Nonsynonymous genetic variants within the MTRR gene play a crucial role in regulating the activity of methionine synthase, which may have protective or detrimental effects on the risk of congenital heart diseases (CHDs) [21]. Previous studies have indicated a potential association between MTRR gene variants and conditions such as atrial septal defect (ASD) and patent ductus arteriosus (PDA) in the Han Chinese population [22].
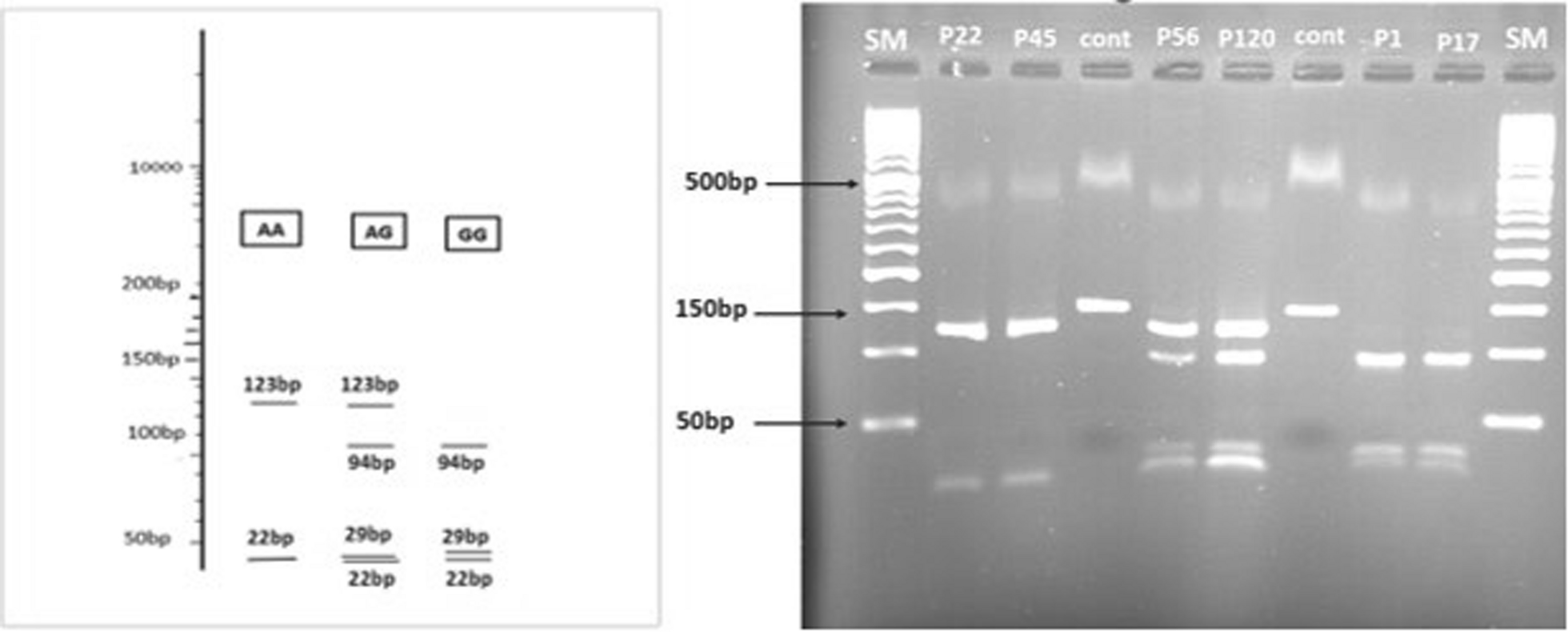
The analysis of the A66G gene polymorphism revealed statistically significant differences between ACHD patients and controls in terms of genotypes, alleles, and both dominant and recessive models. In both the co-dominant and recessive models, the homozygous GG genotype showed a significant association with ACHD (OR = 4.022, P < 0.001 and OR = 3.154, P < 0.001, respectively). Under the dominant model (AA vs. AG + GG), the combined AG and GG genotypes were also significantly associated with ACHD. Regarding the C524T gene polymorphism, in the co-dominant model using the homozygote wild-type genotype (CC) as a reference, the homozygous TT genotype was significantly associated with ACHD, showing a fourfold increase in risk (OR = 4.708, P < 0.001), while the heterozygous CT genotype also showed a significant association (OR = 2.211, P = 0.026). In the dominant model (CC vs. CT + TT), the combined heterozygous CT and homozygous TT genotypes demonstrated a threefold increased risk compared to the homozygous CC genotype (OR = 3.158, P < 0.001). The recessive model further indicated a significantly higher risk for the homozygous TT genotype when compared to the combined CC and CT genotypes (OR = 2.867, P < 0.001). Allele analysis also showed that the 524T allele frequency was notably higher in cases than in controls, with more than a twofold increase in the risk of ACHD (OR = 2.493, P < 0.001).
These findings are consistent with the study by Yu et al., which investigated the association between the MTRR (A66G) polymorphism and the risk of CHDs in various ethnic groups. Their study reported a significant association of the homozygous GG genotype with CHDs (GG vs. AA: OR = 1.332; P = 0.035) and the G allele with a higher risk of CHDs. Subgroup analyses found that the G allele was significantly associated with CHDs in Asian populations but not in Caucasians [24].
Moreover, Zeng et al. also observed that the 66GG and 524CT genotypes were linked to a moderately higher risk of ACHD. While no significant differences in the frequency of the 524TT genotype between cases and controls were noted, they found that the 524T allele was more frequent in ACHD patients than in controls. This discrepancy may be due to the rarity of the 524TT genotype in their sample or a small sample size, which might have limited the ability to detect significant differences [22].
Additionally, a study by Noori et al. linked the A66G polymorphism of the MTRR gene to CHD, with both heterozygote and homozygote mutant genotypes strongly associated with the condition. However, the G allele itself was not significantly associated with CHD in their study [9]. On the other hand, the A66G polymorphism did not show a significant association with the prevalence of CHDs in the Han Chinese and Caucasian populations in the Netherlands [25, 26]. These variations across studies may reflect ethnic differences, as the relationship between MTRR gene polymorphisms and CHD is likely influenced by genetic background [27].
Furthermore, we found significant differences in the distributions of several combined genotypes between ACHD patients and controls. Using the combined homozygous CC/AA genotype as a reference, the AG/CT (OR = 3.942, P = 0.027), GG/CT (OR = 8.225, P = 0.002), AA/TT (OR = 4.396, P = 0.021), AG/TT (OR = 5.644, P = 0.007), and GG/TT (OR = 15.006, P < 0.001) combinations were significantly associated with ACHD. In contrast, the AG/CC (P = 0.996), GG/CC (P = 0.073), and AA/CT (P = 0.431) combinations did not show significant associations. This finding aligns with Zeng et al., who demonstrated that combined genotypes such as 66AA/524CT, 66AG/524CT, and 66GG/524CT were significantly more common in ACHD patients than controls, with an increased risk of ACHD [28].
Su and Li also found that the frequencies of the combined 66AG/524CT and 66GG/524TT genotypes in VSD patients were significantly higher than in controls, correlating with an increased risk of VSD (OR = 2.937 and 5.344, respectively) [27].
To our knowledge, this is the first study to examine different gene polymorphisms in various acyanotic heart diseases in Egyptian children. In this study, the AG genotype was a significant predictor of ASD (OR = 2.55, 95% CI = 1.03–6.33), while the GG genotype was a significant predictor of VSD (OR = 3.28, 95% CI = 1.5–7.15), ASD (OR = 5.43, 95% CI = 2.07–13.79), and pulmonary stenosis (PS) (OR = 4.19, 95% CI = 1.13–15.51). The CT genotype was a significant predictor of PDA (OR = 5.05, 95% CI = 1.02–25.06), while the homozygous TT genotype was a significant predictor of VSD (OR = 5.61, 95% CI = 2.12–14.84), ASD (OR = 3.2, 95% CI = 1.3–7.85), and PDA (OR = 5.67, 95% CI = 1.09–29.62). These findings are consistent with those of Zeng et al., who found a higher frequency of the homozygous 66GG genotype in PDA and a greater frequency of the heterozygous 524CT genotype in VSD and PDA than in controls [10].
The mechanisms by which MTRR polymorphisms contribute to CHDs remain unclear. It is hypothesized that elevated homocystein levels resulting from MTRR dysfunction may lead to endothelial dysfunction, inflammation, and oxidative stress, which could disrupt normal heart development. Additionally, impaired folate metabolism may affect critical DNA synthesis and methylation processes essential for fetal development and organogenesis.
Limitations
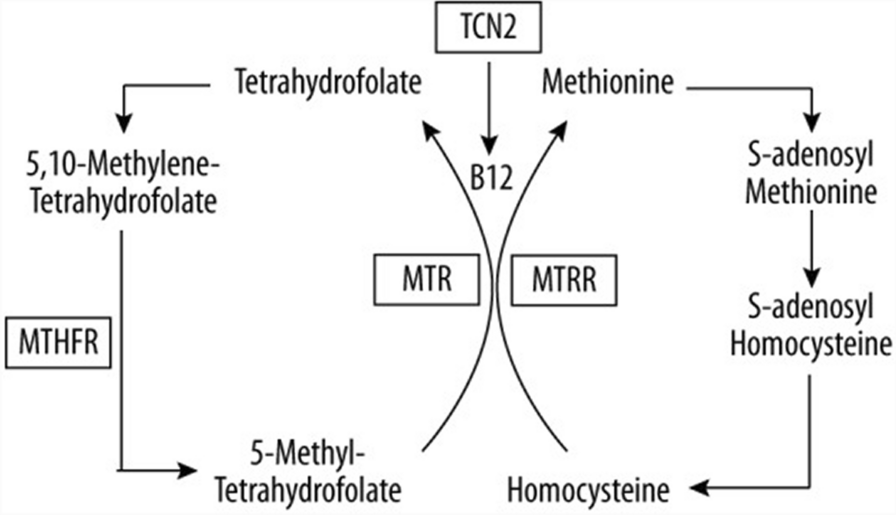
Non-random mating within the study population may have influenced genotype distributions and allele frequencies, potentially affecting the observed associations. Future studies with larger and more genetically diverse populations are necessary to address this potential source of bias and further validate our findings. Additionally, a more comprehensive study including three key genes in folate/ homocystein metabolism—methionine synthase (MTR), methionine synthase reductase (MTRR), and methylenetetrahydrofolate reductase (MTHFR)—is required, as the inclusion of only two SNPs may not entirely capture the genetic complexity of structural heart abnormalities. In addition, testing of homocystien levels in these patients may offer better insight into pathogenesis. Moreover, the impact of consanguinity on genotype distribution and other untested factors such as TORCH screening may limit the generalizability of the results.
Furthermore, some acyanotic heart diseases, such as aortic stenosis or coarctation, were not represented in our sample, which could also influence the results.



Comments (0)