
Remember me


A seven-year-old male was referred to our Medical Genetics consultation for etiological investigation, given NF1 suspicion. He is the only child of a non-consanguineous couple born at term with normal measurements after an uneventful pregnancy. His mother and maternal grandmother were clinically diagnosed with NF1. In the first year of life, he presented with several CAL spots and later axillary freckling. Brain magnetic resonance imaging (MRI) performed at four years old showed multiple areas of T2/FLAIR hyperintensity in the cerebellum, hippocampus, globus pallidus, and thalamus, typical of NF1.
At six years old, he developed facial asymmetry involving the tongue (Fig. 1) associated with redness, ptosis, and tearing of the left eye with chewing movements (Marcus Gunn phenomenon). An updated brain MRI revealed a plexiform neurofibroma in the right maxillofacial area with an infiltrative lesion involving the peri-auricular region, external auditory canal, submandibular and sublingual spaces, and right half of the tongue. Maxillofacial surgeons considered the neurofibroma inoperable.
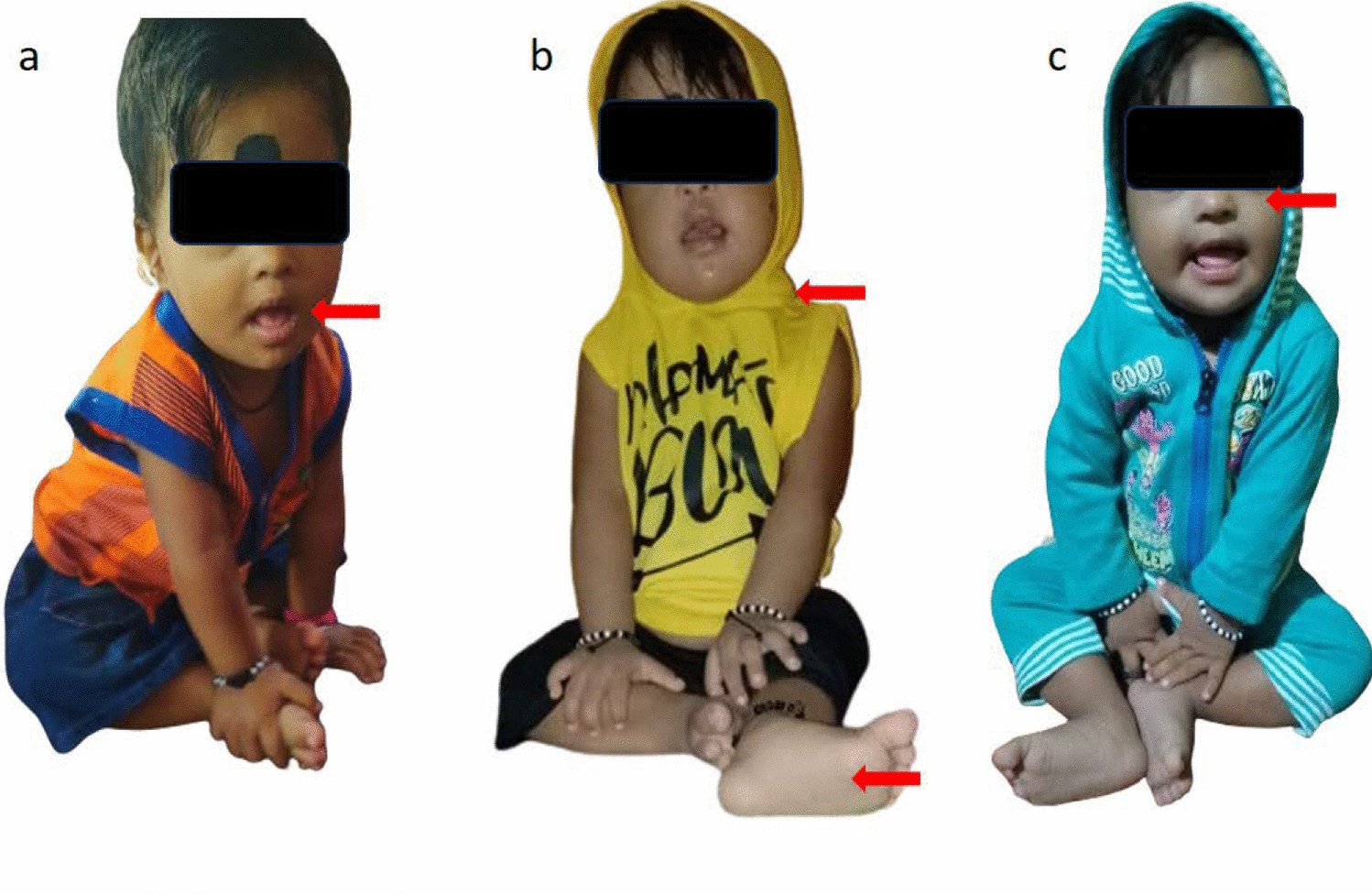
Fig. 1
Male patient with neurofibromatosis type 1 (NF1) and 16p13.11 duplication showing facial and tongue asymmetry as a consequence of a neurofibroma plexiform, as two café-au-lait macules in the right frontal region, a broad forehead, short nose, and low-set, posteriorly rotated ears. His facial features are also coarser than expected for typical NF1/RASopathy dysmorphic features, what elicited additional studies that unravel the identification of a 16p13.11 duplication contributing to the phenotype
In our observation at the age of seven, he presented with more than six CAL spots, axillary freckling, facial and tongue asymmetry, and RASopathic dysmorphic features: a broad forehead, short nose, and low-set posteriorly rotated ears (Fig. 1). In addition, he presented with bilateral earlobe creases and coarser facial features than those expected of NF1. He presented with macrocephaly (percentile > 97th), a common feature in patients with NF1, and obesity, with a body mass index of 27 kg/m2 (percentile > 97th). His behavior was hyperkinetic, with the Conners comprehensive behavior rating scale being diagnostic of attention-deficit hyperactivity disorder and the Griffith Mental Developmental Scale, revealing borderline development with a global developmental quotient of 72. Ophthalmologic, cardiac, and abdominal ultrasound evaluations were normal.
Comments (0)