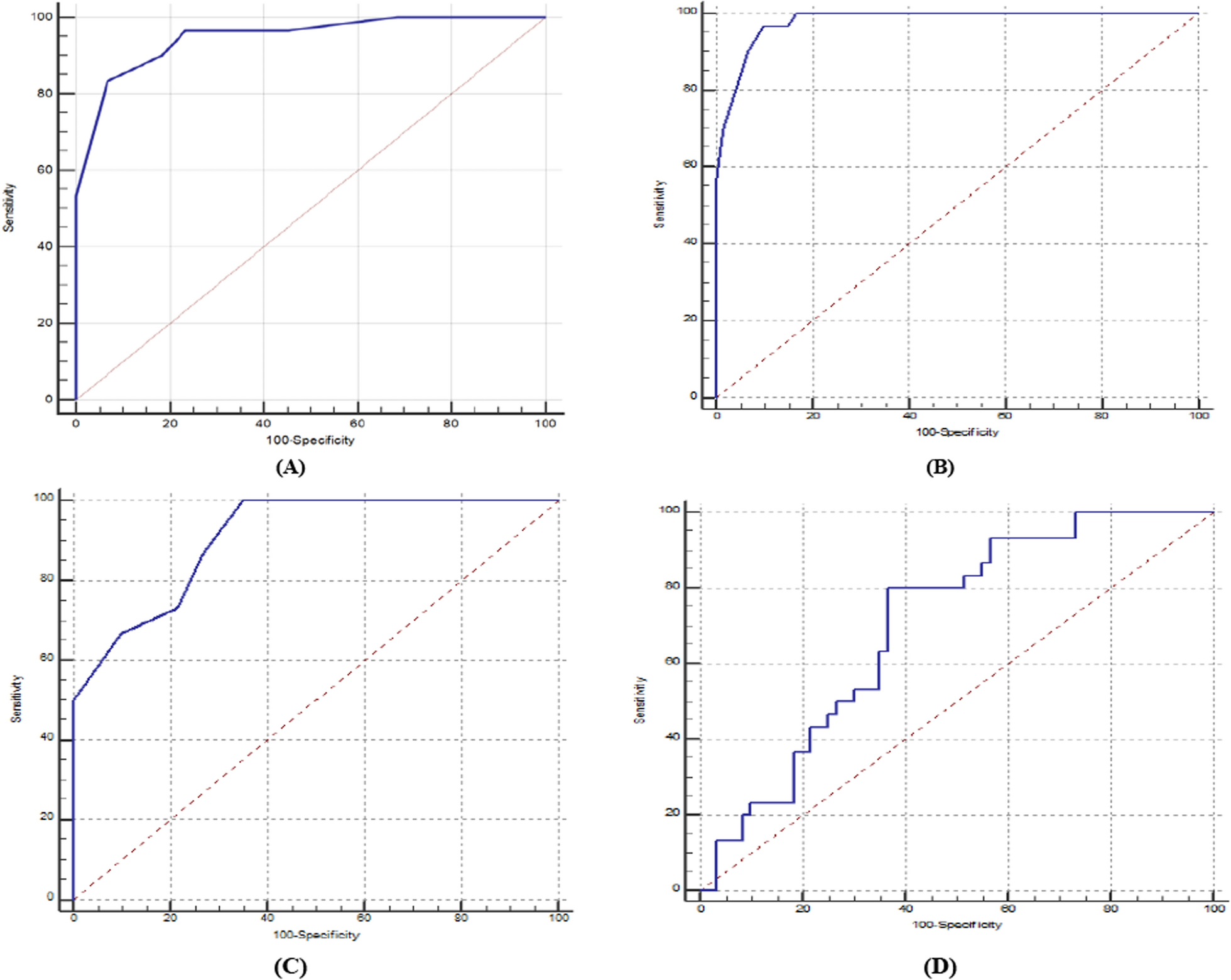
The sample size was calculated based on the following considerations: 95% confidence level and the prevalence of accuracy of GLS for prediction of severity of CAD in CCS patients was 90% according to a previous study [20] ± 5% confidence limit. Seven cases were added to overcome dropout. Therefore, we will recruit 90 cases.
Statistical analysis
Statistical analysis had been carried out utilizing SPSS v26 (IBM Inc., Chicago, IL, USA). Quantitative factors had been displayed as mean and standard deviation (SD) and contrasted across all groups utilizing ANOVA (F) test with post hoc test (Tukey). Qualitative parameters had been displayed as frequencies and percentages (%) and were analyzed employing the Chi-square test. A two-tailed P value < 0.05 was deemed statistically significant.







Comments (0)