
Remember me



Despite efforts to limit the transmission of HIV in the United States, there were more than 30,000 new diagnoses in 2020.1 Historically, most HIV transmission events were associated with persons with HIV (PWH) who were unaware of their diagnosis.2 However, more recently, modeling has suggested that PWH with diagnosed HIV who are out of care (PWH-OOC) may account for the majority of new HIV transmission events.3 This is largely driven by the large number of PWH in the United States who are not retained in care: among approximately 925,000 diagnosed PWH in 2019, just 57.8% were retained in care and only 65.5% had a viral load result that was suppressed during 2019.4 Identifying, reengaging in care, and restarting antiretroviral therapy (ART) for PWH-OOC is essential to prevent onward transmission of HIV in the United States and is a key component of the Ending the HIV Epidemic plan.5,6
Research evaluating strategies to improve reengagement in care among PWH-OOC is often challenging due to high rates of syndemic conditions including substance use disorders, mental health disorders, and unstable housing.7–9 Evaluation and comparison of specific interventions designed to improve reengagement are limited with many studies being observational in nature and/or comprising multiple simultaneous interventions.10–21 A meta-analysis of all studies conducted in the United States with any comparative arm concluded that patient navigation, appointment help/alerts, psychosocial support, and transport/appointment accompaniment improved reengagement in care and viral suppression though the quality of evidence was rated as moderate to weak for most studies included.22
Sixty-Minutes-for-Health is a brief, theory-based, one-session behavioral intervention delivered in person by motivational interviewing to improve retention in HIV care by identifying and correcting misinformation regarding health care, enhancing motivation to achieve personal health goals, building skills to cope with emotional distress, and increasing self-efficacy in navigating healthcare logistics among competing priorities. In one small randomized controlled clinical trial pilot study among individuals who had had a gap in HIV primary care of >6 months, a greater proportion of participants who received the 60-Minutes-for-Health intervention were retained in care after 12 and 24 months compared with those who received a time-and-attention control.23 Notably, rapid ART start and linkage to a range of social support and primary care services were not available in this initial pilot. In this study, we sought to compare viral suppression and engagement in care among PWHs who were out of care who were randomized to InstaCare (a complex intervention that integrated the 60-Minutes-for-Health intervention with rapid ART start) or control (a time-and-attention diet-and-nutrition behavioral intervention integrated with rapid ART start).
METHODSA prospective open-label randomized controlled trial of InstaCare, a complex intervention integrating the 60-Minutes-for-Health behavioral intervention with the rapid start of ART, compared with a time-and-attention control also with rapid start of ART was conducted among PWHs who were out of care. All study participants received rapid restart of no-cost ART at enrollment (defined as restart within 7 days of contact to reestablish care). The behavioral intervention/control sessions were provided in person at enrollment.
SettingParticipants were recruited in San Diego, CA, one of the 50 high-priority Ending the HIV Epidemic jurisdictions in the United States.24 The University of California San Diego (UC San Diego) Healthcare (UCSDH) is a large, tertiary referral hospital that is a major provider of HIV services, caring for over 3000 PWHs. The HIV Medicine Clinic provides care for a broad socioeconomic population with significant low income and an ethnic/racial mix representative of the surrounding County.
PopulationParticipants were recruited predominantly from the UCSDH system using 3 main strategies:
Electronic medical records (EMR) from the HIV Medicine Clinic were used to identify PWH who had not attended routine HIV primary care follow-up. Study coordinators called these PWH to verify eligibility. All individuals calling or walking into the HIV Medicine Clinic were screened for eligibility. Individuals who presented to the UCSDH emergency department and were found to be out of care were evaluated for eligibility by study coordinators before discharge from the hospital.Participants were eligible if they were 18 years or older, had been living with HIV for at least 6 months, and were out of care. Out of care was defined by no receipt of ART for the preceding 2 weeks AND any of (1) no HIV provider visit in the prior 6 months; (2) 2 or more HIV viral loads >200 copies/mL separated by at least 30 days in the past 18 months; (3) 2 or more missed appointments with HIV providers in the past 18 months. The definition of out of care was modified during follow-up to include points (2) and (3) due to slow enrollment. Participants were also considered to be eligible if they fulfilled the inclusion criteria but had already reinitiated ART within the prior 24 hours following an emergency department visit or after walking into the HIV Medicine Clinic.
Study InterventionParticipants were randomized 1:1 to InstaCare, a complex intervention that integrated the 60-Minutes-for-Health behavioral intervention with rapid ART start, or control, a time-and-attention diet-and-nutrition behavioral intervention integrated with rapid ART start. The intervention was administered to participants during enrollment and within 24 hours of rapid ART start. The 60-Minutes-for-Health behavioral intervention has been described previously but briefly, it comprises an interactive workbook that facilitates 4 theory-based discussions to improve participants' information, motivation, and behavioral skills toward engaging in their healthcare.23 Section 1, Focusing on my physical health, aims to normalize retention in HIV care and to identify and correct retention-related misinformation and faulty heuristics. It further elicits participants' physical health priorities that might improve retention in care. Section 2, Focusing on my emotional health, aims to explore emotions about living with HIV and how those feelings may facilitate or impede routine HIV care visits. Behavioral skills for coping with these emotions are identified and practiced and participants are encouraged to practice at home. Section 3, Building on my HIV care history, helps participants identify previous care gaps and explores motivations, behavioral skills, and contexts affecting retention history. The discussion helps leverage personal strengths to promote improved retention. Section 4, Achieving my personal health goals, integrates aspects to support participants in identifying a personal health goal and developing targeted action plans to build motivation, skills, and resources to attain this goal. The time-and-attention control was adapted from Project Eban's health promotion arm to allow the behavioral intervention to be delivered through the same motivational interviewing-based approach and in a one-on-one 60-minute session.25
Study ProtocolAt the initial visit, all participants were randomized by random sequence by study staff and received either active or control intervention. During the initial visit, the participants completed sociodemographic assessments and received study-specific HIV care and social support peer navigation, assistance with insurance application, linkage to HIV provider, free transportation to healthcare appointments, linkage to housing resources, and free HIV medication (bictegravir/emtricitabine/tenofovir alafenamide) if insurance was unavailable. Additional HIV Medicine Clinic resources were also available to all participants including medication-assisted treatment for substance use disorder, mental health services, behavioral health services, social work services, case management, financial counseling, free transport, HIV care and social support peer navigation, and specialist pharmacy services.
All participants subsequently received study phone calls at weeks 1 and 2 for ART adherence/counseling and HIV care and social support navigation. In-person study follow-up visits occurred at weeks 4, 24, and 48 for ART adherence/counseling, outcomes assessments, HIV care and social support navigation, and sociodemographic assessments. Study activities are summarized in Table 1, Supplemental Digital Content, https://links.lww.com/QAI/C305.
Sociodemographic Data AssessmentsThe baseline study evaluation included collection of demographic data, household income, highest education attainment, insurance provider, HIV care history, reasons for stopping prior ART regimens, barriers to care assessment, engagement in care assessment, sexually transmitted infection history, comorbidities, HIV care management questionnaire, HIV transmission risk assessment, unmet needs assessment, current living situation assessment, services receipt assessment, and physical examination. Additional structured questionnaires administered during this study included the Alcohol Use Disorders Identification Test (AUDIT-C) alcohol assessment, the ASSIST smoking and substance use assessments, the Drug Abuse Screen Test (DAST-10), the Patient Health Questionnaire (PHQ-9), and the Generalized Anxiety Disorder (GAD-7).26–32
OutcomesThe primary outcomes were the proportion of participants with viral load <50 copies/mL at week 24 after enrollment and the proportion of participants with 2 or more HIV provider visits (abstracted from the EMR) separated by at least 90 days by week 24. Viral load was assessed either at the week 24 study visit or by abstraction from the EMR if a result was available. Outcome measures were abstracted from the EMR even if participants were lost to study follow-up. Secondary outcomes included the proportion of participants with viral load <50 copies/mL 48 weeks after enrollment. A secondary sensitivity analysis using a viral load threshold of 200 copies/mL was performed. Other outcome assessments included questions regarding the acceptability of rapid restart of antiretroviral therapy at week 4.
StatisticsAnalyses of virologic suppression and engagement in care were conducted on an intention-to-treat basis. Participants without viral loads at week 24 or 48 or who were lost to follow-up were included in the denominators for pertinent events. Group differences were tested using Fisher's exact test for binary and categorical variables and the Wilcoxon rank-sum test for continuous variables.
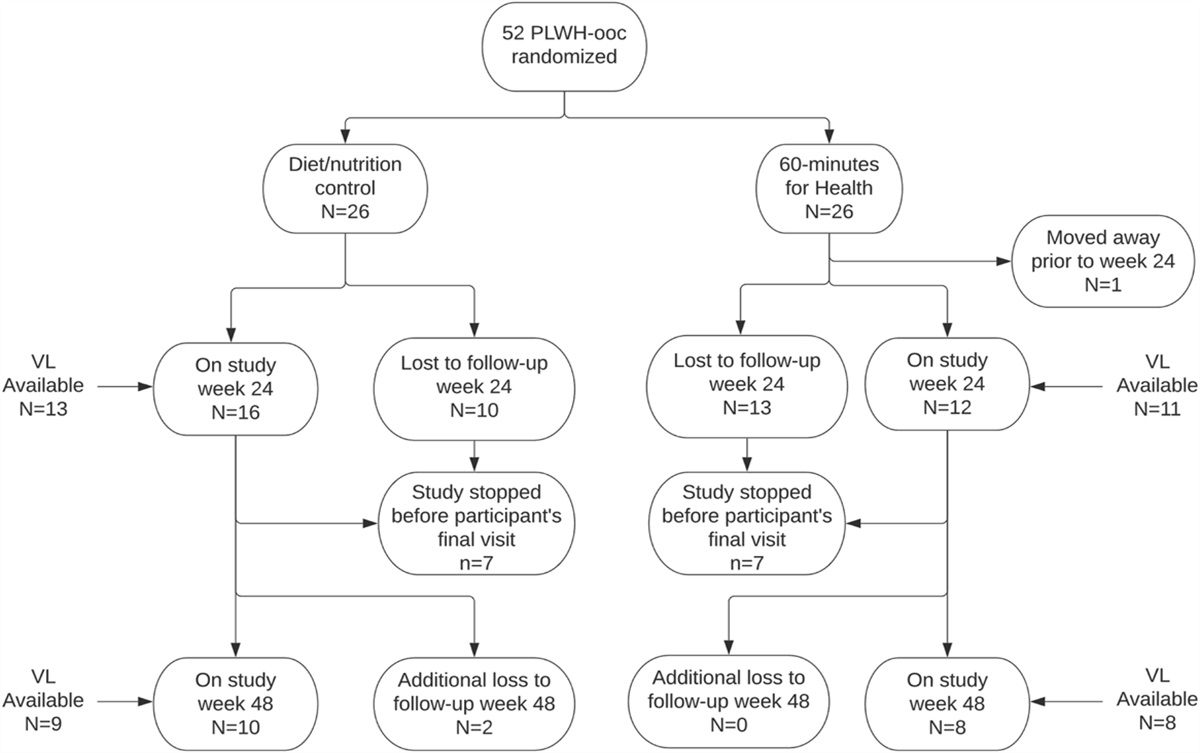
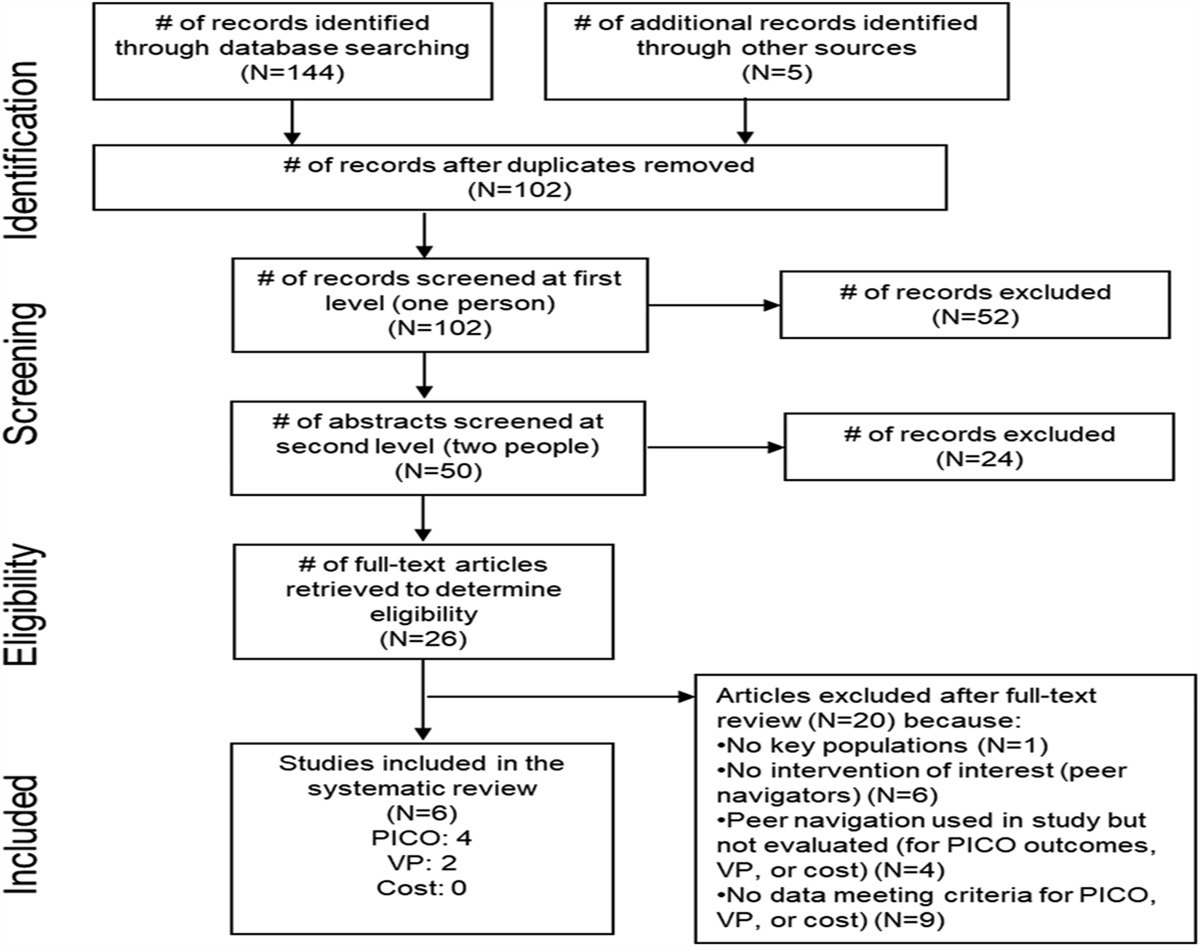
RESULTSA total of 52 PWH-OOC were enrolled between November 2020 and August 2022. The majority (94.2%) were recruited through contact with or outreach from the HIV Medicine Clinic with a smaller number recruited during hospitalization (5.8%). All participants were randomized with 26 receiving the InstaCare complex intervention and 26 receiving the time-and-attention control. In both study arms, all participants were provided with rapid restart of antiretroviral therapy within 7 days of enrollment. One participant, although provided with ART within 7 days, ultimately deferred initiation until day 28 and in 2 participants, ART was initiated outside the defined protocol window restarting ART 3 days and 2 days before enrollment (median time to ART initiation 0 days [range -3 – +28 days]). The participant flow diagram is shown in Figure 1, and participant demographics and prior HIV treatment information are summarized in Table 1 and in Table 2, Supplemental Digital Content, https://links.lww.com/QAI/C305. Among 52 participants, 12 and 23 were lost to follow-up by week 4 and week 24, respectively; 1 participant moved away before the week-24 visit and was not available for follow-up—for participants lost to study follow-up, study outcomes were abstracted from the EMR where available. This study was terminated early due to slow enrollment mostly due to the SARS-CoV-2 pandemic.
 FIGURE 1.:
FIGURE 1.: Participation and loss to follow-up through 48 weeks.
TABLE 1. - Baseline Participant Characteristics by Study Arm TotalNumber of participants who are missing data:
*n = 1.
†n = 3.
‡n = 4.
§n = 12.
‖n = 13.
Baseline evaluations were notable for a high proportion of participants (49%) reporting substance use (not including cannabis) in the 1 month before enrollment and 15.7% reporting injection drug use. Among participants reporting substance use, 88% used methamphetamine, 20% gamma-hydroxybutyrate, and 8% street opioids. Across all participants, 55% had a moderate or substantial drug use disorder using the DAST-10 assessment and 33.3% had heavy or hazardous alcohol intake. Symptoms of mental health disorders were also highly prevalent with nearly half (49%) demonstrating moderate or worse symptoms of depression on PHQ-9 testing and 41.7% with moderate or worse anxiety using the Generalized Anxiety Disorder assessment. More than half the participants (51%) reported living in unstable housing including staying on the streets, in single-room occupancy housing, in a hospital, at a friend's place, or in transitional housing. Groups were overall well matched but there was a trend for lower household income (P = 0.07), lower educational attainment (P = 0.09), increased substance use (P = 0.10), and higher PHQ-9 scores (0.10) in the control group.
Complex sociostructural barriers prevalent in the sample at baseline were reflected in participants' responses for reasons they had previously discontinued their ART regimen with 25.5% reporting mental health issues, 23.4% reporting substance use issues, and 27.7% reporting housing issues as reasons for prior ART discontinuation. In addition, a substantial proportion cited insurance issues (27.7%) as a reason for discontinuing their prior ART regimen. A prior history of gonorrhea was reported by 32 (62.7%), chlamydia by 25 (49.0%), and syphilis by 29 (56.9%). At enrollment, 10 (25.6%) participants had active chlamydia or gonorrhea infection and 10 (26.3%) were found to have active syphilis infection. The median number of sex partners in the past month was 0 though responses ranged from 0 to 50.
OutcomesAt week 24, 28/51 (54.9%) participants remained in this study, and 23 were lost to follow-up. The intention-to-treat (ITT) analysis showed that the overall proportion of participants with HIV viral load <50 copies/mL was 37.3% (19/51) and did not differ between groups (InstaCare 28.0%, control 46.2%, P = 0.25). When only including participants who had a viral load available at week 24 (N = 24), the proportion with viral suppression was 79% (19/24). At week 24, 14 (27.5%) participants had had 2 or more HIV primary care visits separated by at least 90 days and did not differ between groups (InstaCare 7/25 [28.0%], control 7/26 [26.9%], P = 1.00). The main outcomes are summarized in Table 2 and Figure 2. Among individuals with data at week 48 (n = 37), viral suppression was 36.8% in the control arm and 33.0% in the InstaCare arm (P = 1.00).
TABLE 2. - Study Endpoints N Total*This study was prematurely stopped in March 2023, so only 37 participants were available for week-48 visits.
 FIGURE 2.:
FIGURE 2.: Summary of HIV viral suppression and engagement in care outcomes at week 24. Proportions are expressed on an ITT basis. Engaged in care defined as ≥2 visits with HIV provider separated by at least 90 days by week 24; suppressed viral load defined as HIV VL ≤50 copies/mL at week 24. HIV VL, HIV viral load; ITT, intention-to-treat.
Among participants completing the week 4 visit (N = 34), the median level of satisfaction with HIV medications was 5 (interquartile range [IQR] 4–5) on a 5-point Likert-type scale (1 = very low, 5 = very high) with 76% reporting a high or very high acceptance of HIV medications. 94% of participants disagreed or strongly disagreed that they experienced emotional distress associated with restarting ART (median 1, IQR 1–2 on a 5-point Likert-type scale [1 = strongly disagree, 5 = strongly agree]). Week 4 and week 24 sociodemographic evaluations subdivided by intervention are included in Figure 1, Supplemental Digital Content, https://links.lww.com/QAI/C305.
DISCUSSIONThis study did not observe a significant difference in viral load or retention in HIV care 24 weeks after having received the InstaCare complex intervention compared with a time-and-attention control. Complex sociostructural barriers to engagement in care were reported among participants at baseline, including mental health, substance use, housing, and insurance barriers. Despite access to rapid ART-start and access to a range of social support and primary care services, as well as financial compensation for study visits, the rate of loss to study follow-up (>40%) and lack of engagement in care (>70%) by week 24 highlights the challenges of studies evaluating interventions among PWH-OOC. Rapid ART was associated with high levels of acceptance by participants, but viral suppression outcomes were poor overall and similar to other programs providing low-barrier HIV care in the United States.33,34 Differences in this evaluation of InstaCare and the original pilot evaluation of 60 minutes for Health may reflect a more entrenched influence of sociostructural barriers on ART discontinuation vs. gaps in HIV primary care among patients who may have managed to sustain ART utilization to some degree.
A cornerstone of the Ending the HIV Epidemic goals is to increase the proportion of PWHs with suppressed viral load to >95% by the year 2025. To achieve this goal, it is essential that health care and society find improved ways to engage and reestablish treatment among PWH-OOC. It was striking that this study, which provided expanded social, mental health, medical, and financial counselor support with additional financial compensation for participation, achieved a viral suppression of just 37.3% on an ITT basis. This suggests that services offered as standard of care, or supplemented to an enhanced standard of care, are not addressing the underlying needs or issues of this population. To understand these issues better, we performed a post hoc analysis to assess correlates of having 1 or fewer primary HIV care visits by 24 weeks. Individuals who reported substance use as the reason for stopping their most recent ART regimen (P = 0.02) and individuals with higher levels of education attainment (P = 0.01) were less likely to have reengaged with care by week 24. Although not reaching statistical significance, it was notable that the proportions with methamphetamine use in the prior month (48.6% vs. 28.6%), moderate or substantial drug abuse on DAST-10 (59.4% vs. 42.8%), and prior mental health diagnosis (56.8% vs 28.6%) were higher among individuals that did not engage with care.
Several other US centers are exploring strategies to improve reengagement in care. One recent meta-analysis provided useful evidence, though rated as moderate to weak in certainty, that patient navigation, appointment help/alerts, psychosocial support, and transport/appointment accompaniment may help reengagement in care, though these services would be considered standard of care at most HIV centers.22 Some notable US centers for low-barrier HIV care include the POP-UP clinic in San Francisco and the Max Clinic in Seattle, which have both published observational outcomes.7,33,34 The Max Clinic provides a ladder of incentives in addition to low-barrier care though outcomes of viral suppression (44% with 2 viral loads ≤200 copies/mL ≥60 days apart) were consistent with our week 24 outcome (37.5% with viral load <50 copies/mL). The POP-UP clinic was designed to address the needs of people experiencing homelessness or unstable housing incorporating low-barrier care, financial incentives for visits and HIV viral outcomes, enhanced outreach, social work/case management, and substance use/mental health provider training.33 The clinic design was further refined over time using a discrete choice experiment to develop interventions. After 12 months, 44% of 112 participants were virally suppressed and 70% had 1 or more follow-up visits in each 4-month period. Outside the United States, it is notable that many developed countries with greater social support and a socialized model of health care have achieved ambitious World Health Organization 90–90–90 care goals more than 5 years ago.35–37
Our study had limitations: enrollment targets were not met primarily due to the SARS-CoV-2 pandemic, there were high attrition rates leading to limited power to draw conclusions, and the results may not be generalizable to all settings. The proportion lost to follow-up highlights some of the challenges of research involving PWH-OOC. Strategies such as mobile research teams, collaboration with homeless shelters, public health and primary care, and finding reliable communication methods between participants and research team would potentially improve study retention. Strengths included the randomized prospective design with prespecified outcomes and rich baseline HIV and sociostructural data. This likely leads to higher quality outcome data compared with similar studies reporting observational outcomes only.
In summary, this study did not find evidence that the InstaCare complex intervention improved HIV viral suppression or engagement in care after 24 weeks among PWH-OOC compared with a time-and attention control condition. Low reengagement in care rates would suggest that a substantial shift in healthcare/social care provision would be required to improve the HIV care cascade in San Diego. Interventions that combine multimodality structural changes including mobile HIV care, easy access to stable housing, low-barrier mental health care, proactive medication-assisted treatment, and novel HIV therapeutics are likely required in combination to impact HIV care outcomes. Future work should evaluate the impact of these new strategies on improving HIV suppression rates.
ACKNOWLEDGMENTST.C.S.M., L.R.S., C.A., and S.J.L. all contributed to the study conception, design, performance, data analysis, and manuscript preparation.
REFERENCES 1. Centers for Disease Control and Prevention. HIV Surveillance Report, 2020; vol 33. 2022. Available at: http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html. Accessed June 1, 2023. 2. Marks G, Crepaz N, Janssen RS. Estimating sexual transmission of HIV from persons aware and unaware that they are infected with the virus in the USA. AIDS. 2006;20:1447–1450. 3. Li Z, Purcell D, Sansom S, et al. Vital signs: HIV transmission along the continuum of care - United States, 2016. MMWR Morb Mortal Weekly Rep. 2019;68:267–272. 4. Centers for Disease Control and Prevention. Monitoring selected national HIV prevention and care objectives by using HIV surveillance data—United States and 6 dependent areas, 2019. In: HIV Surveillance Supplemental Report 2021. Vol 26, No. 2. Available at: http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html. Accessed June 1, 2023. 5. U.S. Department of Health and Human Services. Ending the HIV Epidemic in the U.S; 2019. Available at: https://www.hiv.gov/federal-response/ending-the-hiv-epidemic/overview. Accessed June 1, 2023. 6. Cohen MS, Chen YQ, McCauley M, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365:493–505. 7. Dombrowski JC, Galagan SR, Ramchandani M, et al. HIV care for patients with complex needs: a controlled evaluation of a walk-in, incentivized care model. Open Forum Infect Dis. 2019;6:ofz294. 8. Imbert E, Hickey MD, Clemenzi-Allen A, et al. Evaluation of the POP-UP programme: a multicomponent model of care for people living with HIV with homelessness or unstable housing. AIDS. 2021;35:1241–1246. 9. Metsch LR, Feaster DJ, Gooden L, et al. Effect of patient navigation with or without financial incentives on viral suppression among hospitalized patients with HIV infection and substance use: a randomized clinical trial. JAMA. 2016;316:156–170. 10. Shacham E, López JD, Brown TM, et al. Enhancing adherence to care in the HIV care continuum: the barrier elimination and care navigation (BEACON) Project evaluation. AIDS Behav. 2018;22:258–264. 11. Bean MC, Scott L, Kilby JM, et al. Use of an outreach coordinator to reengage and retain patients with HIV in care. AIDS Patient Care STDS. 2017;31:222–226. 12. Swygard H, Seña AC, Mobley V, et al. Implementation of the North Carolina HIV bridge counseling program to facilitate linkage and reengagement in care for individuals infected with HIV/AIDS. N C Med J. 2018;79:210–217. 13. Mulatu MS, Hoyte T, Williams KM, et al. Cross-site monitoring and evaluation of the Care and Prevention in the United States Demonstration Project, 2012-2016: selected process and short-term outcomes. Public Health Rep. 2018;133:87s–100s. 14. Wohl AR, Dierst-Davies R, Victoroff A, et al. Implementation and operational research: the navigation program: an intervention to reengage lost patients at 7 HIV clinics in Los Angeles county, 2012–2014. J Acquir Immune Defic Syndr. 2016;71:e44–e50. 15. Maulsby C, Positive Charge Intervention Team, Ch
Comments (0)