
Remember me


Cardiogenic shock (CS) is a life-threatening medical condition that occurs when, as a consequence of cardiac disease, the physiological interdependence between oxygen delivery and consumption is lost, leading to multiorgan failure.1 Despite significant advances in the management of cardiovascular diseases, CS remains a major cause of morbidity and mortality worldwide. Interestingly, variability in etiology, treatment, and outcomes have been reported, translating into an in-hospital mortality rate of 30%–50% in contemporary series,2–6 but this ranged from 2.2% to 62.5% as patients varied from less severe to more advanced shock stages.7 Several studies have been published, contributing to a better characterization of this clinical heterogeneity. However, the epidemiology of CS in Italy is still poorly described because of the lack of a robust and structured CS network, shared healthcare protocols, and electronic health record systems.8–10 The Altshock‐2 Registry, a multicenter prospective data collection with 11 Italian Centers contributing to patients' enrollment, started recruiting patients in March 2020 and is, to date, the only registry of patients with CS in Italy.11,12
The aim of this study is to analyze the clinical characteristics at admission, the clinical course, the treatments received, the outcomes observed, and their predictors in a series of consecutive patients with a diagnosis of CS admitted to an academic, high-volume, tertiary referral cardiac intensive care unit (CICU) in Italy.
METHODSThe Fondazione Policlinico Universitario Agostino Gemelli IRCCS (Rome, Italy) is a surgical/interventional tertiary center without an active heart transplant and left ventricular assist device (LVAD) program. The hospital has a CICU, a general intensive care unit, a postcardiac surgery intensive care unit, a neurological intensive care unit and a postoperative general ICU.
Electronic health records were retrospectively reviewed to identify cases of CS admitted to the CICU of the Fondazione Policlinico Universitario Agostino Gemelli IRCCS between January 1, 2020, and January 1, 2023.
The initial search was based on the International Statistical Classification of Diseases and Related Health Problems (ICD-9) code for CS (785.51) collected in our electronic health record system (Digistat, GE Healthcare). Two cardiologists performed a review to confirm the diagnosis of CS, and data abstraction from electronic health records for a database including demographic data, clinical characteristics, laboratory data, diagnostic test results, treatments received, and in-hospital outcomes and complications. Disagreements on findings or readings were resolved through discussion and consensus. For this analysis, we included patients with CS stage C or worse according to the Society for Cardiovascular Angiography and Interventions (SCAI) shock classification.13 In brief, SCAI SHOCK stage A includes stable patients with cardiac problems at risk for CS but failing to meet the preshock (stage B) or shock (stages C–E) criteria. Stage B represents patients who have evidence of hemodynamic instability (hypotension or compensatory tachycardia) without hypoperfusion (lactate level of <2 mmol/L); stage C represents the classic patients with CS who present with hypoperfusion (lactate level of >2 mmol/L) either untreated or requiring hemodynamic support through pharmacologic or mechanical intervention; stage D represents the failure of initial therapy and the need to add 1 or more additional vasoactive drugs or mechanical circulatory support devices; stage E is reserved for refractory shock with actual or impending cardiovascular collapse despite high and escalating levels of support (including arrest in progress). The CardShock risk score was calculated at admission and consists of 7 variables giving a maximum of 9 points [including age >75 years, confusion at presentation, history of previous acute myocardial infarction (AMI) or coronary bypass graft surgery, AMI-related CS, left ventricular ejection fraction (LVEF) <40%, blood lactate, kidney function].
Patients with alternative causes of shock (ie, hypovolemic, septic, hemorrhagic, obstructive), on antibiotic therapy before or at the time of the admission for suspected sepsis, and those who were candidates to palliative care because of other concomitant severe health conditions or patient's advanced directive were excluded from this study.
The aim of this study is to assess how the clinical characteristics at admission and the treatments received may affect the clinical course and the outcomes observed.
The primary outcome of interest was all-cause mortality. Secondary outcomes included resuscitated in-hospital cardiac arrest (defined as cardiac arrest occurring during the hospital stay with prompt resuscitation with chest compressions, defibrillation, or both), acute cerebrovascular accident (defined clinically and/or using brain imaging), deep vein thrombosis or pulmonary embolism (as documented using Doppler venous ultrasound or chest computed tomography scan), need for renal replacement therapy (ie, continuous renal replacement therapy for acute or worsening renal failure), major bleedings [defined according to the International Society on Thrombosis and Haemostasis as fatal bleeding, and/or symptomatic bleeding in a critical area or organ, such as intracranial, intraspinal, intraocular, retroperitoneal, intra-articular or pericardial, or intramuscular with compartment syndrome, and/or bleeding causing a fall in hemoglobin levels of 1.24 mmol/L (2 g/dL or greater) or more, or leading to a transfusion of 2 U or more of whole blood or red cells], delirium (defined as a disturbance of consciousness and cognition that develops over a short period of time and fluctuating over time with need of nonpharmacological and pharmacological interventions), need for endotracheal intubation, and infection (suspected or confirmed and needing antibiotic therapy).
Statistical AnalysisDescriptive statistics were used to describe the characteristics of the study participants. Continuous data were reported as median and interquartile range, and data were compared with the Mann–Whitney U test or Kruskal–Wallis test, as appropriate. Categorical variables were expressed as numbers and percentages (%) and compared using χ2 test or Fisher exact test, as appropriate. Correlations between clinical variables were determined by Spearman's correlation coefficients. A logistic regression analysis for in-hospital mortality was performed including clinically significant variables. Those meeting statistical significance in the univariable model (P < 0.05, 2-tailed) were further evaluated in the multivariable logistic regression model to identify independent variables associated with the occurrence of in-hospital mortality. For the univariable and multivariable analysis, the measure of association was expressed as an odds ratio (OR) and 95% confidence interval (CI). Receiver-operating characteristic (ROC) curve analysis was used to estimate the overall predictive accuracy of continuous variables of interest to define the optimal predictive cut-off value for in-hospital all-cause mortality by evaluating the area under the curve (AUC) and the respective 95% CI. All the analyses were completed using SPSS, version 29.0 (SPSS, Chicago, IL).
This study complies with the Declaration of Helsinki and was approved by the Catholic University Ethics Committee (protocol number ID 5285).
RESULTS Study PopulationA total of 141 consecutive patients were identified using the ICD-9 for CS (785.51). After reviewing electronic health records, 45 patients were considered ineligible for our study. Fourteen patients did not qualify for inclusion (SCAI stage lower than C during the whole hospital stay), and 31 presented at least 1 exclusion criterion (18 septic shock, 8 obstructive shock, and 5 patients opted for comfort measures).13 A final cohort of 96 patients with a confirmed diagnosis of CS SCAI stage C or worse was analyzed for this study.
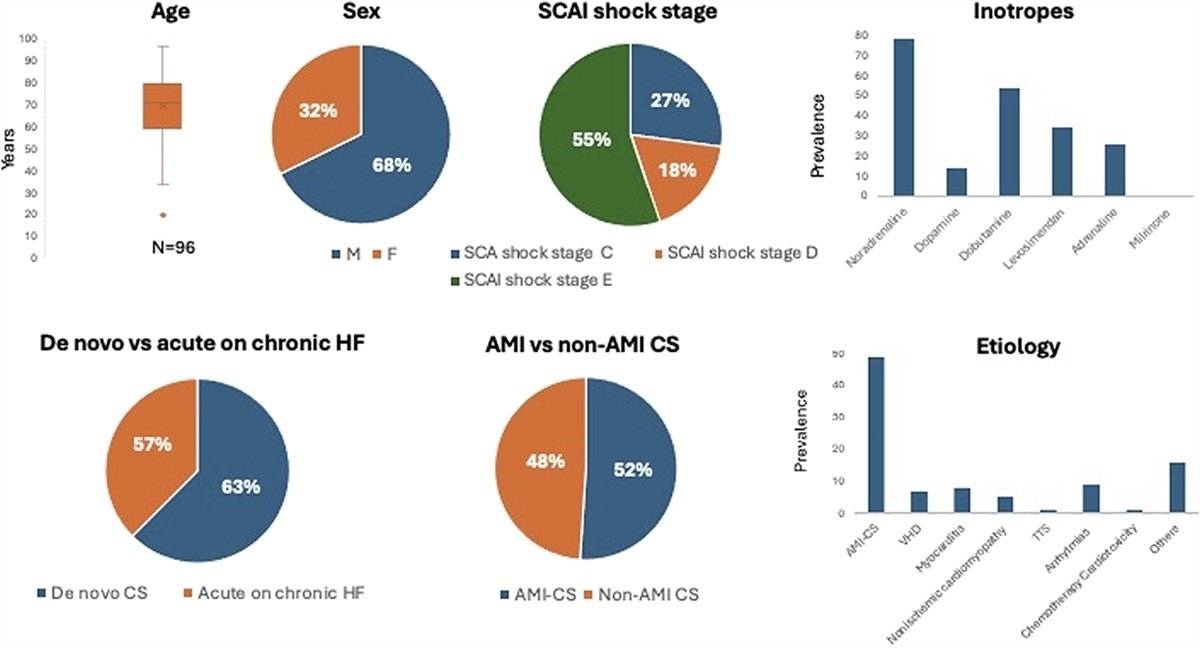
Baseline CharacteristicsBaseline demographic, clinical, laboratory, and echocardiographic data and treatments received are summarized in Table 1 and Figure 1. The median age was 71 years (interquartile range 60–79); 65 (68%) were men, and 91 (95%) were White. Clinical presentation was de novo CS in 60 patients and acute decompensation of chronic heart failure (ADHF) in 36 (63% vs. 37%, respectively). Etiology of CS was AMI in 49 patients (51%), valvular heart disease (VHD) in 7 (7%), nonischemic cardiomyopathy in 5 (5%), myocarditis in 8 (8%), Takotsubo syndrome in 1 (1%), life-threatening arrhythmias in 9 (9%), adverse reaction to chemotherapy in 1 (1%), and other causes in 16 patients (17%).
TABLE 1. - Baseline Characteristics of Patients Admitted With CS Variable Total (n = 96) Age (y) 71 [60–79] Sex (F), n (%) 31 (32) White 91 (95) Black 2 (2) Other 3 (3) BMI (kg/m2) 24 [22–27] Diabetes, n (%) 19 (20) COPD n (%) 19 (20) CKD, n (%) 17 (18) Active cancer n (%) 6 (6) CVA, n (%) 7 (7) Clinical presentation SCAI stage at admission, n (%) A 3 (3) B 30 (31) C 39 (41) D 16 (∼17) E 8 (8) Worst SCAI stage during the hospital stay, n (%) C 26 (27) D 17 (18) E 53 (55) CardShock risk score 4 (3–5) De novo cardiogenic shock, n (%) 60 (63) Acute on chronic heart failure, n (%) 36 (37) Etiologies, n (%) AMI-CS 49 (51) VHD 7 (7) Myocarditis 8 (8) Nonischemic cardiomyopathy 5 (5) TTS 1 (1) Arrhytmias 9 (9) Chemotherapy cardiotoxicity 1 (1) Other 16 (17) Laboratory data WBC 109/L 11.6 [7.7–15.5] CRP mg/L 31.0 [8.9–111.0] PCT ng/mL 3.0 [1.0–17.2] Lactic acid mmol/L 4.0 [1.9–7.0] TnI (peak) ng/L 28.5 [10.8–52.3] NTproBNP pg/mL 21,500 [1000–45,250] Echocardiography at admission LVEF (%) 25 [20–35] EDV (mL) 86 [65–101] LVOT VTI (cm) 11 [9–12] E/e′ 15 [13–22] TAPSE (mm) 14 [11–18] sPAP (mm Hg) 45 [35–55] In-hospital treatment Necessity of inotropes/vasopressors, n (%) 100 (100) Noradrenaline 79 (82) Dopamine 14 (15) Dobutamine 54 (56) Levosimendan 35 (37) Adrenaline 26 (27) Milrinone 1 (1) Necessity of temporary ventricular support device, n (%) 34 (35) IABP 18 (19) Impella 22 (23) ECMO 6 (6) Necessity of vasodilators, n (%) 16 (17) Necessity of diuretics, n (%) 82 (85) Treatment with high-dose corticosteroids, n (%) 8 (8) Pressure-support ventilation 41 (43) HFNC 10 (10) Both PSV and HFNC 4 (4)AS, aortic stenosis; BMI, body mass index; CKD, chronic kidney disease; CVA, cerebrovascular accident; ECMO, extracorporeal membrane oxygenation; EDV, end-diastolic volume; ESV, end-systolic volume; HFNC, high-flow nasal cannula; IABP, intra-aortic balloon pump; LVOT, left ventricular outflow tract velocity–time integral; NT proBNP, N-terminal pro-B-type natriuretic peptide; PCT, procalcitonin; sPAP, systolic pulmonary artery pressure; TTS, Takostubo syndrome; WBC, white blood cell count.
 FIGURE 1.:
FIGURE 1.: Clinical characteristics of the population cohort of patients with CS. This figure illustrates the demographic characteristics (age, sex, comorbidities), the clinical presentations on admission according to the SCAI shock stage, the etiology, and the treatments administrated in our cohort of patients with CS.
SCAI stage at admission was A in 3 (3%), B in 30 (31%), C in 39 (41%), D in 16 (∼17%), and E in 8 patients (8%). The median Card Shock risk score was 4 [3–5]. The Sequential Organ Failure Assessment score within 24 hours was 8 [6–9].
The median LVEF was 25 [20–35] % with a median left ventricular outflow tract velocity–time integral of 11 [9–12] cm and a median E/e' average ratio of 15 [13–22].
Lactate levels at admission were 4 [1.9–7] mmol/L, median C-reactive protein (CRP) at admission was 31.0 [8.9–111.0] mg/L, and white blood cell counts were 11.6 [7.7–15.5] 109/L.
Clinical Course and Treatment ReceivedThe hospital length of stay was 11.52–20 days. During the hospital stay, 26 patients (27%) progressed to SCAI stage C, 17 (18%) to stage D, and 53 (55%) to SCAI stage E. All patients required inotropes and/or vasopressors as detailed in Table 1. In particular, dobutamine and levosimendan were the most frequently used inotropes [adopted in 54 (56%) patients and 35 (37%) patients, respectively] and noradrenaline the most frequently used vasopressor [adopted in 79 (82%) patients]. Most patients received diuretics [82 (85%)], while only 16 (17%) patients required vasodilators and 8 (8%) patients high-dose corticosteroids. Mechanical circulatory support was required in 34 patients (35%), including 18 (19%) intra-aortic balloon pump, 22 (23%) percutaneous LVAD [p-LVAD (Impella CP; Abiomed)], and 6 (6%) venous-arterial extracorporeal membrane oxygenation. A pulmonary artery catheter was used in 15 (16%) of patients for invasive hemodynamic monitoring.
Study OutcomesAll-cause in-hospital mortality occurred in 45 (47%) patients, of whom 1 (2%) patient had presented with SCAI stage A, 10 (22%) patients with SCAI stage B, 18 (40%) with SCAI stage C, 12 (27%) with SCAI stage D, and 4 (9%) with SCAI stage E at admission.
Regarding the secondary outcomes of interest, cardiac arrest occurred in 45 patients (47%), infection in 55 (57%) patients, major bleedings in 9 (9%) patients, delirium occurred in 14 (15%) patients, and deep venous thrombosis or pulmonary embolism in 3 (3%) patients. Furthermore, 20 (20%) patients needed renal replacement therapy and 48 (50%) patients needed endotracheal intubation (Fig. 2).
 FIGURE 2.:
FIGURE 2.: Prevalence of in-hospital complications among patients with CS. This figure illustrates the distribution of in-hospital complications among our population cohort of patients with CS and survivors versus nonsurvivors.
The characteristics of survivors (Ss) versus nonsurvivors (NSs) are summarized in Table 2. In brief, NSs were older [median age 75 (63–82) years vs. 69 (56–75) years; P = 0.019], had a higher prevalence of chronic obstructive pulmonary disease (COPD) [13 (29%) vs. 6 (12%), P = 0.036], presented higher levels of white blood cell at admission [13.4 (8.1–18.9) 109/L vs. 9.5 (7.3–14.2) 109/L, P = 0.019], CRP [60 (27.0–128.5) mg/L vs. 7.7 (2.8–31.0) mg/L, P < 0.001], procalcitonin [1.8 (0.4–5.5) ng/mL vs. 0.2 (0.05–0.31) ng/mL, P < 0.001], N-terminal pro-BNP type natriuretic peptide (NT-pro BNP) [13,037 (8129–31,935) pg/mL vs. 9220 (4311–20,199) pg/mL, P = 0.043], and lactate [6 (3.0–9.8) mmol/L vs. 3 (1.8–4.8) mmol/L, P = 0.001] at admission, and showed a higher increase in lactate levels at 24–48 hours from admission (delta with baseline lactate levels) [+2.25 (−1.5; 5) vs. −1.05 (−2.8; 0.0), P = 0.001]. NSs had a worse SCAI stage at hospital admission (P < 0.001), a more depressed right ventricular (RV) function, assessed by tricuspid annular plane systolic excursion (TAPSE) [12 (10–15) mm vs. 18 (12–19) mm, P < 0.001], and a higher estimated left ventricular filling pressure assessed by the average E/e′ ratio [21 (18–25) vs. 14 (11–18), P < 0.001]. NSs had a higher CardShock risk score [5 (3.5–6) vs. 3 (2.8–4), P < 0.001].14
TABLE 2. - Baseline Characteristics in Survivors Versus Nonsurvivor Patients With CS Survivors (n = 51) Nonsurvivors (n = 45) P Age (y) 69 [56–75] 75 [63–82] 0.019 Sex (F), n (%) 14 (27) 17 (38) 0.280 BMI (kg/m2) 25 [23–27] 24 [21–26] 0.316 Diabetes, n (%) 10 (20) 9 (20) 0.962 COPD, n (%) 6 (12) 13 (29) 0.036 CKD, n (%) 9 (18) 8 (18) 0.987 Active cancer—n (%) 3 (6) 3 (7) 1.000 CVA—n (%) 2 (4) 5 (11) 0.247 Clinical presentation SCAI stage—at admission, n (%) 0.083 A 2 (4) 1 (2) B 20 (39) 10 (22) C 21 (42) 18 (40) D 4 (8) 12 (27) E 4 (8) 4 (9) Worse SCAI stage, n (%) <0.001 C 26 (51) 0 (0) D 17 (33) 0 (0) E 8 (16) 45 (100) CardShock risk score 3 (2.8–4) 5 (3.5–6) <0.001 No previous history of heart disease, n (%) 15 (29) 21 (47) 0.081 Etiologies, n (%) 0.513 AMI-CS 24 (47) 23 (51) VHD 3 (6) 2 (4) Myocarditis 6 (12) 2 (4) Nonischemic cardiomyopathy 3 (6) 2 (4) 0.817 TTS 0 (0) 1 (2) 0.888 Arrhythmias 6 (12) 5 (11) 0.504 Chemotherapy cardiotoxicity 1 (2) 0 (0) 0.888 Other 8 (16) 8 (18) 0.660 Laboratory test WBC 109/L 9.5 [7.3–14.2] 13.4 [8.1–18.9] 0.019 CRP mg/L 7.7 [2.8–31.0] 60.0 [27.0–128.5] <0.001 PCT ng/mL 0.2 [0.05–0.31] 1.80 [0.4–5.5] <0.001 Lactic acid mmol/L 3.0 [1.8–4.8] 6.00 [3.0–9.8] 0.001 TnI (peak) ng/L −1.05 [−2.8 to 0.0] +2.25 [−1.5 to 5.0] <0.001 NTproBNP pg/mL 3719 [254.5–40,109.0] 6648 [224.7–36,801.5] 0.848 WBC 109/L 9220 [4311–20,199] 13,037 [8129–31,935] 0.043 Echocardiography at admission LVEF (%) 25 [20–35] 25 [19–39] 0.734 EDV (mL) 80 [62–103] 87 [58–100] 0.713 LVOT VTI (cm) 11 [9–15] 10 [9–11] 0.076 E/e′* 14 [11–18] 21 [18–25] <0.001 TAPSE (mm) 18 [12–19] 12 [10–15] <0.001 sPAP (mm Hg) 45 [30–54] 50 [45–60] 0.055 In-hospital treatment Necessity of temporary ventricular support device, n (%) 18 (35) 16 (36) 0.979 Necessity of vasodilators, n (%) 11 (22) 5 (11) 0.170 Treatment with high-dose corticosteroids, n (%) 5 (10) 3 (7) 0.197*E/e′ was missing in 13 patients.
AS, aortic stenosis; BMI, body mass index; CKD, chronic kidney disease; CVA, cerebrovascular accident; EDV, end-diastolic volume; ESV, end-systolic volume; HFNC, high-flow nasal cannula; IABP, intra-aortic balloon pump; LVOT, left ventricular outflow tract velocity–time integral; NT proBNP, N-terminal pro-B-type natriuretic peptide; PCT, procalcitonin; sPAP, systolic pulmonary artery pressure; TTS, Takostubo syndrome; WBC, white blood cell count.
Moreover, they presented more often a resuscitated in-hospital cardiac arrest [37 (82%) vs. 8 (16%), P < 0.001], the necessity of endotracheal intubation [31 (69%) vs. 17 (33%), P = 0.001], and a lower rate of delirium compared with Ss [3 (7%) vs. 11 (22%), P = 0.046]. On the contrary, no differences were found among Ss versus NSs in the etiologies of CS (P > 0.05), in LVEF values (P = 0.734), in the inotropes/vasopressors used, or in the necessity of temporary ventricular support [Ss 18 (33%) vs. NSs 16 (36%), P = 0.979], as well as in transient ischemic attack/stroke, deep venous thrombosis or pulmonary embolism, kidney failure requiring renal replacement therapy, major bleedings, and infection rate. The results are summarized in Table 3.
TABLE 3. - In-Hospital Complications in Survivors and Nonsurvivor Patients Survivors (n = 51) Nonsurvivors (n = 45) P Resuscitated IHCA, n (%) 8 (16) 37 (82) <0.001 Stroke or TIA, n (%) 2 (4) 3 (7) 0.663 DVT or PE, n (%) 1 (2) 2 (2) 0.598 Endotracheal intubation, n (%) 17 (33) 31 (69) 0.001 Major bleedings, n (%) 3 (6) 6 (13) 0.297 Delirium, n (%) 11 (22) 3 (7) 0.046 Infection needing antibiotics, n (%) 28 (55) 27 (60) 0.614 Continuous dialysis, n (%) 9 (18) 11 (24) 0.413 Acute kidney injury, n (%) 11 (22) 18 (40) 0.041DVT, deep vein thrombosis; IHCA, in-hospital cardiac arrest; PE, pulmonary embolism; TIA, transient ischemic attack.
At univariate logistic regression, age, lactate levels at admission, lactate increase in the first 48 hours, CRP levels at admission, and TAPSE were predictors of in-hospital death for all causes (Table 4).
TABLE 4. - Variables Associated With In-Hospital Mortality by Univariate and Multivariate Logistic Regression Analysis Variables Univariable Analysis Multivariable Analysis OR (95% CI) P OR (95% CI) P Age (y) 1.04 [1.01–1.08] 0.010 1.09 [0.99–1.22] 0.091 Lactate levels (mmol/L) 1.23 [1.08–1.39] 0.002 3.49 [1.59–7.63] 0.020 Delta lactate 1.17 [1.04–1.32] 0.009 2.8 [1.37–5.75] 0.005 NTproBNP (pg/mL) 1.00 [1.00–1.00] 0.161 CRP (mg/L) 1.01 [1.01–1.02] 0.001 1.03 [1.00–1.04] 0.027 WBC (109/L) 1.07 [0.99–1.16] 0.063 PCT (ng/mL) 1.13 [0.93–1.37] 0.212 TAPSE (mm) 0.81 [0.72–0.92] 0.001 0.79 [0.59–1.04] 0.091NT proBNP, N-terminal pro-B-type natriuretic peptide; PCT, procalcitonin; WBC, white blood cell count.
At multivariate analysis, lactate levels at admission [OR 3.49 per unit in increase mmol/L (1.59–7.63), P = 0.02], lactate increase in the first 48 hours [OR 2.8 per unit in increase mmol/L (1.37–5.75), P = 0.005], and CRP levels at admission [OR 1.03 per unit in increase mg/L (1.00–1.04), P = 0.027] remained independent predictors of in-hospital death for all causes. The E/e′ ratio was not included in the analysis because it was missing in 13 patients (Table 4).
ROC curve analysis was performed to assess the ability of CRP at admission to predict in-hospital mortality. The AUC for CRP levels to predict in-hospital mortality was 0.793 (P < 0.01; Fig. 3). The optimal cut-off was identified using the Youden method and was found to be a CRP cut-off value of 25 mg/L (sensitivity of 82% and specificity of 64%). Of note, 50 (52%) of the patients had CRP on presentation ≥25 mg/L. In-hospital mortality occurred in 9 (20%) patients with CRP levels <25 mg/L and 36 (72%) patients among those with CRP levels equal or above the cut-off value (P < 0.001). Table 5 summarizes the clinical, laboratory, and echocardiographic data of the overall population divided for the cut-off of CRP of ≥25 mg/L. We did not find a significant correlation between lactic acid level at admission and CRP levels (R = +0.175, P = 0.101); however, we found a moderate correlation between delta interval changes in lactic acid levels and CRP at admission (R = +0.326, P = 0.01), with higher levels of CRP at admission correlating with higher lactate increases (Fig. 4).
 FIGURE 3.:
FIGURE 3.: ROC curve analysis for CRP to predict in-hospital complications. ROC curve analysis showed an AUC for CRP levels to predict in-hospital mortality of 0.793 (P < 0.01).
TABLE 5. - Baseline Characteristics and Treatments Received According to the Cut-Off Value of CRP CRP <25 mg/L (n = 46) CRP ≥25 mg/L (n = 50) P Age (y) 68 [58–75] 71 [58–79] 0.596 Sex (F), n (%) 15 (33) 16 (32) 0.949 BMI (kg/m2) 24 [23–28] 23 [21–26] 0.381 Diabetes, n (%) 12 (26) 7 (14) 0.138 COPD, n (%) 11 (24) 8 (16) 0.331 CKD, n (%) 11 (24) 6 (12) 0.127 Active cancer n (%) 2 (4) 4 (8) 0.679 CVA, n (%) 3 (6) 4 (8) 1.000 Clinical presentation Worse SCAI stage, n (%) <0.001 C 22 (48) 4 (8) D 10 (22) 7 (14) E 14 (30) 39 (78) Card shock 4 (3–4) 5 (3–5.2) 0.07
Comments (0)