
Remember me



The clinical features of the five patients are summarized in Table 1. The patients included five females ranging in age from 43 to 77 years. Lymphedema was caused by surgical intervention for uterine cervical cancer or ovarian cancer in three patients, idiopathic in one, and disuse edema following an ischemic stroke in one. The duration of lymphedema ranged from 8 to 18 years. The presenting symptoms included a palpable mass in three patients, painful skin exanthesis in two, and bleeding in one. Tumors were located in the lower leg in three patients and in the lower abdominal wall in two. Histologic diagnosis was made by biopsy in two patients and by surgical resection in three patients. Of the former two patients, one received palliative therapy and the other received chemoradiotherapy. Of the latter three patients, two had positive pathologic margins and were subsequently treated with adjuvant chemotherapy. Of the four patients treated curatively, three relapsed; two patients developed local recurrence, one developed systemic lymph node metastases and one developed lung metastases. In the final outcome, three patients died of the disease between 6 and 23 months, one is alive with disease after 60 months of follow-up, and one was alive without disease after 481 months of follow-up.
Table 1 Clinical features of the institutional five patientsThe MRI and pathologic features are summarized in Table 2, and representative cases are presented in Figs. 3, 4, and 5. The tumor depth was the subcutis in three cases and the cutis and subcutis in two. Outer protrusion from the skin surface was observed in three cases. Four cases had multiple masses and one single mass. The mean maximal diameter of the largest lesion in each case was 6.0 cm, ranging from 4.3 to 10.4 cm. The tumor shape was confluent multinodular in three cases and amorphous or diffuse in two. The tumor margins were ill-defined in all cases. On T1-weighted images, two tumors showed a mixture of high and intermediate signal intensities with a predominance of intermediate signal intensity, and the remaining two showed intermediate signal intensity. On T2-weighted images, four tumors showed a mixture of high and intermediate signal intensities and one showed a mixture of intermediate and low signal intensities. Among these mixed signal intensities, the intermediate signal intensity was predominant in four cases. Our first presentation of ADC mapping was obtained in four cases. The mean ADCmean value were 0.88 × 10−3 mm2/s, ranging from 0.77 × 10−3 to 0.96 × 10−3 mm2/s.
Table 2 MRI and pathologic features of the institutional five patientsFig. 3
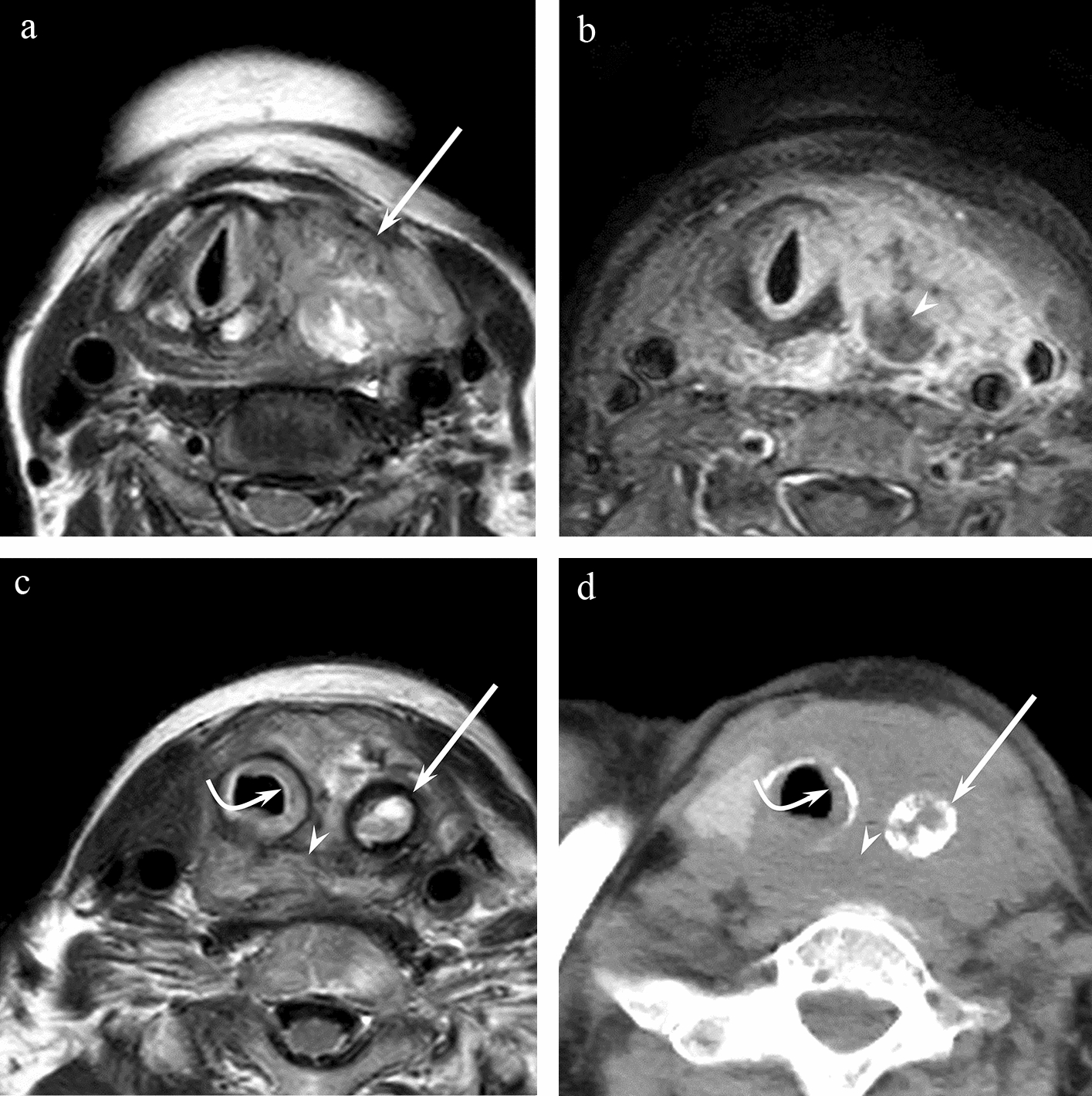
A 75-year-old female, with a 10-year history of lower extremity lymphedema following hysterophenectomy for ovarian cancer presented with painful dark red exanthesis of the left lower leg (case 1). a Axial T1-weighted image shows multiple ill-defined masses with intermediate signal intensities. b On axial T2-weighted image, the signal intensities of the masses are mainly intermediate and partly high. c Coronal contrast-enhanced fat-suppressed T1-weighted image shows the confluent multinodular shapes of the masses. d and e DW image and ADC map show hyperintense masses with low ADC values (ADCmean = 0.96 × 10−3 mm2 /s) on the ADC map. f Microscopy of a lower-power field shows a predominant distribution of a solid sheet of tumor cells and a convoluted border between the tumor and subcutaneous connective tissue without capsular formation (double-lined arrows). The former appears to contribute to the low ADC values and the latter to the ill-defined margin on MR images. g Microscopy of a high-power field in a central area of the tumor shows a proliferation of tumor cells with atypical nuclei of various sizes. h In a peripheral area of the tumor, microscopy of a high-power field shows an infiltration of numerous inflammatory cells (arrows) in addition to the infiltrative growth of tumor cells
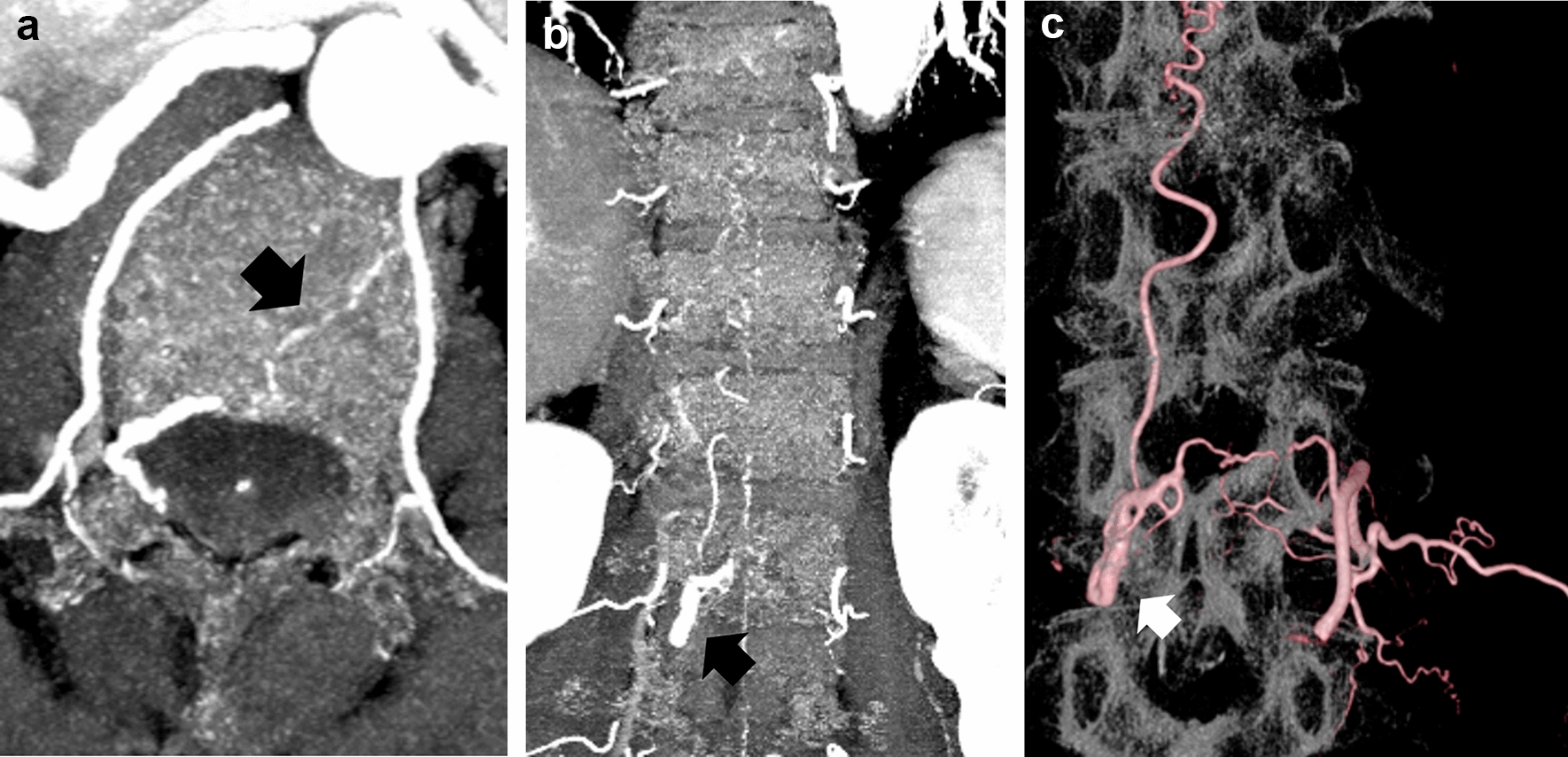
Fig. 4
A 64-year-old female with an 8-year history of lower extremity disuse edema caused by cerebral infarction, presented with hemorrhagic masses of the left lower leg (case 2). a and b Axial T2-weighted and fat-suppressed T2-weighted images show an ill-defined mass with a confluent multinodular shape. c On sagittal fat-suppressed T2-weighted image, multiple masses in close proximity are identified (arrows). d and e DW image and ADC map show a hyperintense mass with low ADC values (ADCmean = 0.83 × 10−3 mm2/s).
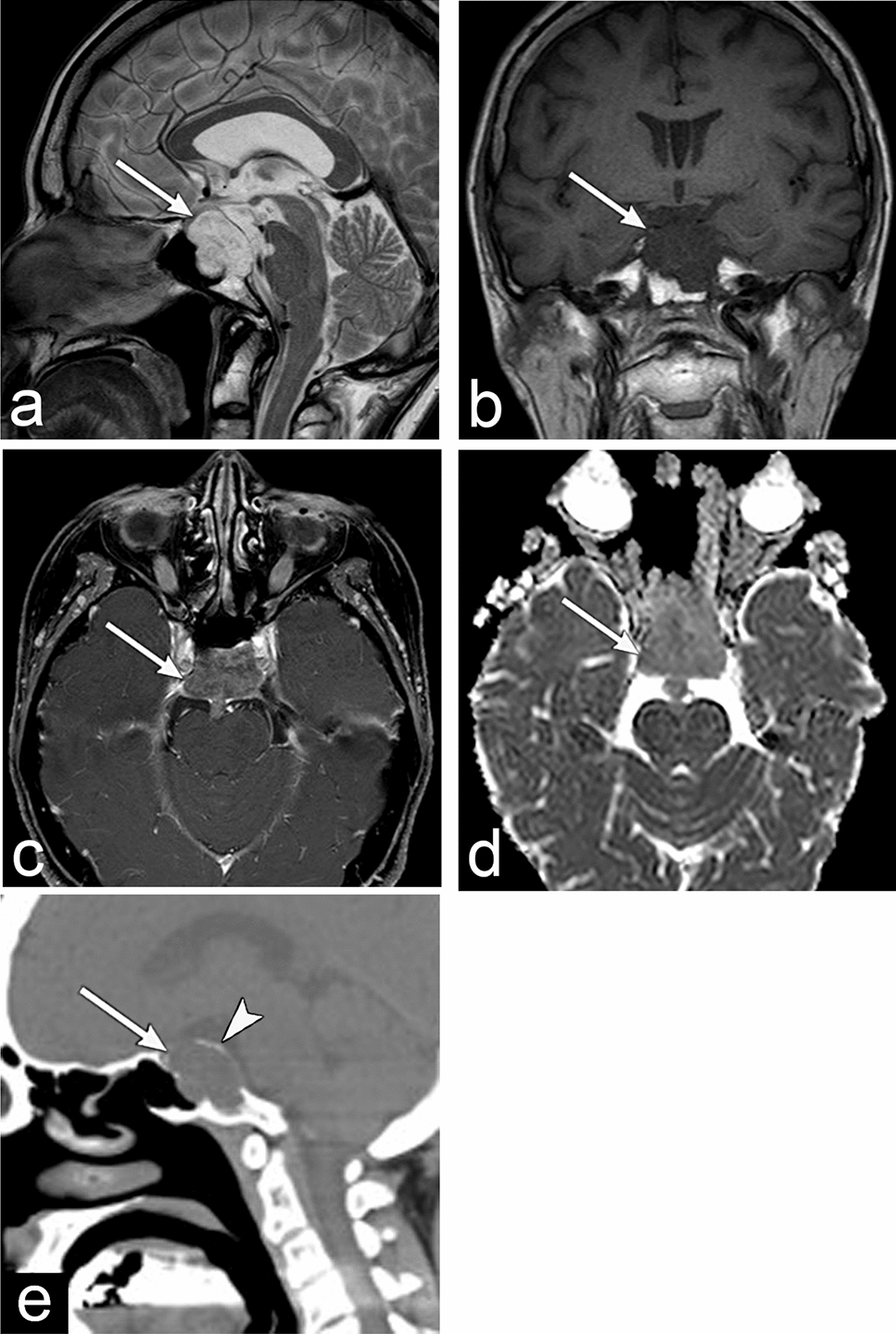
Fig. 5
A 77-year-old female with a 10-year history of lymphedema following radical hysterectomy with pelvic lymphadenectomy for cervical cancer, presented with a palpable mass of the left lower abdominal wall (case 5). a and b Axial T1 and T2-weighted images show an ill-defined subcutaneous mass in the lower abdominal wall. c and d Sagittal T2- and fat-suppressed T1-weighted images show a confluent multinodular shaped mass with a mixture of intermediate and high signal intensities
In the histopathologic correlations available for four cases, infiltrative growth of tumor cells with inflammatory cells was observed in all cases. In the central part of the tumor, a solid architectural pattern consisting of dense cell proliferation with relatively little stroma was observed in three cases. Intratumoral hemorrhage was identified in three cases.
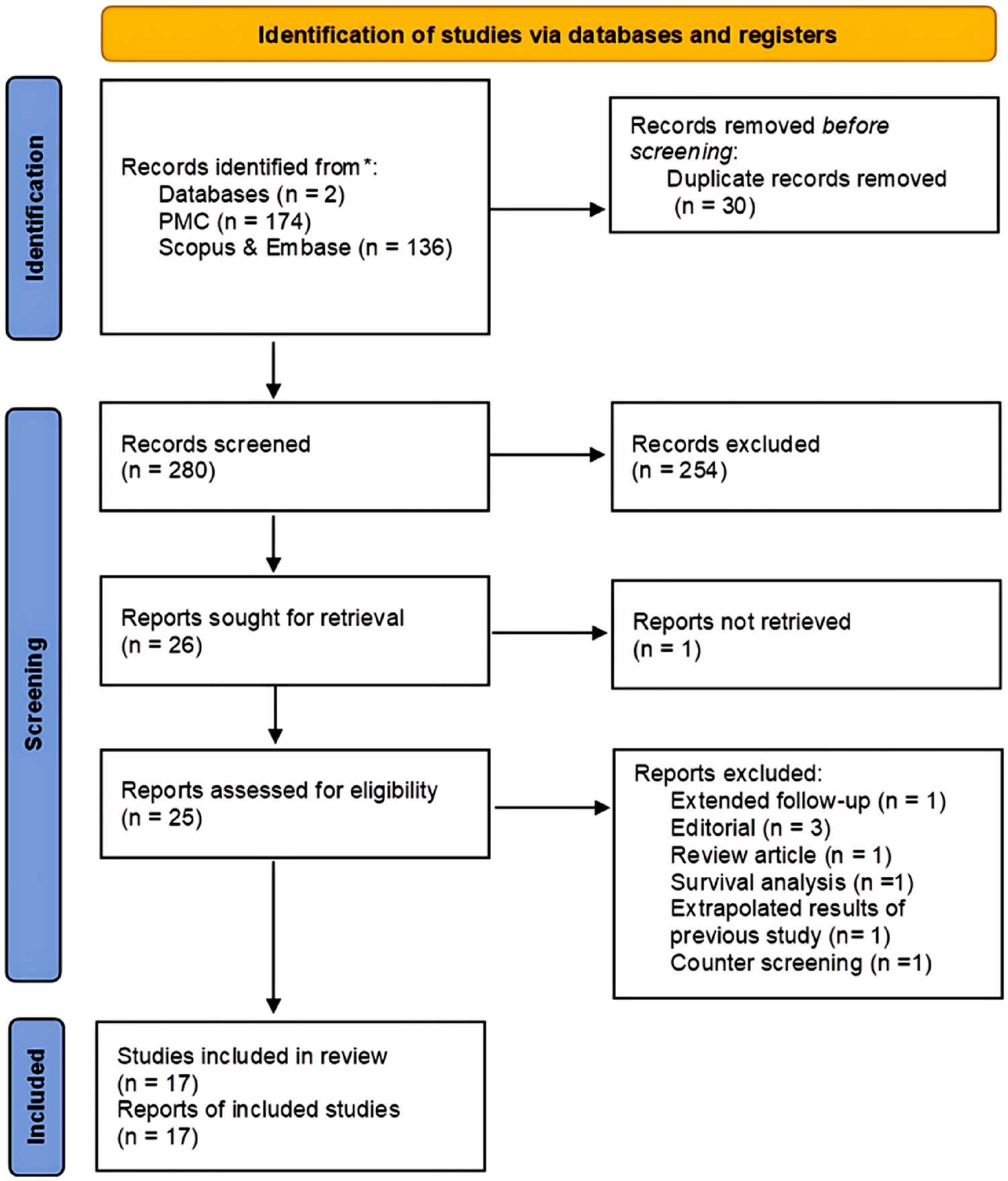
Article selectionThe initial literature search yielded 123 articles, and after the removal of duplicated articles and screening of abstracts, 53 potentially eligible articles were assessed for further full-text review. After excluding 39 articles, 24 cases from 14 articles met the selection criteria for the systematic review [2, 7, 11,12,13,14,15,16,17,18,19,20,21,22]. A citation review identified an additional case from an article that met the selection criteria [23]. Finally, 25 cases from 15 articles were included in the systematic review (Fig. 1). Combined with five cases from our institutions, the final study cohort included 30 STS cases.
Clinical features of the combined dataTable 3 summarizes the clinical features of the combined 30 patients. The patients included 25 females and 5 males, with a mean age of 60 years, respectively, ranging from 15 to 90 years. The most common cause of lymphedema was surgical intervention for breast cancer in 13 patients (13/23, 56.5%), followed by surgical intervention for uterine cervical cancer in four patients (4/23, 17.4%). The mean duration of lymphedema was 12 years, ranging from 8 to 20 years. The most common presenting symptom was a palpable mass (11/13, 84.6%), followed by skin discoloration or exanthesis (8/13, 61.5%). Except for two cases of lower abdominal origin (2/30, 6.7%), all tumors were located in the extremities; the most common sites were the lower leg (8/30, 26.7%) and forearm (8/30, 26.7%), followed by the upper arm (4/30, 13.3%), foot (4/30, 13.3%), thigh (3/30, 10.0%), and hand (1/30, 3.3%).
Table 3 Clinical features of the combined 30 patientsMRI features of the combined dataTable 4 summarizes the MRI features of the combined 30 patients. Tumor depth was at the cutis in two cases (2/25, 8.0%), cutis and subcutis in 17 (17/25, 68.0%), and subcutis in six (6/25, 24.0%). Ten of the 23 tumors involving the subcutis were in contact with the deep peripheral fascia; however, none extended beyond the fascia. Outer protrusions from the skin were observed in 10 tumors (10/22, 45.5%). Multiple tumors were observed in 16 cases (16/27, 59.3%). The tumor shape was round or oval in four cases (4/21, 19.0%), confluent multinodular in eight (8/21, 38.1%), and amorphous or diffuse in nine (9/21, 42.9%). The tumor margin was ill-defined in 26 cases (26/28, 92.9%). On T1-weighted images, the common signal intensity of the tumors was intermediate (16/19, 84.2%). In the remaining cases (3/19, 15.8%), the signal intensity was a mixture of intermediate and high, with an intermediate predominance. The signal intensities on T2-weighted images were intermediate in seven cases (7/13, 53.8%), a mixture of intermediate and high in five (5/13, 38.5%), and a mixture of intermediate and low in one (1/13, 7.7%). In all tumors with mixed signal intensities, the intermediate signal intensity was predominant. On fat-suppressed T2-weighted images, the common signal intensity was a mixture of intermediate (7/11, 63.6%). Contrast-enhanced images showed homogeneous enhancement in nine cases (9/12, 75.0%) and heterogeneous enhancement in three (3/12, 25.0%). In conclusion, angiosarcomas presenting as Stewart-Treves syndrome usually involved the subcutis and more than half were multiple. In more than 90% of cases, the tumor has an ill-defined margin and predominantly intermediate signal intensities on both T1- and T2-weighted images.
Table 4 MRI features of the combined 30 patients
Comments (0)