Cardiac myxoma is a tumour of mesenchymal origin comprising almost half of all primary cardiac tumours [4]. As many as 10% of patients with atrial myxoma remain asymptomatic. They usually present with systemic embolism, intracardiac obstruction, constitutional symptoms and rarely with arrhythmia or acute coronary syndrome (Table 1) [5, 6]. Acute ischaemic stroke is the most common neurological sequel secondary to tumour embolism, and others include intracranial aneurysms, vascular malformation and parenchymal metastases [7]. In a recent systematic review of 55 patients with atrial myxomas and intracranial aneurysms described to date, the majority were females (65%) and young (age < 60 years, 86%) [3, 8]. Aneurysms were detected before, during or even 25 years after the diagnosis/resection of the atrial mass [3].
Table 1 Comparison of the index case with existing reported cases (summarised from a systematic review by Chojdak-Łukasiewicz J et al. [3])The pathogenesis of aneurysm formation is not well defined, and several mechanisms have been postulated. Firstly, tumour cell infiltration of the vessel wall via vasa vasorum leads to vessel wall destruction. However, the relative lack of vasa vasorum in the intracranial arteries in human autopsy studies contradicts the proposal [9]. Secondly, occlusion by tumour emboli causes subsequent scarring and pseudoaneurysm [10]. Thirdly, breach of the internal elastic lamina of vessels by direct invasion by the tumour cells, subsequent IL-6-mediated inflammation and damage to the arterial wall by excess matrix metalloproteinases leading to subsequent aneurysm formation [11, 12]. This is supported by the histological examination in a few case reports [12].
The natural history of the aneurysm is not well defined. Few reports have shown the stability of the lesions over many years, or even regression with excision of myxoma [13, 14]. In patients with atrial myxoma and intracranial aneurysms, the most common manifestation was vascular incidents (25%) in the form of transient ischaemic attacks or strokes secondary to embolism and aneurysms were mostly detected coincidentally [3]. Patients with multiple intracranial aneurysms may be asymptomatic or experience nonspecific headaches which can be predictive as seen in our case [3]. Seizures and dizziness have also been reported secondary to microbleeding from aneurysms. Subarachnoid or intracerebral bleeds were very rare.
Magnetic resonance imaging and computed tomography can show infarcts, haemorrhage or aneurysms. T1-weighted MRI images may show aneurysmal segment and may show enhancement either due to a slow flow phenomenon or enhancement of the tumour cells/myxoid matrix within the vessel wall [15, 16]. Conventional angiogram may be planned for the characterisation of the aneurysms which are commonly multiple and fusiform located more peripherally. Anterior and middle cerebral arteries are the most common arteries involved. Extracerebral artery involvement is very rare due to the avidity of myxoma cells for cerebral blood vessels [8] .
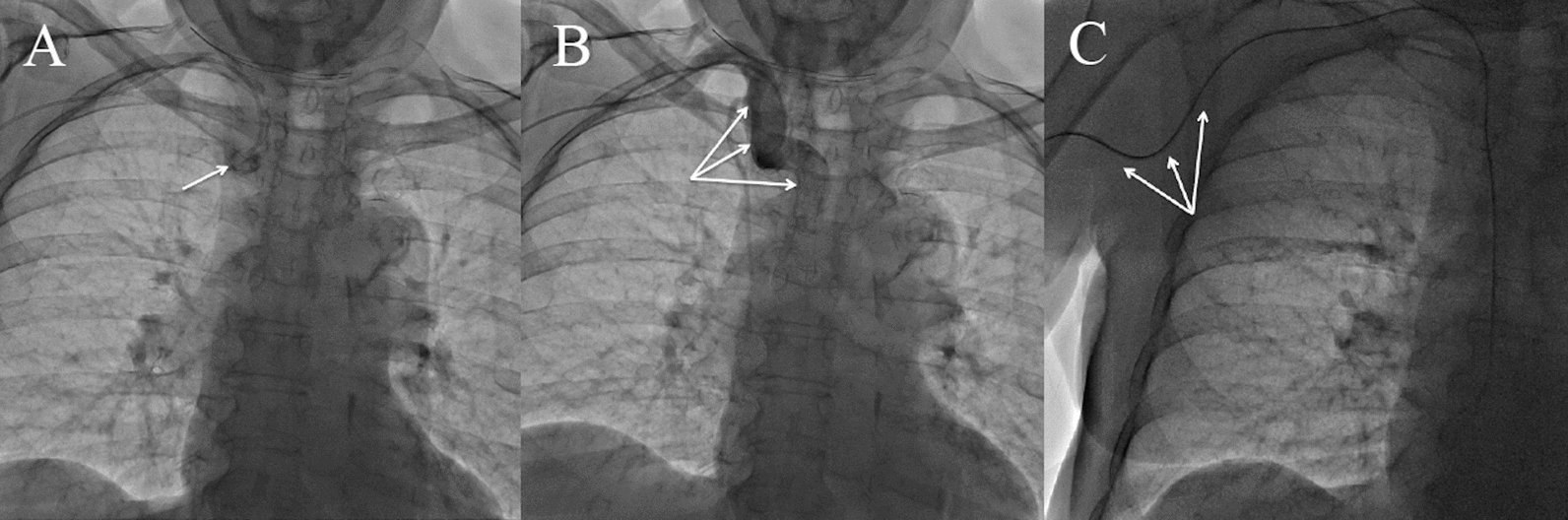
Cognitive disturbance is an uncommon presentation in atrial myxomas which can be due to recurrent infarcts or bleeding from aneurysms. Our patient presented with cognitive decline secondary to recurrent subcortical infarcts caused by myxomatous embolism which could have been averted had she undergone evaluation for her stroke earlier. Digital subtraction angiogram showed multiple aneurysms at distal branches which were predominantly fusiform, the aetiology of which can be attributed to myxoma in the absence of other risk factors or genetic morphology for aneurysms.
The atrial myxoma should be excised as soon as possible after the diagnosis to prevent further complications. During surgery, three important points are to be ensured to prevent recurrence and future complications: (1) removal of the multi-focal tumour; (2) removal of appendages when and where required; (3) avoidance of tumour fragmentation and embolization [17].
Currently, there is a lack of specific guidelines for the treatment of aneurysms caused by cardiac myxomas. However, a watchful clinical and radiological follow-up is recommended [15, 18]. A lot of therapeutic methods, ranging from endovascular methods, surgery, chemotherapy, radiation or a combination of these, are available. By default, endovascular treatment is not recommended because they are multiple, distally located, fusiform and without neck. Only enlarged or ruptured aneurysms may require invasive management and must be evaluated for endovascular or neurosurgical intervention [19]. Open surgical management is required for a lesion causing mass effect or in a single saccular aneurysm not amenable to percutaneous interventions.
In recent years, chemotherapy with doxorubicin or a combination of etoposide and carboplatin was useful in some cases in conjunction with surgical excision of myxoma [20, 21]. Chemotherapy may prevent aneurysm growth [22]. Low-dose radiation in combination with chemotherapy has been reported as an effective method for the degradation of metastasis [23]. A new option of frameless stereotactic radiosurgery (SRT) has emerged less invasive and less toxic alternative [24].
Despite the presence of multiple, small aneurysms, the patient's lack of serious aneurysm-related symptoms allowed for medical follow-up following the atrial myxoma excision. Nevertheless, close follow-up was recommended. The patient remained asymptomatic and showed no signs of neurological decline. Interval imaging was deemed unnecessary in the absence of symptoms.







Comments (0)