Melorheostosis is a rare mesenchymal bone dysplasia that presents as excessive sclerotic bone that grows on pre-existing host bone surfaces. It was first described in 1922 by Léri and Joanny [7]. Its name derives from the Greek “melos” for limb, “rhein” for flowing, and “ostosis” for bone formation [1]. Classically, the presentation of melorheostosis as described in literature is that of osteosis with the appearance of flowing wax. The disease usually begins sporadically in adolescence and has no sex predilection [8, 9]. Diagnosis of the disease usually occurs at ages 20 or younger [8,9,10].
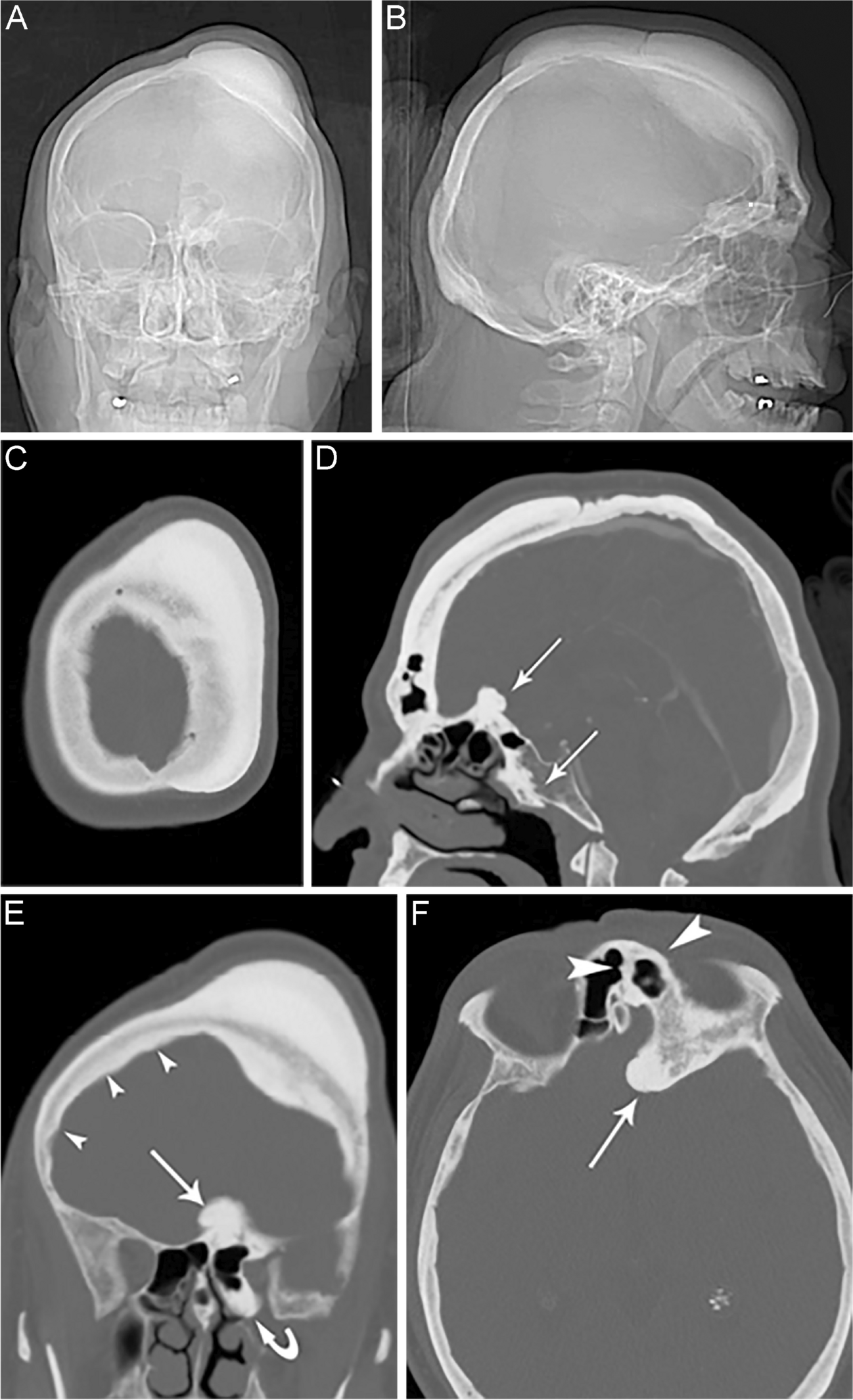
As is evident from the name of the disorder, melorheostosis typically appears in the appendicular skeleton. Involvement of the axial skeleton is rare [11], and craniofacial involvement is even more so [12]. A case of craniofacial melorheostosis involving the facial bones and a portion of the calvarium was reported previously [6], but to our knowledge, no clear cases centered in the calvarium have been reported.
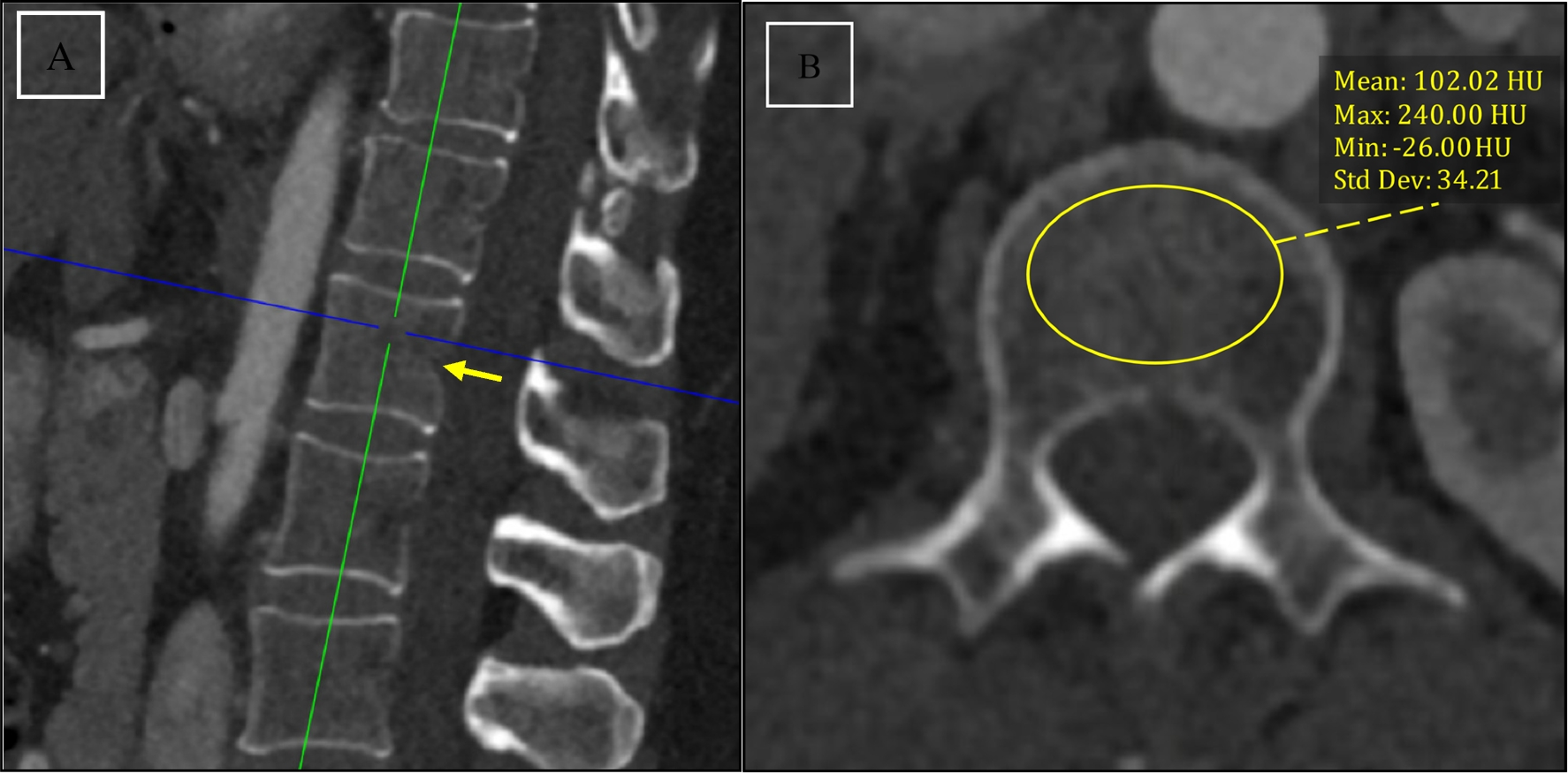
This case of melorheostosis did not have the flowing candle wax appearance first described by Léri and Joanny [7], presumably due to the vastly different configuration of the bone involved. Initial impressions of the radiographs and computed tomography studies led to a differential diagnosis including osteoma/Gardner syndrome and genetic or metabolic bone syndromes such as Van Buchem syndrome or hypercalcemia. The initial radiologic impression of an osteoma is reminiscent of some studies that show some cases of melorheostosis with an osteoma-like appearance [3, 13]. According to one series, the osteoma-like appearance is more common than the candle wax appearance; out of 23 cases, 7 (30%) had an osteoma-like appearance and 5 (22%) had the candle wax appearance [3]. In the present case, there were some areas of focal sclerosis radiographically within the diploic space, indicating that the process was not confined only to the outer and inner tables, further distinguishing this entity from osteoma. Diploic involvement is analogous to marrow involvement seen in melorheostosis in long bones, where bone marrow edema may also be seen [14]. In addition, osteomas are usually much smaller than the case presented and often are isolated lesions. Our patient also had no other signs or symptoms of Gardner syndrome, making this diagnosis less likely. Van Buchem syndrome is a heritable sclerosing bone dysplasia that results in extensive osteosis, and when present in the skull involves thickening of the maxilla and mandible [15]. However, it has almost entirely been recorded in people of Dutch descent, or from other nearby regions, making it less likely in this case.
The exact etiology of melorheostosis is unknown. Much of the research in melorheostosis has been in the context of coexistence with osteopoikilosis, Buschke-Ollendorff syndrome, and mixed sclerosing bone dysplasia [16]. While the cases that coexist with other diseases are much rarer than sporadic cases, it is of interest that overlap exists among these diseases. A loss-of-function mutation in the LEMD3 gene has been described in osteopoikilosis and Buschke-Ollendorff syndrome. The MAN1 inner nuclear membrane protein encoded by LEMD3 is responsible for the modulation of TGFβ and bone morphogenetic protein signaling, which activate genes involved in bone formation. Melorheostosis concurrent with osteopoikilosis has been shown to be associated with the LEMD3 mutation [17]. Sporadic cases of melorheostosis are not associated with the loss-of-function mutation of LEMD3. Instead, it has been shown that the bone associated with melorheostosis has a mutation in the MAP2K1 gene, which encodes the protein kinase MEK1 [16, 17]. The mutation results in a loss of function for MEK1, which in turn increases osteoblast proliferation and reduces their differentiation. The result of this mutation may explain the histologic features described in melorheostosis, an increase in osteoblast/osteoclast number as well as an increase in osteoid and bone remodeling. Interestingly, cases of melorheostosis in which the MAP2K1 mutation is present are the cases in which the flowing candle wax appearance is noted [18] as well as the previously mentioned histologic findings. Cases of melorheostosis without the MAP2K1 mutation lack the candle wax sign and do not have increased osteoblast/osteoclast counts when examined histologically. In our case, DNA sequencing was attempted; however, insufficient genomic material was available for genomic testing due to the nature of the tissue submitted.
While there is a reported quantitative difference in the counts of osteoblasts/osteoclasts between MAP2K1 mutation positive and negative cases of melorheostosis, there are other features that may be useful in aiding the diagnosis of melorheostosis histologically. While these vary from case to case, these findings include an increase in cortical density, presence of woven bone, increased porosity, disorganized osteoid formation, and angiogenesis [4]. However, the presence of these features can be variable and in some cases present only with an increase in cortical density as in our case [4]. Histologic analysis of melorheostosis is not necessarily required for the diagnosis if the classic radiologic findings are present; however, in some cases, it is needed to rule out potential malignancy as some bone-forming tumors, such as parosteal osteosarcoma, may have similar radiologic characteristics [19]. By histology, these two entities can usually be separated by identifying the classic features of a parosteal osteosarcoma including long parallel arrays of bone with an infiltrating, bland, but atypical, spindle cell proliferation. Fluorescence in situ hybridization may also be of benefit as parosteal osteosarcoma is known to harbor amplification of the MDM2 gene [20].
The diagnosis of melorheostosis is often suggested due to the radiologic recognition of the flowing candle wax appearance as described in the literature. However, there exist cases of melorheostosis that do not fit this profile, and careful radiologic and pathologic analysis can be essential in making this diagnosis.



Comments (0)