
Remember me


Here we have reviewed systematically the relevant scientific literature starting from the twenty-first century regarding the clinical utility of 3D MRI in the assessment of stenoses of the spine. In general, a lot of heterogeneity exists among the studies conducted on this subject including the study setups, imaging techniques, reference standards, assessment of diagnostic performance and reliability analyses.
Lumbar and cervical MRI examinations are the most common MRI scans in everyday clinical workflow to evaluate radiculating extremity pain, suspected central stenosis or prolonged back pain. Historically, the lumbar MRI usually consists of several routine 2D sequences (T2 & T1 weighted sagittal, T2 weighted axial and STIR coronal planes), and the cervical MRI includes 2D T1 & T2 weighted sequences in sagittal plane and T2 weighted FSE or GRE sequences in axial plane. However, to date, no specific guidelines for the exact composition of lumbar or cervical MRI protocol exists. Although the use of 3D lumbar and cervical spine MRI sequences has transpired since the 2010s, the current literature offers no answer, which 3D sequence is the best or most optimal to image spine and associated pathologies. Based on this current literature review, it seems that 3D sequences offer superior overall evaluation of recess stenoses [3, 8] and increased sensitivity to detect foraminal (both intra- and extra-) stenoses at least in lumbar level [2, 6,7,8]. These observations have also been confirmed at our institution intuitively (Figs. 1, 2, 3 and 4). Although the evaluation of central canal stenosis seems to be equivalent in both 2D and 3D MRI techniques, it could be argued that 3D sequences provide some aid in the respect of accurate slice orientation; this phenomenon was already confirmed in the year 2012 by Henderson and colleagues, who showed that 3D MRI approach was superior in the measuring and grading of the lumbar central canal stenosis [28].
Fig. 1
Comparison of 2D and 3D MRI sequences with corresponding axial images at the lumbar level of L3/4. In the conventional 2D T2 TSE axial image the degree of foraminal stenosis remains unclear (black arrow) due to scarring from previous surgery and partial volume effect (A). In the 3D T2 TSE (SPACE) image, no stenosis is detected (white arrow) (B)
Fig. 2
Evaluation of lumbar recess stenosis on 2D and 3D MRI sequences. A typical L4/5 disc herniation is seen on conventional 2D T2-weighted sagittal MR image (A). In the routine 2D T2 TSE axial image no recess stenosis is visible (white arrowhead) (B), whereas in the 3D T2 TSE (SPACE) image a definite stenosis is seen in the left lateral recess (white arrow) (C)
Fig. 3
Comparison of 2D and 3D MRI sequences with corresponding axial images at the cervical level of C6/7. In the conventional gradient echo axial image, there seems to be only mild stenosis on the left side (white arrowhead) (A). In the 3D T2 TSE (SPACE) image, severe stenosis is detected (white arrow) (B)
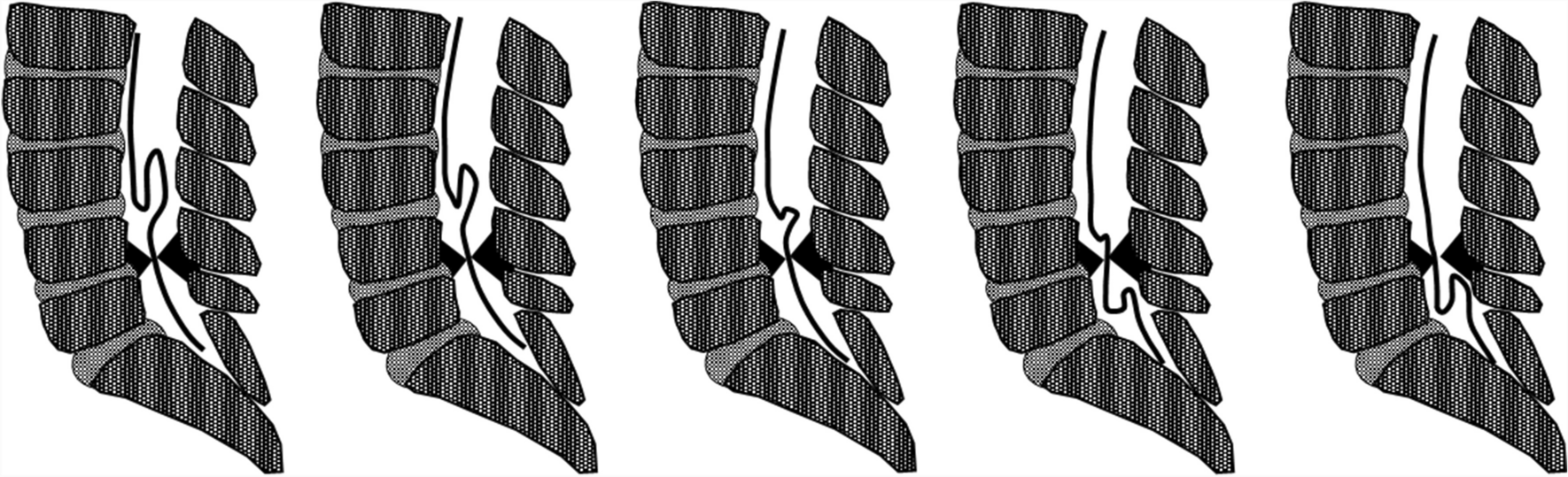
Fig. 4
Assessment of cervical foraminal stenosis on 2D and 3D MRI sequences. Conventional 2D T2-weighted GRE sequence (MEDIC) shows moderate stenosis of the left C8 foramen (black arrow) probably due to partial volume effect (A), since in 3D T2 weighted TSE (SPACE), the C8 foramina are wide and symmetrical (white arrows) (B). Another advantage of 3D sequence is the ability to visualize nerve canals in sagittal oblique reformats (C) (as shown by the perpendicular white lines in B)
The main focus of cervical MRI is usually in diagnosing stenosis. However, demonstration of abnormal signal in the cord (i.e. spondylotic myelopathy) is also important, especially since it may serve as a prognostic tool in aiding surgeons with clinical decision making [29]. Traditionally, it has been thought that gradient based T2 sequences are superior or even mandatory in diagnostic work-up of cord pathology. Indeed, delineation of spinal cord structures and CNR were better in gradient based 3D FFE sequence than in 2D TSE sequence in a study with healthy volunteers [30]. However, also 3D T2 FSE sequences have been shown feasible in spondylotic myelopathy, even though poorer CNR compared to conventional 2D FSE sequence was evident [18, 26]. Postoperative recovery varies greatly even with similar cord pathology on imaging. Urakawa et al. (2011) speculated that this may partly be due to inability of conventional images to distinguish individual tracts and presented 3D anisotropy contrast single-shot echo planar imaging as a solution [31]. Thus, it may well be that adequate imaging of cord pathology requires completely different methods beyond the scope of this review article.
Based on the literature it is difficult to conclude the best 3D sequence to use for imaging spinal stenosis. More specifically, quantitative comparison between 3D and 2D based sequences can be cumbersome due to the fact that the contrast, resolution and scan time all are affected by the choice of the sequence parameters (mostly, the choice of repetition time (TR), echo time (TE), number of slices etc.)), type of sequence (e.g. Spin-echo and Gradient echo based sequences; T1, T2 –weighted and inversion recovery –based sequences etc.) and the used field strength (1.5 T vs. 3 T). For example, traditional 3D spin echo (SE) sequences (e.g. SPACE, CUBE etc.), require longer acquisition time and different contrast properties than 3D gradient echo techniques (e.g. MPRAGE, MERGE etc.). The long acquisition times can be overcome by using techniques that accelerate the imaging process, for example parallel imaging or CS [13, 23]. Most of these acceleration methods are not lossless and may deteriorate the final image, however, recent studies have demonstrated that developments in deep learning reconstruction methods may help to overcome this [21, 27].
The literature also showed nonuniform voxel sizes, interpolation and varied use of reformatted image planes from the 3D images. Particularly, the use of isotropic voxel sizes is advised in 3D imaging to get uniform reformats in all three planes. Notably, most 3D sequences gathered here were imaged in either sagittal or coronal planes which require generally larger FOVs, but less slices to cover the regions of interest, while in the authors' institution, the imaging in done in axial plane. The choice of primary phase-encoding direction (i.e. the imaging plane) can affect imaging time and manifestation of imaging artefacts (wrapping, flow and motion artefacts and geometric distortion).
All in all, many challenges exist in comparing 3D and 2D sequences. Particularly, when it comes to the choice of compared imaging techniques and sequences, there seems to be notable discrepancy (e.g. comparisons between T2-weighted and T1-weighted images, between sequences imaged with scanners from different vendors, different types of sequences (SE, GRE, STIR etc.)) (Tables 1 and 2). Nevertheless, well optimized 3D sequences allow the use of higher spatial resolution, similar scan time and increased SNR and CNR when compared to 2D sequences [11, 13]. However, the largest benefit of 3D sequences is in the clinical value of the additional information provided by them and in the possibility to replace a number of 2D sequences to save time. Especially, the ability to review images in any orientation allows better visualization of stenosis and is extremely beneficial in anatomical deformities such as scoliosis [8].
Comments (0)