
Remember me
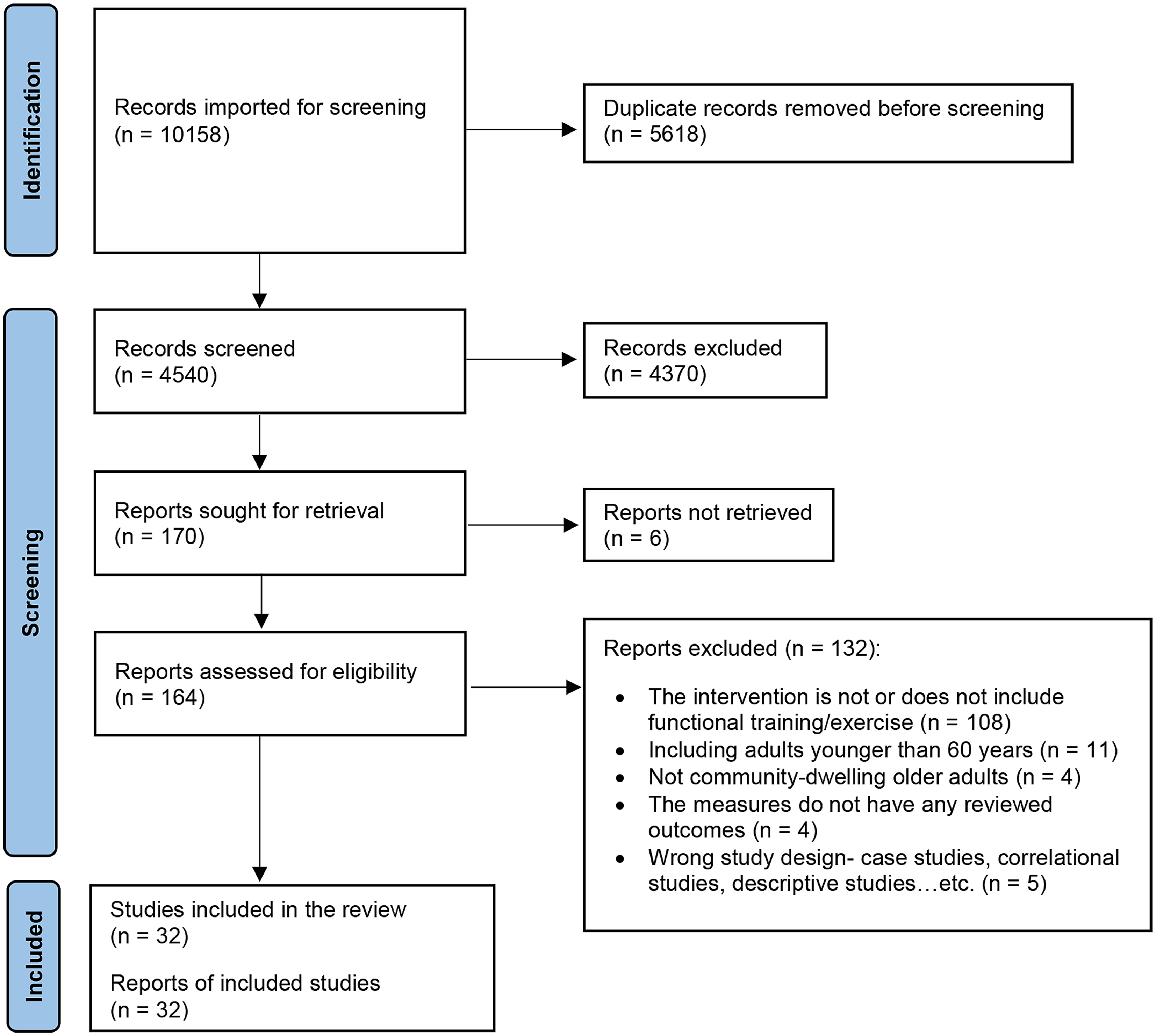

Of the 10,158 articles identified, 32 were included in the data analysis. The flowchart in Fig. 1 shows the screening process. Appendix C summarizes the research design, study participants and intervention characteristics, outcome measures, and relevant main findings of the included articles. Table 1 highlights the study and participant characteristics.
Fig. 1
Flow chart of the systematic review process
Table 1 Trial characteristics of all studiesCharacteristics of functional trainingThe training programs were categorized into three main categories: the single-component approach (n = 22), the multi-component approach (n = 8), and the dual-task paradigm approach (n = 2). The single-component approach focuses on exercise as the sole intervention, which could be functional training exercise alone or in combination with other types of physical exercises, such as resistance training. For example, the LiFE program integrates balance and muscle-strengthening exercises into everyday activities, and the 3-Step Workout for Life program combines resistance exercises with daily activity exercises [29, 30]. The multi-component approach includes other components in addition to exercise, such as combining exercises, home modifications, and caregiver support intervention with ADL training [31]. The dual-task paradigm approach requires participants to perform two tasks simultaneously, and at least one is a functional task. For example, maintaining balance while reading newspapers or carrying a tray with glasses [32].
The general intervention duration ranged from 40 to 60 min per session, with three sessions per week, and lasted 8 to 13 weeks. Healthcare professionals, such as physical or occupational therapists, typically delivered the intervention. The intervention could be home-based, center/hospital-based, or a combination of both.
Outcome measuresOutcome measures were categorized into ADL/IADL, physical functioning, and cognitive function. See Appendix D for the list of reviewed measures. Twenty-one studies measured personal ADL and/or instrumental ADL outcomes, predominantly self-reported or observation-based instruments, such as Katz’s ADL or Lawton IADL Scale. Twenty-four studies measured physical functioning, which was categorized into overall physical function (i.e., physical performance of the upper body and lower body together), lower body function (i.e., mobility or walking), upper body function (i.e., gross and fine motor hand function), and balance (i.e., static and dynamic balance). Lower body function, especially the Timed Up and Got test, is measured more often than upper body function and overall physical function. Ten studies measured cognitive functions, which were categorized into global cognitive function and domain-specific cognitive function. Global cognitive function assesses multiple domains of cognitive function concurrently, such as the Mini Mental State Examination or Neurobehavioral Cognitive Status Examination.
Methodology qualityTable 2 shows the PEDro scale results according to the functional training approaches and participants’ characteristics. The overall level of methodological quality of the studies included was fair, with a mean score of 4.84. Specifically, 47% of the studies achieved a score of 6 or higher, indicating good methodological quality.
Table 2 PEDro Scale RatingSummary of Key findingsGeneral community-dwelling older adultsTwenty studies recruited older adults without specifying their cognitive or frailty status. Among these, 14 used a single-component approach, four used a multi-component approach, and two used a dual-task paradigm approach.
Single-component approach and ADL/IADL outcomes. Nine studies measured ADL/IADL outcomes [29, 30, 33,34,35,36,37,38,39]. Six studies compared the single-component approach with a control group or another active intervention, such as structured resistance or balance exercise, and five reported a significant outcome [29, 33, 36, 37, 39]. The other three studies examined the effect using a pretest-posttest design, and two from the same research group showed a significant improvement [30, 38]. In summary, there is strong strength of evidence that single-component functional training can improve or maintain ADL/IADL performance in general community-dwelling older adults.
Among the seven studies with a significant outcome, two examined the LiFE program [29, 33] and three examined the 3-Step Workout for Life program [30, 38, 39]. Another two studies applied task-specific training which consisted of exercise linked with the participant’s home environment [37] and simulated daily activity training [36].
Single-component approach and physical functioning outcomes. Eleven studies measured physical functioning [29, 30, 33, 35, 38,39,40,41,42,43,44]. Seven studies compared functional training with a control group or another active intervention [29, 33, 35, 39, 40, 43, 44], and none reported a difference except three studies that reported an improvement in balance or mobility [29, 33, 44]. Two of the three studies examined the LiFE program.
The other four studies applied a pretest-posttest design [30, 38, 41, 42]. These studies measured lower body performance, but the results were mixed. The results were also mixed in two studies that measured upper body performance [30, 38]. Three studies measured mobility outcomes, and all showed a positive effect [30, 41, 42]. Two studies measured balance, and both showed a positive effect [41, 42]. In summary, there is moderate strength of evidence for using functional training as a single-component approach to improve balance and mobility in general community-dwelling older adults. However, the effect may not be greater than other structured exercise or usual care programs.
Multi-component approach and ADL/IADL, physical functioning, and cognitive function outcomes. The intervention components in the four multi-component studies varied and might include structured exercise, fall prevention education, home modification recommendations, home exercise programs, motor imagery training, and/or caregiver support in addition to functional training [31, 45,46,47]. Two studies measured ADL/IADL outcomes [31, 45]. One was a pretest-posttest trial and showed a significant improvement [31]. The other was an RCT [45], which compared multi-component functional training with a center-based exercise program. The study did not show a superior effect of the multi-component functional training. This study also measured global cognition but did not find an effect.
Three studies measured physical functioning outcomes [45,46,47]. All were RCTs. One trial compared multi-component functional training to a center-based exercise program, as aforementioned [45]. However, the trial found a superior effect on hand dexterity in a center-based exercise program. The second trial compared multi-component functional training to attention controls and found a superior effect of functional training on balance but not mobility [46]. The third trial compared multi-component functional training and single-component functional training with fall prevention education [47]. The trial found that both trainings improved physical functioning outcomes, but the improvement in multi-component functional training was greater. In summary, there is low strength of evidence of multi-component functional training on ADLs/IADLs and physical functioning.
Dual-task paradigm and physical functioning and cognitive function outcomes. Two studies applied the dual-task paradigm approach [32, 48]. Both studies compared dual-task functional training with a control group. One study showed an improvement in gait speed [32]. The other study did not show a superior effect on mobility [48]. Additionally, one of the studies measured cognitive function but did not find an effect [48]. Overall, findings from the two studies are not sufficient to make a conclusion about the effect of dual-task paradigm functional training.
Community-dwelling older adults with mild cognitive impairmentFive studies included older adults with mild cognitive impairment. Four of these studies used a single-component approach. One study used a multi-component approach.
Single-component approach and ADL/IADL and cognitive function outcomes. Four studies examined the same single-component approach, called Simulated Functional Tasks Exercise [17,18,19, 49]. The training program involved sorting cups and bowls while following specific rules and specific movement patterns to stimulate working memory and executive function. All studies showed an improvement in the ADL/IADL outcomes, including three pretest-posttest studies [18, 19, 49] and one RCT, which compared the program to a computer-based cognitive training program [17]. Furthermore, improvements were detected in overall cognitive function, memory, problem-solving, and executive function. Single-component functional training seems beneficial for improving ADL/IADL performance and cognitive outcomes in older adults with mild cognitive impairment. However, the strength of the evidence was regarded as moderate due to certain limitations. All four studies were conducted by the same research group and investigated the same functional training program. Furthermore, three of these studies applied a single-group pretest-posttest research design.
Multi-component approach and ADL/IADL and cognitive function outcomes. Only one study applied a multi-component approach [50]. The approach involved VR-based physical and cognitive training using everyday tasks, such as window cleaning and food preparation. Compared with combined multimodal exercise and cognitive training, the intervention had positive effects on IADLs but not on global cognition, memory, or executive function.
Community-dwelling older adults with dementiaTwo studies recruited older adults with dementia and used a single-component approach. Additionally, two other studies recruited older adults with dementia or mild cognitive impairment and used a multi-component approach.
Single-component approach and ADL/IADL and physical functioning outcomes. Function training in one study focused on functionally relevant muscle groups and ADL-related motor functions, such as stair climbing [51]. This intervention was more effective in improving lower body function, mobility, and balance than low-intensity multimodal exercise in older adults with dementia. Another study applied simulated locomotion and ADLs to people with dementia [52]. There were no significant differences in ADLs, balance, overall physical function, or global cognitive outcomes when compared to a social gathering group.
Multi-component approach and ADL/IADL, physical functioning, and cognitive function outcomes. One study combined sensorimotor exercise, cognitive training, and ADLs as activations [53]. Compared to usual care in daycare centers, the multi-component approach group significantly maintained ADL function and global cognition. The other study combined physical exercise, daily activities, community participation, risk enablement (positive risk taking), and environmental assessment [54]. Although the multi-component intervention group did not outperform a simple fall prevention group on the outcomes of ADLs/IADLs, balance, and mobility, the intervention yielded better outcomes in executive function and visual-spatial working memory. In short, the strength of evidence for multi-component functional training for people with dementia is low because of limited studies and mixed results.
Community-dwelling older adults with frailtyThree studies recruited older adults using frailty-specific screening criteria and all were RCTs. Two studies used a single-component approach, and one used a multi-component approach.
Single-component approach and ADL/IADL and physical functioning outcomes. Both studies applied multi-modal exercise. One combined tailored walking with activity exercises [55]. The study showed a superior effect on one of the physical functioning tests of the lower extremities (i.e., 6-minute walk) when compared to an educational control group. The other combined strength training, endurance, balance, and flexibility exercises with ADL training [56]. The group improved in ADLs and all lower extremity physical functioning measures but not in IADLs after program completion. There was low strength of evidence that single-component functional training can improve the physical functioning of the lower extremities for frail older adults.
Multi-component approach and ADL/IADL and physical functioning outcomes. The study combined medication use and safety and nutritional status optimization with exercise and ADL training, such as walking outdoors and shopping [57]. Compared to a control group, the intervention did not have a superior effect on the ADLs or the physical functional outcomes.
Comments (0)