In the current study, the commonly used AA-TP technique was found to overestimate LLD by 3.70 mm compared to the IT-TP technique. Additionally, there was an absolute increase of 14% in the risk of reporting a clinically significant LLD when the AA-TP technique was used instead of the IT-TP technique. The odds of a result exceeding this clinically significant LLD threshold of 10 mm when using the AA-TP technique were 3.8 times higher than when using the IT-TP technique.
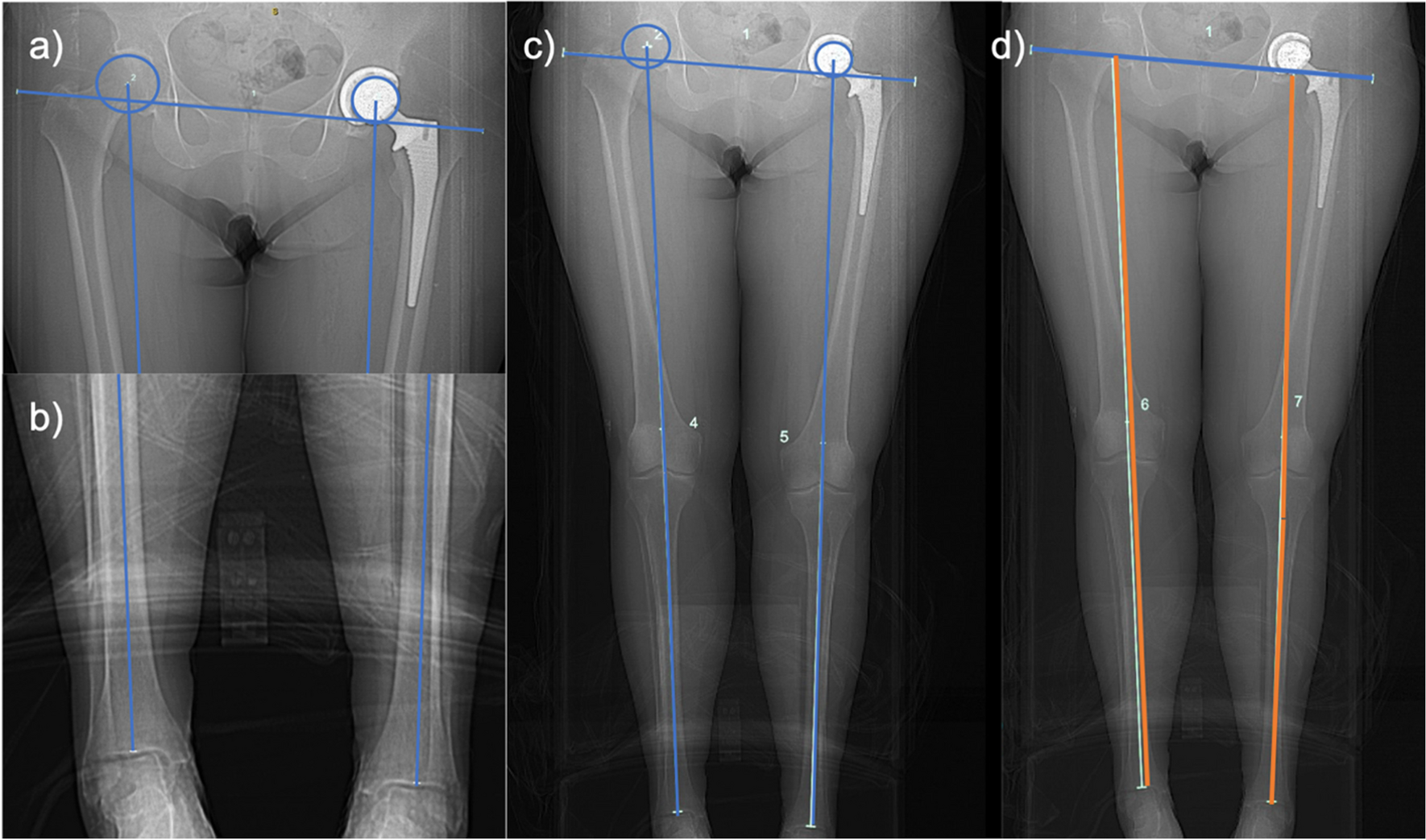
When establishing reference landmarks for leg length, it is essential that they are readily identifiable and exist in the same axial plane to ensure measurement accuracy. This can become challenging in prosthetic joint replacement, where certain anatomical structures may no longer be present bilaterally. For example, using the apex of the acetabular component as the superior landmark on the operative side and either the sourcil or apex of the native femoral head on the contralateral side highlights these issues. Not only do these landmarks exist in different axial planes, but the average distance between them is inconsistent and unpredictable due to factors such as proximalization of the hip joint from acetabular reaming, often resulting in an overestimation of operative limb length.
Routinely assessing LLD after total hip arthroplasty is essential, particularly for patients with dissatisfaction or suboptimal post-operative outcomes [1,2,3]. Notably, an LLD of 10 mm or more is often associated with clinical issues, including gait asymmetry, back pain and symptomatic or progressive hip and knee osteoarthritis [28,29,30]. However, overdiagnosis of LLD can also be problematic. The significant increase in reported LLD in this study could theoretically heighten patient anxiety and complicate evaluation in cases of post-operative dissatisfaction. This is especially relevant given the clinical and medicolegal implications of a radiologically measured LLD exceeding published thresholds [5, 6].
The reported rate of clinically significant post-arthroplasty LLD (≥ 10 mm) varies considerably in the literature, with rates between 3 and 23.5% [13, 22]. Other studies have noted mean LLD values of 9–10 mm [1, 9]. Most of these assessments used Woolson’s method exclusively, without a full-limb comparator. There is limited recent data comparing post-operative LLD measured on traditional AP pelvic radiographs to modern full-limb imaging methods. In a study by Hardwick-Morris et al., LLD measurements were conducted using AP pelvic radiographs and EOS scans for 93 patients, revealing a mean LLD of 1.7 mm on AP radiographs (4.2% of the cohort ≥ 10 mm) using Woolson’s method on weight-bearing x-rays, 0.6 mm when measured from the femoral head centre to the ankle centre (17.9% were ≥ 10 mm) and 3.1 mm when measured from the ASIS to the ankle centre (32.6% were ≥ 10 mm) [23]. Although these measurements were pre-operative and cannot be directly compared, the findings, similar to those in this study, underscore the meaningful impact of imaging modality and landmark selection on LLD measurement. To our knowledge, this study is the first to assess the magnitude of LLD differences using various full-limb imaging techniques in the post-operative setting.
Surprisingly, despite the recognized importance of leg length discrepancy after total hip arthroplasty, no widely accepted reference standard exists [31, 32], underscoring the need for studies like this to compare techniques and establish a standard. CT scans are readily accessible in most healthcare settings, and CT scanograms have a high level of accuracy, inter-observer reliability and intra-observer reproducibility when measuring leg length discrepancy [17, 33]. However, other imaging modalities may be preferred in the post-operative follow-up of arthroplasty patients by some practitioners for various reasons, including accessibility, radiation minimization or costs. The authors believe that the findings on measurement techniques from the current study may be applicable to other imaging modalities, particularly other orthogonal modalities like EOS 3D biplanar radiographs (EOS Imaging, Paris, France), which also minimize distortions caused by the parallax effect.
Since many orthopaedic surgeons still use post-operative anteroposterior pelvic radiographs to assess leg length after surgery, the authors wished to compare a commonly utilized technique, Woolson’s technique (distance between inter-teardrop line and lesser trochanter [17, 18, 21, 22]), with both full-limb techniques previously discussed, IT-TP and AA-TP. The degree of correlation between measurements obtained using the IT-TP and Woolson methods, both of which use the inter-teardrop line as their proximal reference line, was only determined to be fair [26]. Woolson’s technique is unable to take into account any factor affecting limb length distal to the lesser trochanter as it is measured on an anteroposterior x-ray of the pelvis only. Additionally, the inter-observer and intra-observer reliability of each technique measured in the current study was categorized as excellent, although Woolson’s method demonstrated the lowest inter-observer agreement of the methods studied. These shortcomings may be also explained by increased variability in lesser trochanter morphology and limb rotation, which can obscure the trochanter behind the femoral shaft, leading to slightly differing interpretations of the lesser trochanter apex location amongst observers. Therefore, in clinical situations where a CT scanogram image is not available, this technique may provide an adequate indication of leg length discrepancy; however, in situations where accuracy is critical, measuring on full-limb imaging, especially using the IT-TP technique, may be preferable.
A strength of the current study is the inclusion of a less experienced interpreter who was a medical student at the time of measurement. The excellent intra-rater and inter-rater reliability results obtained between observers of differing levels of clinical experience enhance the external validity and applicability of our findings.
The current study has some limitations. First, the current project evaluates only the radiological measurements of tLLD, without assessing clinical outcomes or perceived LLD. Therefore, the clinical significance of these findings remains uncertain and requires cautious interpretation. Then, rotation of the lesser trochanter and lower limb was not perfectly controlled for, and seven patients were excluded on the basis of a poor-quality CT scanogram. Whilst this may account for some differences found between measurements taken using the scanogram images and those on AP pelvis x-rays (Woolson’s technique), the IT-TP and AA-TP measurements were made on the same scanogram images.
Current CT scanogram measurements from the acetabular apex to the tibial plafond often overestimate operative limb length due to reference landmarks in different axial planes. Measurements from the inter-teardrop line to the tibial plafond yield significantly lower LLD values, possibly reflecting actual limb length better. The authors recommend using the inter-teardrop line and tibial plafond as reference landmarks to improve LLD assessment accuracy post-arthroplasty.



Comments (0)