Generally, more than half of the patients with HPBC benefit from anti-HER2 treatment, especially trastuzumab, but many patients show resistance to these treatments, which is a major clinical problem [22]. Resistance to therapies in HPBC remains a challenge in the current management of these patients [23]. Many molecular mechanisms have been proposed as potential causes of such resistance. Noninvasive biomarkers, such as blood testing of gene polymorphisms in HER2, apoptosis/cell cycle machinery (CCND1), and ATP-binding cassette B1 (ABCB1), have been proposed as potential predictors of the clinical outcomes in HPBC patients receiving trastuzumab [24].
In the current study, we investigated the significance of HER2 rs1136201 variants as a predictor of the response to trastuzumab in 122 HPBC patients who received trastuzumab therapy and were clinically monitored for therapeutic response. Our primary finding was that there was a considerable relationship between HER2 rs1136201 polymorphism and the response to trastuzumab. The rs1136201 polymorphism in the HER2 gene has been extensively studied for its potential link to breast cancer risk, yielding different and sometimes contradictory results.
Several meta-analyses have reported a significant association between this polymorphism and a heightened risk of breast cancer, particularly among Asian and African populations [25, 26]. Substitution A by G in this polymorphic site results in the replacement of Ile by Val at position 655 of the HER2 protein, which appears to pose a greater risk of trastuzumab resistance than Ile [25]. However, some studies, including one conducted in a Brazilian population, have failed to find a significant correlation [27]. This contradictory evidence indicates that while some research suggests a connection between rs1136201 and breast cancer risk, especially within certain ethnic groups, other studies do not corroborate these findings.
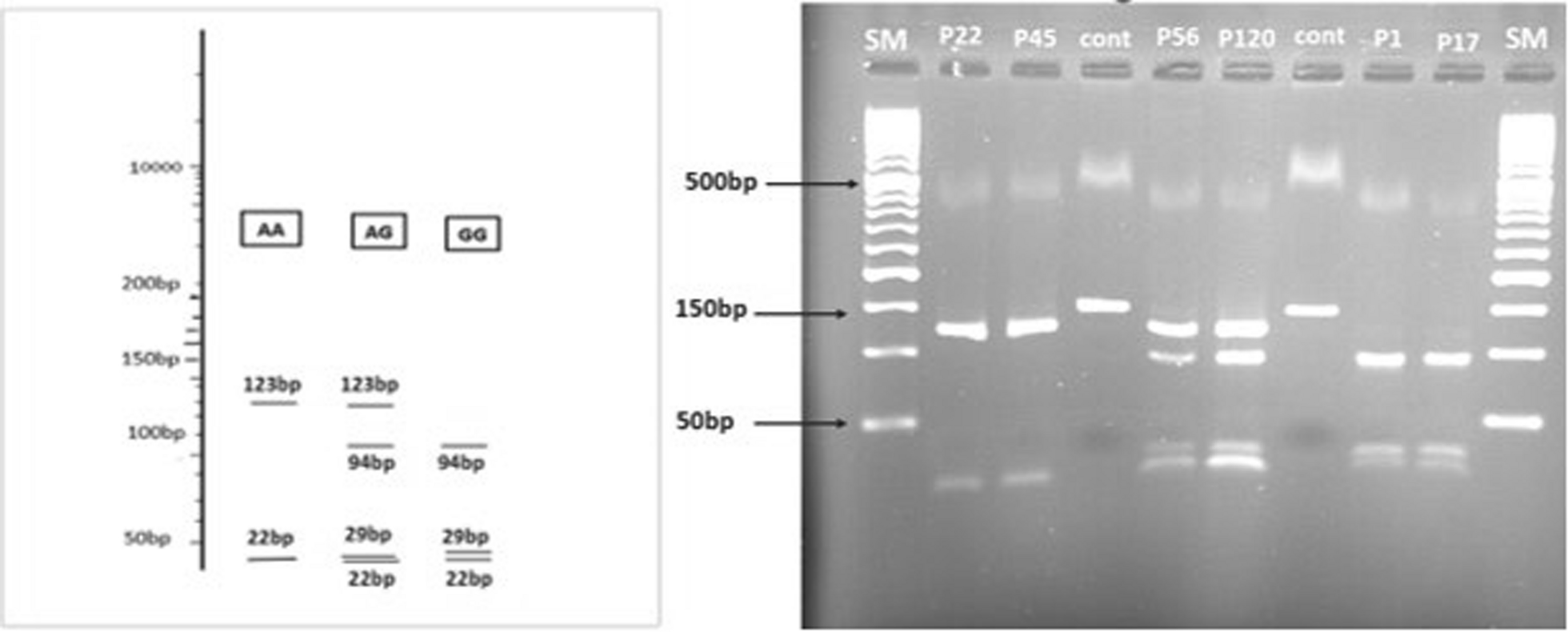
The HER2 gene is subject to somatic mutations and germinal polymorphism. The most investigated germinal polymorphism at the clinical level concerns codon 655 GTC/valine to ATC/isoleucine, transmembrane domain of the HER2 protein. The allele frequency for the Val form was found to be significant in Caucasians and variable among different populations [28]. The overall frequency of the G (Val) allele in our study patients was 14.9%. Interestingly, this variant has previously been reported to have a prevalence of approximately 13% in South Asian populations, suggesting a potential inherent genetic background that may contribute to trastuzumab non-responsiveness in this region. According to our results, about 55% (67/122) of patients with HPBC were sensitive to trastuzumab treatment. In contrast, the others developed metastasis and recurrence after receiving trastuzumab therapy and exhibited resistance to the drug. Additionally, the risk of metastasis or recurrence was higher in patients with AG and GG genotypes than in those with AA genotypes. Patients with a HER2 score of 3+ or lymph node involvement were also at increased risk of metastasis or recurrence. Most of the studies conducted on this polymorphism are related to the risk of breast cancer and cardiotoxicity caused by trastuzumab, and only a few studies have been conducted on the relationship between this polymorphism and the response to trastuzumab [28,29,30].
Regarding HER2 polymorphisms, our patients with the Ile/Val or Val/Val genotype had significantly worse PFS than those with the Ile/Ile genotype. Nevertheless, other researchers have described interesting albeit controversial results for this polymorphism regarding patient survival. Furrer et al. detected HER2 Ile655Val and Ala1170Pro polymorphisms by TaqMan assay and gathered clinicopathologic and survival data from medical records of 236 non-metastatic HPBC patients who had been treated with trastuzumab [31]. They reported that there was no association between alcohol consumption during trastuzumab treatment and disease-free survival (DFS). However, concerning HER2 polymorphisms, patients with the Ile/Val or Val/Val genotype had a significantly worse DFS than those with the Ile/Ile genotype [31]. There are contradictions among previous studies regarding the association between the HER2 Ile655Val polymorphism and trastuzumab response. These discrepancies may be due to differences in study design, sample size, patient ethnicity, clinical characteristics, treatment regimens, or genotyping methods. Such inconsistencies highlight the need for larger, well-designed, and multi-ethnic studies to clarify the true clinical significance of this polymorphism in predicting trastuzumab response [28, 29]. Han et al. surveyed the relationship between the HER2 Ile655Val polymorphism and clinical outcomes in women with HER2-negative breast cancer (HNBC) and in those with HPBC who either received trastuzumab or did not. Among 212 HPBC patients who underwent chemotherapy with trastuzumab, it was found that those with Val/Ile or Val/Val genotype had significantly better DFS and distant disease-free survival (DDFS) compared to those with Ile/Ile genotype [21]. Our results are consistent with Furrer’s findings and contrast with Han’s conclusions. Studies have revealed that substituting isoleucine for valine at position 655 might increase the tumorigenic potential of breast cancer cells because it predisposes HER2 as a receptor to assume an active conformation, leading to enhanced activity of the tyrosine kinase domain.
Novillo et al. reported that after 6 months of neoadjuvant anti-HER2 therapy (by trastuzumab or pertuzumab) and chemotherapy, 30% of the patients achieved a pathologic complete response (pCR). The HER2 rs1058808 polymorphism was significantly more prevalent among good homozygous responders for the variant allele. In contrast, the BARD1 rs2070096 polymorphism was associated with a higher pCR rate in both homozygous and heterozygous carriers. In this study, contrary to our results, no significant correlation was observed between the rs1136201 polymorphism and response to treatment. In addition, the association between the studied SNPs and survival was not reported due to the low mortality observed (five-year survival 87.02%; 95% confidence interval: 68.98–95.95) [11].
Damien Cote’s study involving 32 women with HPBC identified six notable SNPs across the exomes of 28 genes. The HER2 rs1136201, ERBB3 rs2229046, and rs773123 SNPs were strongly associated with poorer relapse-free survival (RFS) in patients treated with docetaxel, carboplatin, and trastuzumab (TCH)-based therapy, as opposed to those receiving non-TCH regimens. In this study, similar to our findings, patients who were heterozygous for the HER2 rs1136201 were significantly more likely to relapse in patients treated with TCH regimens than those who received non-TCH regimens [32].
In G. A. Milano’s study, genomic DNA from 57 advanced breast cancer patients undergoing trastuzumab treatment, mostly with paclitaxel, was analyzed for the Val655Ile polymorphism. This study found no significant correlation between the HER2 genotype and treatment outcomes like objective response rate, DFS (median, months: 21 for Val/Ile + Val/Val and 18 for Ile/Ile), while median PFS for genotypes in our study was higher [33].
Our finding aligns with studies by Furrer et al. and Damien Cote, suggesting that specific polymorphisms in the HER2 gene are linked to poorer outcomes in HPBC. However, this contrasts with research by Han et al., indicating that some HER2 polymorphisms can be associated with better outcomes. These mixed results underscore the need for further research into the molecular mechanisms behind trastuzumab resistance, providing insights that can lead to more targeted and effective treatment strategies. The hydrophobicity and conformational stability of the hydrophobic domains, such as transmembrane, may be altered due to the isoleucine to valine change [25]. HER2-positive breast cancer cells carrying the Val allele might be more prone to developing trastuzumab resistance in the presence of alternative signaling pathways [16].
This research and other studies can improve the diagnosis, prognosis, and treatment of this type of cancer and develop more accurate treatment strategies. Additionally, our study has several limitations. Some subgroup comparisons, such as Fars versus Arab + Lor or G2 versus G1 + G3, were not performed, as the study design focused on predefined comparisons based on clinical relevance and hypotheses determined before data analysis. The relatively small sample size may have reduced the statistical power and contributed to the absence of individuals with the GG genotype, possibly affecting the observed association with patient survival in the multivariate model. The short follow-up period was another constraint. Moreover, we assessed the association of this polymorphism with only one drug (trastuzumab) and, due to high laboratory costs, could not examine additional polymorphisms. The lack of gene sequencing for BRCA1, BRCA2, and PALB2 mutations, which may influence treatment response, was also a limitation. Finally, our research did not evaluate cardiotoxicity, a relevant aspect highlighted in previous studies on the HER2 Ile655Val polymorphism and trastuzumab, and should be acknowledged as a further limitation.
In conclusion, our data suggest that HER2 rs1136201 polymorphism significantly predicts the response to trastuzumab in HPBC patients. Thus, patients homozygous for the minor allele (GG) had significantly worse PFS rates than patients homozygous for the major allele (AA) or heterozygous form (AG). Our results demonstrate that genotyping of the rs1136201 polymorphism before the start of trastuzumab therapy may help to stratify HPBC patients and identify those who respond better to this treatment. Further studies are needed to confirm the data regarding the role of rs1136201 polymorphism and other variants in responding HPBC patients to trastuzumab. However, when well confirmed, these studies may allow genetic screening before the start of anti-HER2. They could potentially be used for personalized treatment of HPBC and help to improve the outcome of this group of patients.



Comments (0)