
Remember me



This animal study was designed following the ARRIVE guidelines [15]. The protocol of this study was carried out according to the ethical principles approved by the international committees for the protection of laboratory animal rights and was approved with the ethics code IR.KMU.AEC.1401.012.
Forty healthy adult male rats aged between 92 and 105 days and an approximate weight of 250 to 300 g were obtained from the Laboratory Animal Care and Breeding Center of the Faculty of Medicine, Kerman University of Medical Sciences. The rats were kept in standard laboratory conditions (ambient temperature 22 ± 2 °C, humidity 55 ± 5%, and a 12-hour light-dark cycle) with free access to standard food and water (Nuvilab CR-1, PR, Brazil).
The sample size of 8 in each group was determined by G power software with α = 0.05 and β = 0.80 [13, 16]. So, using block randomization, 40 rats (each with two critical size defects (CSDs), one for allograft and the other for xenograft groups) were initially divided into 5 groups of 8 each. Each group then received one of the interventions (no hydration of bone graft, 2-minute saline hydration, 10-minute saline hydration, 30-minute saline hydration, and 2-minute blood hydration).
Five-mm CSDs were created on either side of the sagittal plane in the calvaria of the rats, and a number was assigned to each rat. In each rat, the right defect was filled with 150–1000-micron corticocancellous FDBA powder (A) (Cenobone®, Hamanand Saz Baft Kish, Iran) and the left defect with xenograft particles (B) (Cerabone® granules, Botiss, Germany) with the size of 0.5–1 mm (Fig. 1). All rats were quarantined for 7 days before the start of the experiment. The animals were kept under NPO conditions for 3 h and were prevented from drinking water for 2 h before surgery.
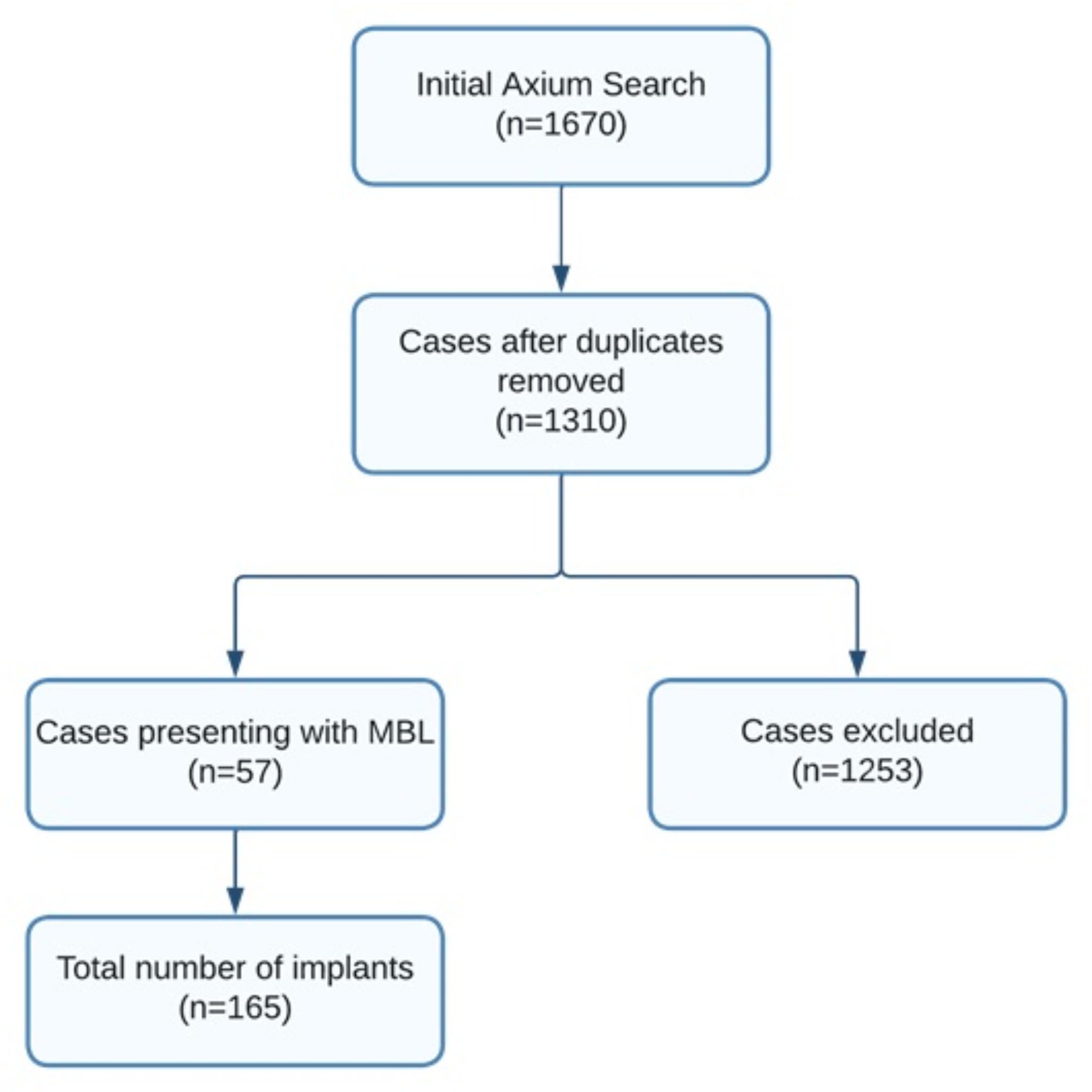
Fig. 1
Flow chart of the study groups
Surgical proceduresIn order to induce anesthesia, ketamine (Ketamine, Alfasan, Woerden-Holland) (65 mg/kg) and xylazine (Xylazin 2%, Alfasan, Woerden-Holland) (7 mg/kg) were used intraperitoneally, and if necessary, anesthesia was continued with 0.25–0.5% isoflurane with 1 L per minute oxygen. The principles of sterility were followed for the surgeon’s hands, the surgical site, and the surgical instruments.
An autoclaved 3-inch stocking was rolled over the rat using aseptic techniques, and the head was pulled out. A No. 40 blade was used to carefully shave the calvarium area and then the area was scrubbed using betadine 7.5% (brown betadine). Then the intended area was disinfected again with 10% betadine solution (green betadine). In order to keep the rat’s head fixed during surgery, it was placed in a rodent stereotaxic device. An incision was made on the mid-sagittal skin using a No. 15 blade. Then, the full-thickness flap was carefully removed by a Molt #9 periosteal elevator (Smart Instru Molt elevator, Pakistan). Two CSDs were created on the calvaria at a distance of 3 mm from the midline on each side, 5 mm in diameter and 2 mm in depth, using a trephine bur (Trephine Bur Dentium, Korea). During the drilling, the surgical area was continuously washed with saline to prevent tissue damage, and great care was taken to avoid damage to the durameter and the fibrous connections attached to the inner surfaces of the cranial bone. the wound was washed with saline and the bone particles were removed by suction [17, 18]. FDBA was used in right cavity in each rat (groups A1 to A5) and xenograft bone was used in left cavity (groups B1 to B5). In each group, the cavities were filled based on the allograft or xenograft hydration method as follows:
1.No hydration– Control group.
2.Two minutes of hydration with 0.9% sterile saline (Darupakhsh, Iran).
3.Ten minutes of hydration with 0.9% sterile saline (Darupakhsh, Iran).
4.Thirty minutes of hydration with 0.9% sterile saline (Darupakhsh, Iran).
5.Two minutes of hydration with blood (blood was obtained from the bone defect site using an insulin syringe).
Then approximately 0.1 cc graft material to fill up to the outer surface of the bone edge was placed in the cavities slowly and without pressure so that the particles did not enter the meningeal space.
After placing the materials into the defects in different groups, the periosteum was returned and sutured in place using a simple single pattern using a 4 − 0 polyglycolic acid suture (Supa, Iran). Then, the skin was sutured using a 3 − 0 nylon suture (Supa, Iran) with a simple single pattern. The surgical area was disinfected with betadine, and tetracycline antibiotic ointment and bandaged. The animal was taken to a warm place to recover from anesthesia. Then, they were transferred to their cages and given food and water. In order to prevent possible infections, 5 mg/kg enrofloxacin 10% (Enrofan, Erfan darou, Iran) and 1 mg/kg keptoprofen 10% (Keptofen, Razak Labratories, Iran) were administered intramuscularly twice a day for first week after surgery and once a day for the second week in all groups. The animals also had free access to standard water and food (Nuvilab CR-1, PR, Brazil). The skin sutures were pulled ten days after the operation.
Histological analyses8 weeks [10] after surgery block sections including the area of the original surgical defects were removed and a code based on the number of the rat and type of bone graft was assigned to each sample. The samples were fixed in 10% formalin solution for 3 to 5 days. The decalcification process was done using 10% nitric acid for about 1 to 2 weeks. The acid was changed every day, and this process continued until the bone softened. After the necessary decalcification, the sample was cut with a scalpel and prepared using a tissue processor machine. This preparation takes 16 h and consists of 3 stages of dehydration, clearing with xylenol, and embedding in molten paraffin. Molding was done by an L-shaped aluminum mold with melted paraffin. Then a cut was made using a microtome device with a thickness of 3 to 5 mm in a tissue bath at 55 °C. After deparaffinization, staining with hematoxylin and eosin was done.
The prepared slides were coded, and evaluation was done by a pathologist who was blind to the studied groups.
The histology of the samples was examined using an Olympus YX-100 optical microscope (made in Japan). In this examination, all samples were examined in terms of new bone formation, remains of graft particles, evidence of acute and chronic inflammation, and granulomatous inflammation in response to the foreign object.
Histomorphometric examinationIn order to perform histomorphometric evaluation, micrographs were prepared from each slide under a Nikon-50 optical microscope (made in Japan) connected to a camera. For each sample, one micrograph at 40x magnification was prepared, and histomorphometric analysis was performed on this micrograph. Some micrographs were also prepared at 100x and 400x magnification from various parts of the lesions.
The micrographs were coded according to the slide code and stored in the computer for evaluation using Image J software. The surface of newly formed bone, remains of the graft particles, and soft tissue were calculated. In the next step, the area of each part was divided by the total area and reported as a percentage (for newly formed bone, remains of graft particles, and soft tissue). Histomorphometric evaluation of all samples was done at 40x magnification and all samples were standardized in terms of length, width, and pixels.
In order to differentiate the newly formed bone from the rat’s own native bone, the following criteria were used:
1.Absence of organized mature lamellar bone.
2.Increase in cellularity and new vascularization.
3.Observation of numerous osteocytes.
4.More intense staining by hematoxylin than eosin.
The newly formed bone was differentiated from allograft or xenograft particles based on the presence of cells in living bone lacunae and difference in staining.
Statistical analysisThe general linear model (GLM) method was used to analyze the studied data according to the objectives of the study. In order to accurately compare the hydration groups according to the structure of the studied response variables, both multivariate and univariate modes were used in this model. Bonferroni correction was also used for pairwise comparison of different groups. The normality of the distribution of the studied data was evaluated using the Shapiro-Wilk test and skewness and kurtosis values. Finally, according to the nature of GLM models, those variables whose distribution was non-normal were also included in this model after the proper conversion. In addition to the GLM model, the generalized estimating equation (GEE) model was also used to compare allograft and xenograft bone grafts. SPSS 22 statistical software was used with 0.05 as the significance level for this study.
Comments (0)