
Remember me




This was a retrospective, observational single centre study at the Guys and St Thomas’ NHS Foundation Trust Hospital. Between July 2016 and April 2024, there were a total of 380 standalone ASD closures, of which 29% were performed surgically. During this period, a total of 33 selected patients underwent fluoroscopy-free transcatheter ASD closure using either the conventional approach (Group 1) or the simplified superior vena caval approach (Group 2).
Procedure characteristicsAll procedures were performed in our congenital cardiac catheterisation laboratory under general anaesthesia. Intravenous heparinisation at 100 units/kg and prophylactic flucloxacillin or teicoplanin (in the case of penicillin allergy) were given as routine practice. Systematic transoesophageal echocardiography (TOE) assessment at 0o, 30o, 60o, 90o and 120o views were used to determine the size of the defect and assessment of rims for suitability for device closure. Patients who were considered to require balloon sizing of the ASD or had multiple defects were excluded from having a fluoroscopy-free procedure. In all the patients, only femoral venous access was obtained. A device size of 0–4 mm larger than the greatest diameter on TOE was chosen prior to percutaneous access.
Group 1 patients had the procedure performed using the well-described technique similar to the normal fluoroscopy-guided ASD closure. A multipurpose catheter was manipulated across the ASD into the left atrium or pulmonary vein under TOE guidance. This was exchanged for an Amplatz 0.035” Extra-stiff guidewire (Cook Inc., Bloomington, IN, USA), which facilitated passage of the delivery sheath into the left atrium and pulmonary vein. The ASD device was deployed across the septum in the traditional way under TOE guidance.
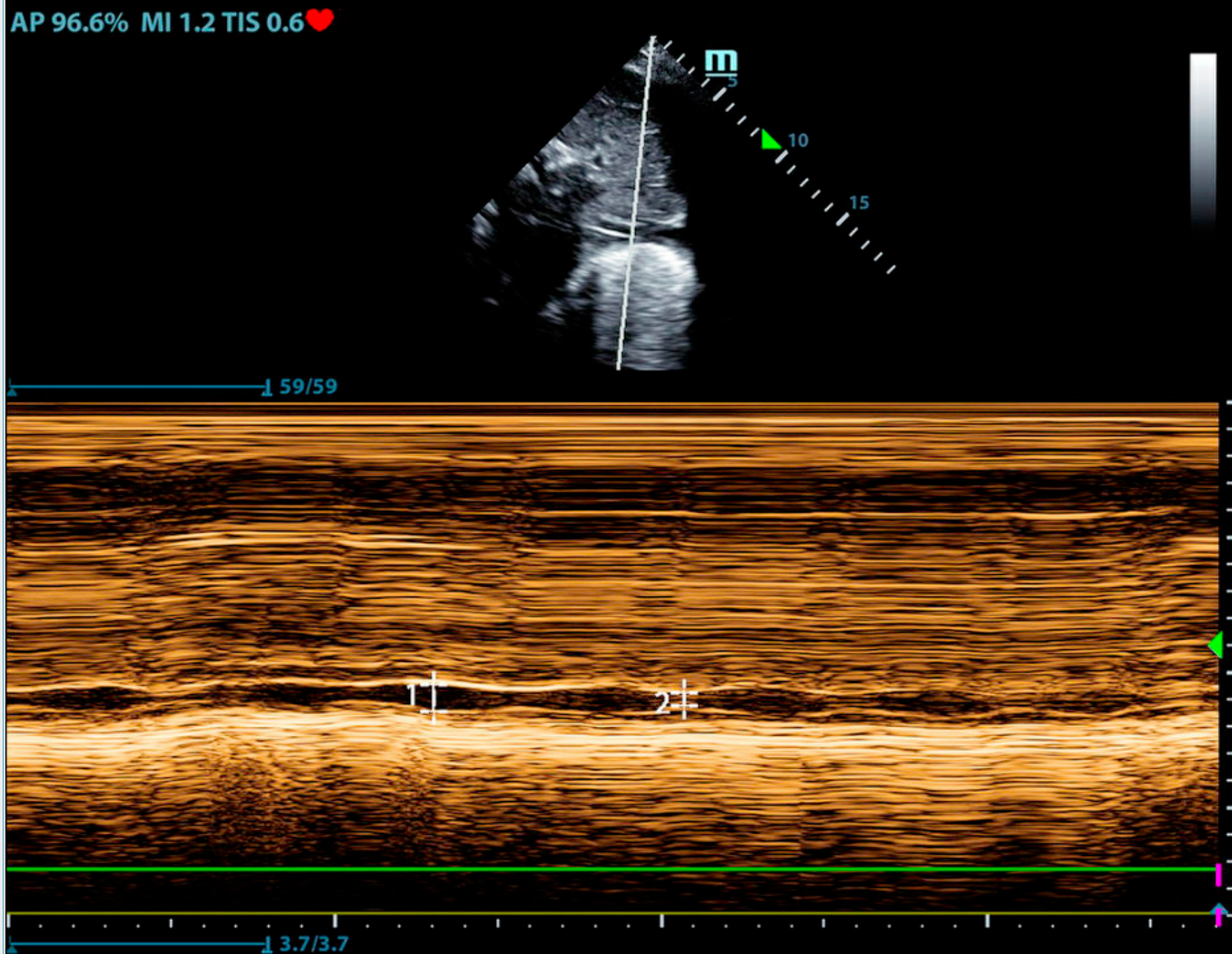
Group 2 patients underwent a modified procedure (Fig. 1), whereby an Amplatz 0.035” Extra-stiff J-tip guidewire was advanced directly to the SVC followed by an appropriately sized sheath for the delivery of the device (Video 1). The wire and dilator were removed, and the selected septal occluder was advanced through the sheath, so that a small portion of the left atrial disc was extruded from the end of the sheath in the SVC to form an ‘onion’, easily visible on TOE (Video 2). The delivery sheath/device assembly was then withdrawn and manoeuvred across the ASD into the left atrium (Video 3) and the device was deployed and released in the usual way.
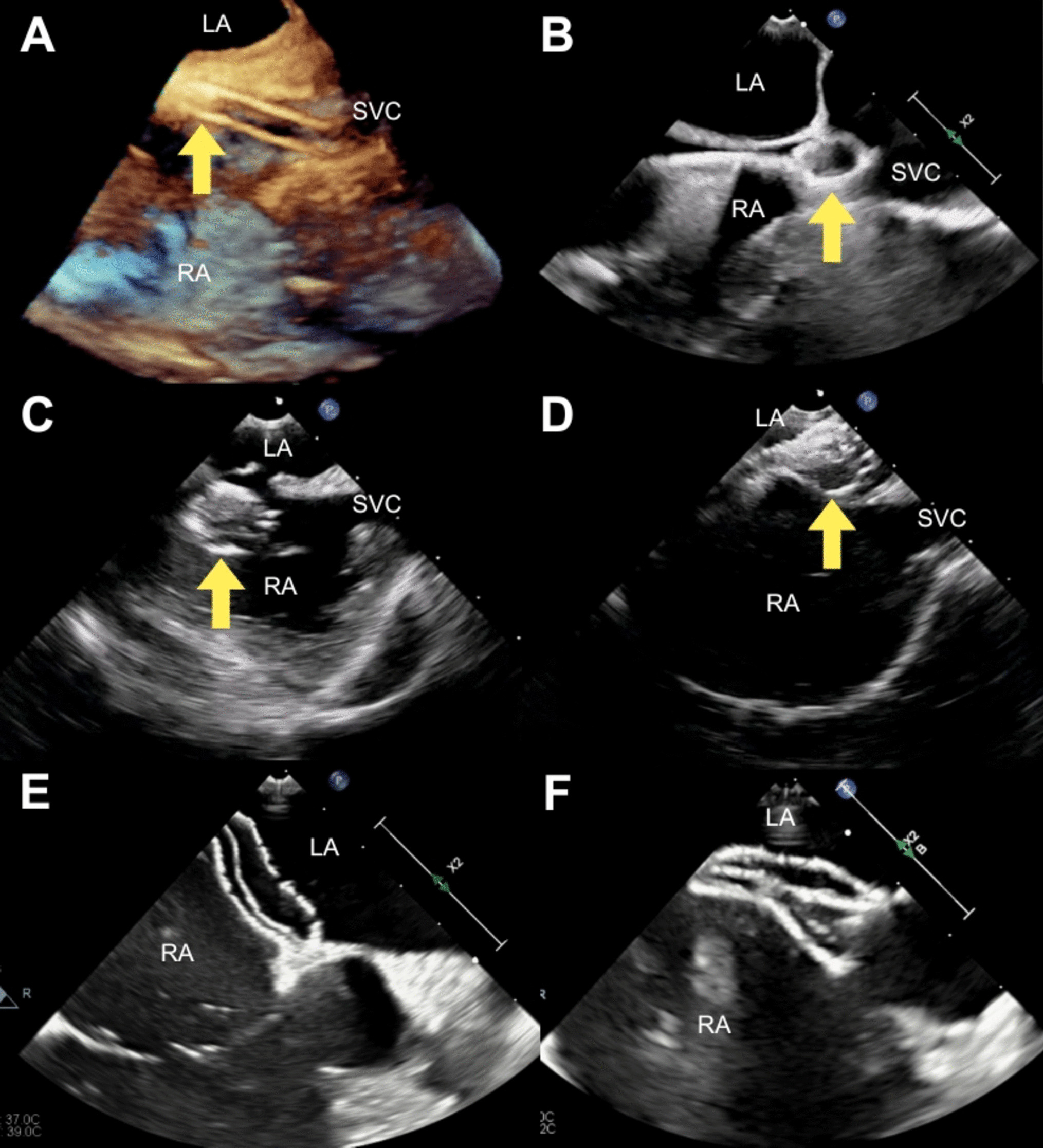
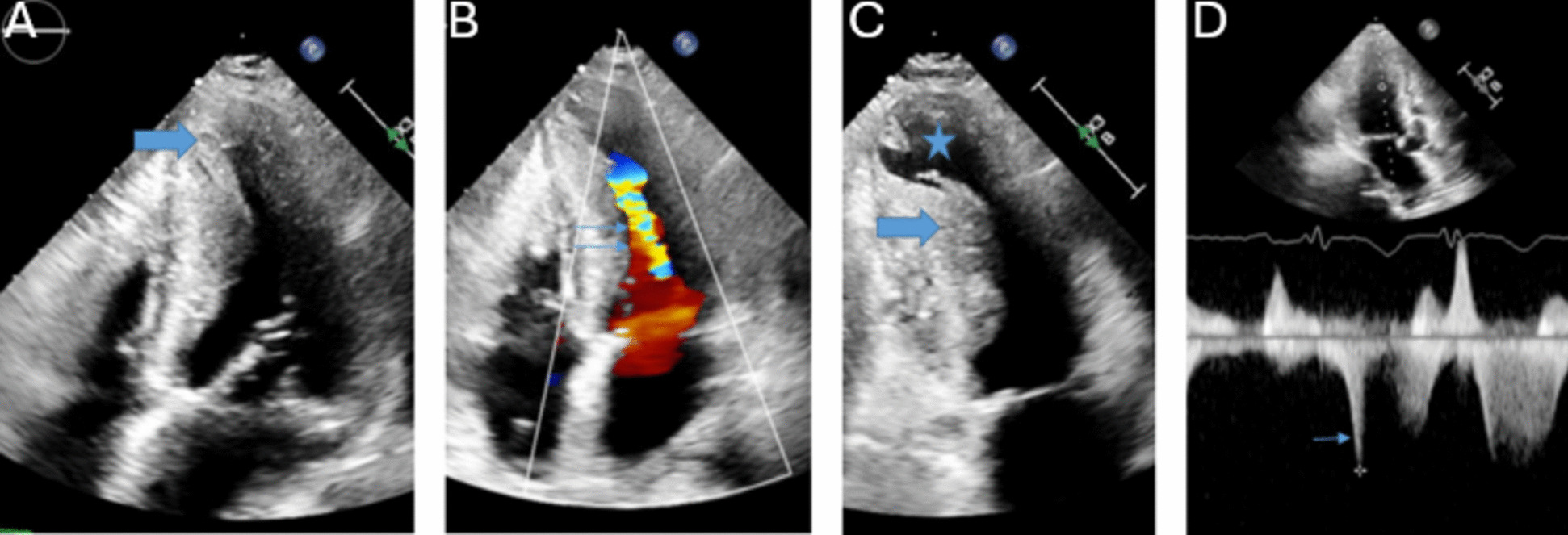
Fig. 1
The modified procedure. (A) A 3D transoesophageal echocardiogram image shows the ASD occluder (arrow) advanced within the delivery sheath in the SVC. (B) A small portion of the left atrial disc of the occluder (arrow) is extruded from the end of the sheath in the SVC to form an ‘onion’. (C) The ‘onion’ and delivery sheath assembly (arrow) is rotated towards the ASD. (D) The ‘onion’ and delivery sheath assembly (arrow) is manoeuvred across the defect into the left atrium. (E) The left atrial disc is deployed and positioned. (F) The right atrial disc is deployed in the usual way. Key: SVC: superior vena cava; RA: right atrium, LA: left atrium
An Occlutech Figulla Flex II (Occlutech International, Helsingborg, Sweden) was used in 26 patients (9/9 in Group 1, and 17/24 in Group 2), Amplatzer Septal Occluder (Abbott Medical, St. Paul, MN, USA) in 5 patients (in Group 2), Cocoon Septal Occluder (Vascular Innovations Co., Nonthaburi, Thailand) in 1 patient (in Group 2) and CeraFlex ASD Closure System (Lifetech, Shenzhen, China) in 1 patient (in Group 2).
Final assessment was made with TOE including assessment of stability with a push-pull manoeuvre (the Minnesota wiggle) and the device was released. Haemostasis was achieved either by manual compression or Perclose ProStyle suture (Abbott Medical, St. Paul, MN, USA) depending on patient suitability and operator choice. A transthoracic echocardiogram was performed prior to discharge to assess immediate procedural success and exclude any complications. All patients received aspirin 5 mg / kg (maximum dose 75 mg daily) for 6 months and the initial follow-up was conducted after 2 months.
Ethics and statistical analysisThis retrospective analysis was approved by the Guys & St Thomas NHS Trust Audit Committee. All patients, parents or legal guardians granted their informed consent for the procedure.
Statistical analysis was performed in Stata 18.0. Chi-squared tests was used for categorical variables and student t test or Mann Whitney-U was used for numerical variables. A p-value < 0.05 was considered statistically significant.
Comments (0)