
Remember me
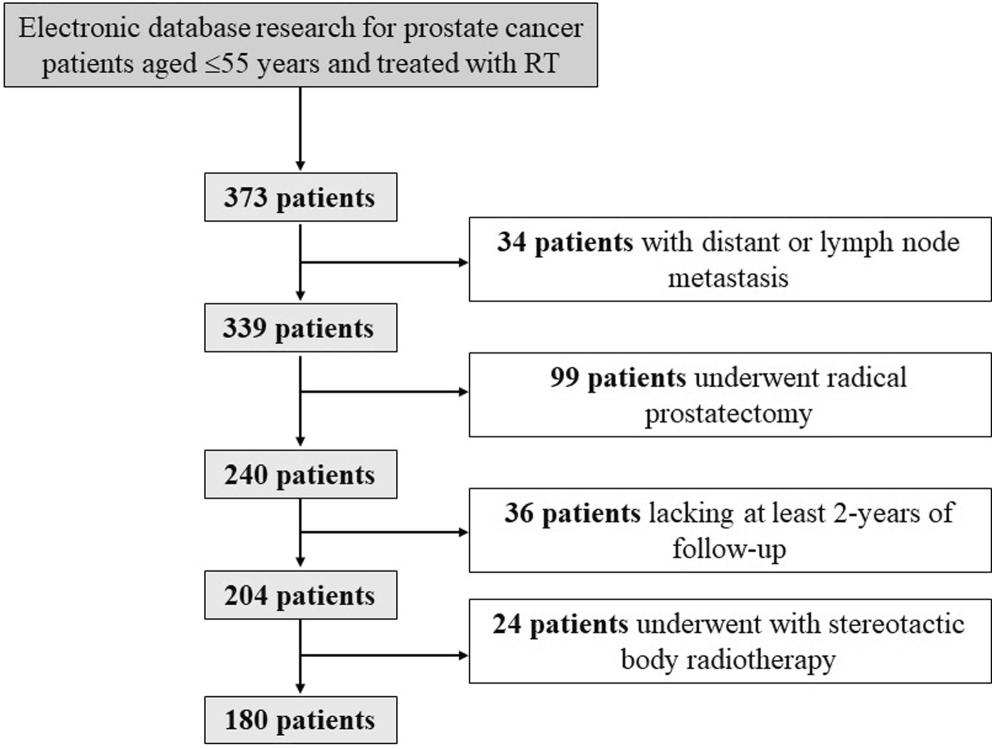
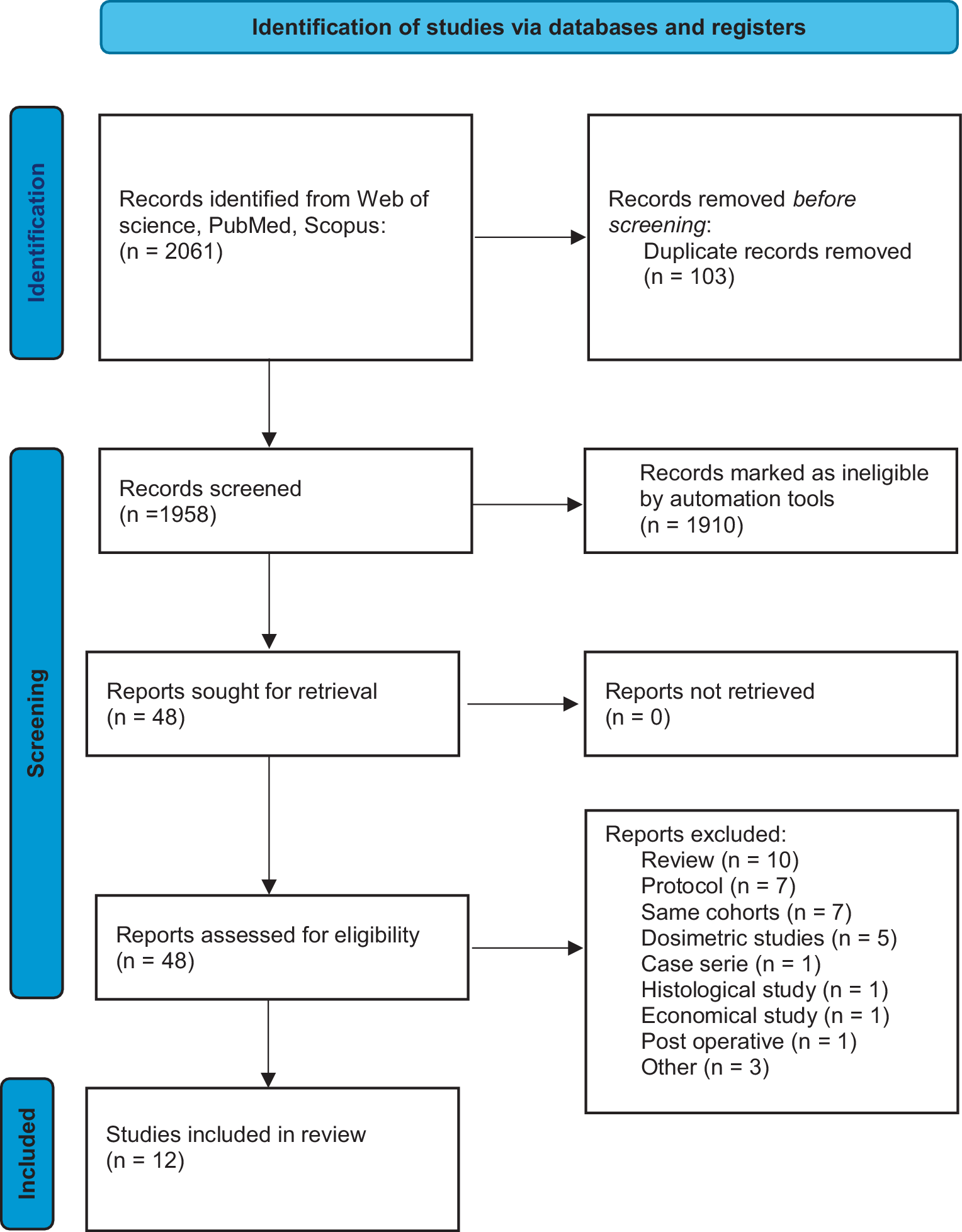
Initially, the 266 included patients were categorized into four groups based on their treatment methods. The median time from first diagnosis of BM to treatment was 1 month (0–9 months). There were 42/501 lesions of > 10 cc, 645 patients with lung cancer BM in the institution, and 124 patients who did not match the pathological type of NSCLC. Moreover, there were 78 patients with no records of immunologic or targeted drug use, 120 patients who were still on first-generation or second-generation EGFR-TKIs, 57 patients who were lost to follow-up, and 266 patients who were eligible for the study. A total of 73 (27%) patients were treated with SRT-alone; 65 (24%) were treated with SRT combined with IT, 62 (23%) were treated with SRT combined with TT, and 66 (25%) were treated with SRT combined with IT and TT. The SRT combined IT and TT treatment group included two subgroups: one receiving first-line combined IT and TT before SRT and the other receiving oral TT before SRT followed by IT. However, there was no significant difference in the recurrence rates between the two subgroups. (P = 0.059).
Progression-free survivalA total of 42% (113/266) of patients included in the study developed intracranial progression, which included 76 patients who developed intracranial progression within 1 year, accounting for 67% of the patients who relapsed at the study endpoint. Of these, 35.5% (27/76) patients developed progression locally at the irradiated sites within 1 year and 64.5% (49/76) developed intracranial progression at distant sites without radiation within 1 year. Thirty-five patients who were newly diagnosed with BM underwent SRT therapy again, and the median follow-up time for PFS was 10.50 (0–36) months in SRT-alone group, 13.50 (0–35) months in SRT combined with IT group, and 13.75 (0–36) months in SRT combined with TT group. The median follow-up time in SRT combined with the IT and TT group was 14.75 (0–38) months. For these four different groups, SRT-alone, SRT combined with IT, SRT combined with TT, and SRT combined with IT and TT, the overall 12-month PFS was 49.73%, 65.89% (HR, 0.63 [95% CI: 0.32–1.24]. P = 0.183), 78.05% (HR, 0.38 [95% CI: 0.18–0.76]; P = 0.007), and 80.76% (HR, 0.32 [95% CI: 0.16–0.65]; P = 0.001) (Fig. 2). The 1‑year PFS of the local intracranial radiation site in these four groups were 77.89% (P = 0.239), 88.75% (HR: 0.607, 95% CI [0.251–1.465], P = 0.266), 88.01% (HR: 0.556, 95% CI [0.221–1.394], P = 0.210), and 91.97% (HR: 0.366, 95% CI [0.130–1.029], P = 0.057) (Fig. 3), respectively. The 1‑year PFS of new intracranial (distant intracranial failure outside of the radiotherapy site) BM in the respective groups were 63.96% (P = 0.039), 74.17% (HR: 0.726, 95% CI [0.417–1.264], P = 0.258), 88.70% (HR: 0.480, 95% CI [0.253–0.908], P = 0.024), and 87.81% (HR: 0.459, 95% CI [0.246–0.858], P = 0.015) (Fig. 4). Patients treated with SRT combined with IT and TT displayed better PFS than those treated with SRT-alone, SRT combined with IT, and SRT combined with TT.
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4
Figure 2 shows the overall intracranial PFS. The 1‑year PFS rate for SRT-alone was 49.73%, that for SRT combined with IT group was 65.89% (HR 0.63 [95% CI: 0.32–1.24]; P = 0.183), that for SRT combined with TT group was 78.05% (HR 0.38 [95% CI: 0.18–0.76]; P = 0.007), and that for SRT combined with both IT and TT was 80.76% (HR 0.32 [95% CI: 0.16–0.65]; P = 0.001).
Figure 3 depicts local radiation-range recurrence in different treatment modalities. The 1‑year PFS for local recurrence at the radiation site was 77.89% for SRT-alone (P = 0.239); 88.75% for SRT combined with IT (HR: 0.607, 95% CI [0.251–1.465], P = 0.266); 88.01% for SRT combined with third-generation EGFR-TKIs (HR: 0.556, 95% CI [0.221–1.394], P = 0.210), and 91.97% for SRT combined with both IT and third-generation EGFR-TKIs (HR: 0.366, 95% CI [0.130–1.029], P = 0.057).
Figure 4 depicts distant intracranial recurrence beyond the local radiation range. For new intracranial metastases, the 1‑year PFS was 63.96% for SRT-alone (P = 0.039); 74.17% for SRT combined with IT (HR: 0.726, 95% CI [0.417–1.264], P = 0.258); 88.70% for SRT combined with third-generation EGFR-TKIs (HR: 0.480, 95% CI [0.253–0.908], P = 0.024); 87.81% for SRT combined with both IT and third-generation EGFR-TKIs (HR: 0.459, 95% CI [0.246–0.858], P = 0.015).
Tumor intracranial objective response rateOnly 5% of the patients in the SRT-alone group achieved CR at a median time of 8.9 (3–13.5) months, 12% of the patients in the SRT combined with IT group achieved CR at a median time of 6.25 (2–16) months, and 24% of the patients in the SRT combined with TT group achieved CR at a median time of 8.2 (1–17) months. In addition, 26% of the patients in the SRT combined with IT and TT group achieved CR, and the median time to CR was 14 (1–22) months, which was longer than that in the other treatment groups. This difference could be attributed to the higher baseline tumor volume in the SRT combined with the dual therapy group. The tumor IORR in the SRT-alone group was 32% (95% CI: 21–42) (Fig. 5a); in the SRT combined with IT group, the IORR was 46% (95% CI: 34–59, OR 0.54 [95% CI: 0.27–1.07], P = 0.08) (Fig. 5b); in the SRT combined with TT group, the IORR was 58% (95% CI: 45–71, OR 0.33 [95% CI: 0.16–0.67], P = 0.002) (Fig. 5c); and in the SRT combined with IT and TT group, the IORR was 61% (95% CI: 49–73, OR 0.32 [95% CI: 0.16–0.64], P = 0.001) (Fig. 5d). The IORR of patients treated with SRT combined with IT and TT was higher than that of patients in the other groups, which indicated that the combination therapy markedly increased the IORR of the tumor (Table 2). Figure 6 provides the image of a patient in whom CR was recorded at the last follow-up.
Fig. 5
Objective response rate of intracranial tumors
Table 2 BM response of different treatments assessed by BICRFig. 6
Figure 5 presents the IORR of four different treatments, including a visual comparison of CR PR SD PD of every group. (a) The application of SRT-alone; (b) SRT combined with IT monotherapy; (c) SRT combined in the application of third-generation EGFR-TKIs; (d) SRT combined with both IT and TT.
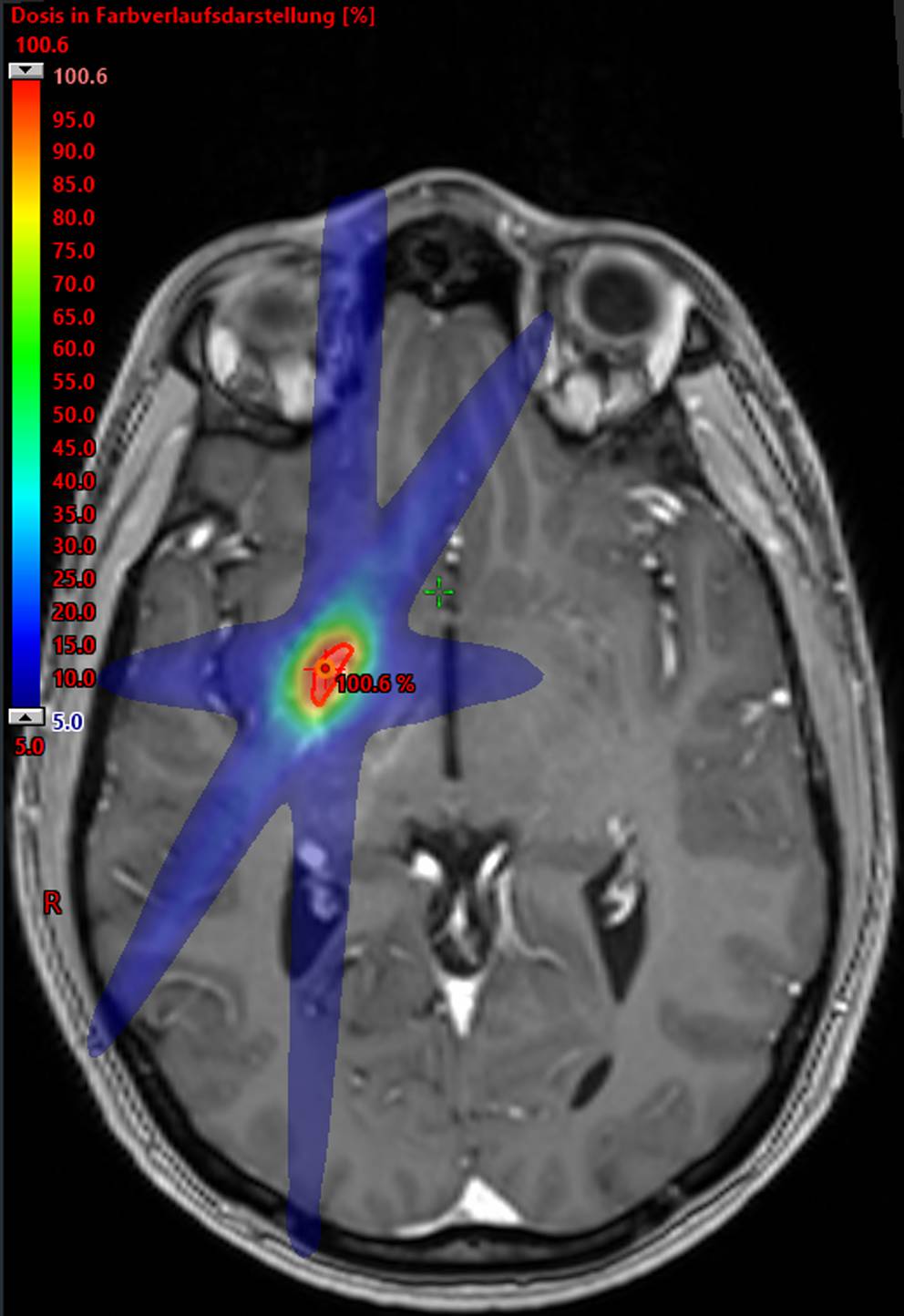
Figure 6 illustrates a patient with BM associated with NSCLC. Following the initial discovery of BM via MRI, SRT was promptly administered. The patient subsequently commenced regular oral administration of osimertinib in conjunction with treatment with the IT agent, avelumab. At the 7‑week follow-up, a reduction in tumor volume and a decrease in the peritumoral edema were recorded. By the 36-week follow-up, the tumor had completely regressed with no residual lesions, and the peritumoral edema had subsided, achieving a CR.
Disease control rate of BMIDCR was defined as the proportion of intracranial lesions that achieved CR, PR, and SD after treatment. In those treated with SRT-alone, IDCR was 44% (95% CI: 32–55), whereas patients treated with SRT combined with IT achieved an IDCR of 52% (95% CI: 40–65, OR 0.71 [95% CI: 0.36–1.39], P = 0.321). In patients treated with SRT combined with TT, the IDCR was 66% (95% CI: 54–78, OR 0.40 [95% CI: 0.20–0.81], P = 0.010) and in those simultaneously treated with SRT combined with IT and TT, the IDCR was 71% (95% CI: 60–82, OR 0.34 [95% CI: 0.17–0.68], P = 0.002). Furthermore, the IDCR in the SRT combined with IT and TT group surpassed that of patients treated with SRT-alone or SRT combined with either IT or TT (Table 2).
Comments (0)