Design and data sources
Using detailed individual-level data from national registries and databases, we performed a nation-wide cohort study in Denmark, Finland, Norway, and Sweden. In these countries, girls are offered free-of-charge HPV vaccination through the national childhood immunization programs (NCIPs). The vaccine is offered at age 12 years in Denmark, Finland, and Norway, and at age 11 or 12 years in Sweden. Throughout the study period (defined below), Finnish girls were offered the bivalent vaccine Cervarix®, targeting HPV16 and HPV 18, while Swedish girls were offered the quadrivalent vaccine Gardasil®, targeting HPV6, HPV11, HPV16, and HPV 18. In Denmark and Norway, girls were initially offered Gardasil®, but towards the end of the study period, the vaccine used in the programs changed to Cervarix®. Further details of the HPV vaccination programs are presented in Table 1. Furthermore, vaccines offered through the NCIPs between ages 4 and 15 years to girls in the birth cohorts eligible for HPV vaccination are presented in Supplementary Tables 1–4. Information on vaccinations was obtained from The Danish Vaccination Register, the Finnish vaccination register, the Norwegian Immunization Registry, and the National Vaccination Register in Sweden [21,22,23,24]. The registries contain information on vaccines in the NCIP since 1996 in Denmark, 2009 in Finland, 1995 in Norway, and 2013 in Sweden.
Table 1 HPV vaccine in the national childhood immunization programs in the Nordic countries during the study periodInformation on hospital contacts was obtained from patient registries with national coverage and individual-level data since 1978 in Denmark, 1994 in Finland, 2008 in Norway, and 1987 in Sweden [25]. Information on redeemed prescriptions, demographics, socioeconomic factors, and residency was also obtained. Data from the different registers was linked using the unique personal identifier assigned to all residents in the Nordic countries.
A description of the common data model used to generate homogenous country-specific data sets has been published previously [26]. Due to data protection legislation, the data was stored and analyzed separately in each country.
Study period
In Denmark and Finland, the study period started when HPV vaccine was introduced into the NCIP; January 1, 2009, and November 1, 2013, respectively. In Norway, the study period started January 1, 2010, the first date with complete information on all covariates (described below). In Sweden, it started January 1, 2013, when the National Vaccination Register was launched. The end of the study period was defined as the last date with available information from all the registries: December 31, 2017, in Denmark, Finland, and Sweden; and December 31, 2018, in Norway.
Study population and follow-up
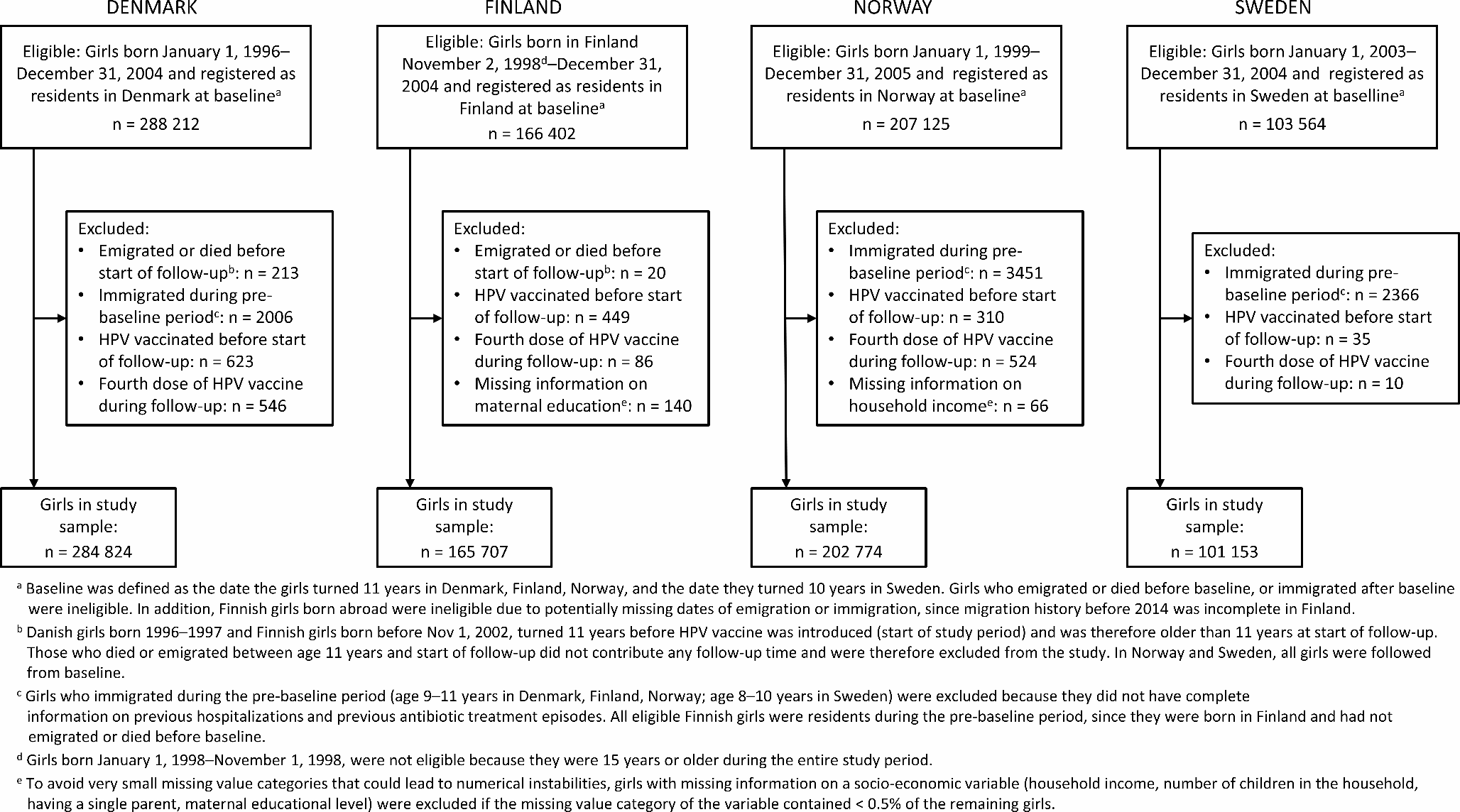
We included girls from the birth cohorts offered HPV vaccine through the NCIPS during the study period: 1996–2004 in Denmark; 1998–2004 in Finland; 1999–2005 in Norway; 2003–2004 in Sweden. The study was limited to Danish, Finnish, and Norwegian girls aged 11–14 years and Swedish girls aged 10–14 years. Baseline was defined as the date the girls turned 11 years in Denmark, Finland, Norway, and the date they turned 10 years in Sweden, i.e., approximately 1 year prior to when HPV vaccine was usually offered. To be eligible for inclusion, we required that girls were registered as residents at baseline, to ensure that potential HPV vaccination could be captured. Moreover, Finnish girls born abroad were not eligible, since migration history before 2014 was incomplete and residency at baseline could therefore not be verified [26].
Follow-up started at baseline or at start of the study period, whichever occurred last. Girls who died or emigrated between baseline and start of the study period were excluded from the study. Follow-up ended at emigration, death, age 15 years, or end of the study period, whichever occurred first.
Outcome
The main outcome was infectious disease hospitalization, defined as an inpatient hospital contact with at least one overnight stay and a primary or secondary diagnosis classified as an infection (Supplementary Table 5). Furthermore, we defined a secondary outcome, hospital contacts with at least one overnight stay and a diagnosis classified as a respiratory tract infection (RTI). Infectious disease hospitalization was treated as a recurrent event. Thus, we included all hospitalizations occurring at least 14 days after discharge of a previous infectious disease hospitalization. Time from admission up to the 14th day after discharge was excluded from analyses, since outcomes cannot occur in this time period [27].
HPV vaccination
Girls were considered vaccinated from receipt of the first dose of HPV vaccine until the end of follow-up. Girls who received HPV vaccine before start of follow-up, or received a fourth dose of HPV vaccine during follow-up were excluded from the study.
CovariatesTime-independent covariates
Using information from the year the girls turned 10 years of age, we defined household income level, number of children in the household, having a single parent, and maternal educational level. Because information from the registries was not complete, these variables included an additional missing value category. Due to very small missing value categories (< 0.5%), we excluded Finnish girls with missing information on maternal education and Norwegian girls with missing information on household income. In addition, we defined a variable for immigrant background. Furthermore, we defined variables for previous infectious disease hospitalization and for number of previous antibiotic treatment episodes, using information on hospitalizations and prescriptions from a 2-year period prior to baseline (from age 9 to 11 years in Finland, Denmark, and Norway; from age 8 to 10 years in Sweden). Girls who immigrated during the pre-baseline period were excluded due to incomplete information on these covariates.
Time-dependent covariates
We defined variables for receipt of diphtheria, tetanus, acellular pertussis (DTaP) booster vaccine (Finland, Sweden), diphtheria, tetanus, acellular pertussis, inactivated polio (DTaP-IPV) booster vaccine (Norway), and MMR vaccine (Denmark and Norway), i.e., vaccines in the NCIPs that the girls in the study population could have been offered during the study period. We also defined receipt of influenza vaccine (Finland), and receipt of non-program vaccines (Denmark, Finland, Norway, data not available in Sweden). Finally, we used all hospital contacts from the start of the pre-baseline period until the end of follow-up to define presence of chronic disease, including congenital and acquired conditions such as congenital heart disease, chromosomal abnormalities, cancer, autoimmune disease, and epilepsy. The complete list of diagnoses can be found in the study by Kristensen et al. [28].
Detailed definitions of the covariates are provided in Supplementary Table 6. The variable assessment periods are illustrated in Supplementary Figs. 1 and 2.
Statistical analysis
To evaluate the association between HPV vaccination and risk of infectious disease hospitalization we estimated hazard ratios (HRs) and 95% confidence intervals (CIs) with Cox regression. We used stratified Cox models with calendar year of birth as strata and age in days as the underlying time scale. To account for recurrent events, we used the Andersen-Gill generalization of the Cox model, applying a robust variance estimate [29]. Multivariable models were adjusted for the covariates described above. We also included time-dependent variables for season, defined as spring (March–May), summer (June–August), autumn (September–November), and winter (December–February). We performed a sensitivity analysis limited to girls without immigrant background. Since the vaccine used in the program in Denmark and Norway changed during the study period, we also performed a sensitivity analysis limited to birth cohorts offered Gardasil® (1996–2003 in Denmark, 1999–2004 in Norway). In this analysis, girls were censored at receipt of the first dose of HPV vaccine if this occurred after the change of vaccine was implemented.
Furthermore, we evaluated the effect of number of received doses. In Denmark, Finland, and Norway, this analysis was restricted to girls from birth cohorts eligible for the three-dose schedule (1996–2003 in Denmark, 1998–2003 in Finland, 1999–2004 in Norway). Girls were censored at receipt of the first dose of HPV vaccine if this occurred after the two-dose schedule was implemented. In Sweden, the entire study population was eligible for the two-dose schedule, and girls were therefore censored at receipt of the third dose. The follow-up time for each dose was further categorized according to time since vaccination (1–90 days, 91–180 days, 181–365 days, and > 365 days).
As many Danish girls received HPV and MMR vaccines together, we performed an additional analysis in Denmark to assess whether co-administration was associated with lower risk of infectious disease hospitalization compared to receiving the first dose of HPV vaccine after MMR vaccine. This analysis was limited to girls who had received MMR vaccine at age 11 years or later and the first dose of HPV vaccine, either after or together with MMR vaccine. Start of follow-up was at receipt of first dose of HPV vaccine. We included a time-dependent variable indicating receipt of additional HPV vaccine doses, in addition to the same covariates as in the main analysis.
The analyses were performed using Stata/SE 16.0 and 17.0 (StataCorp, College Station, Texas, USA).


Comments (0)