
Remember me


Recent advances in mechanical ventilator monitoring allow for the assessment of advanced pulmonary mechanics, which can evaluate the impact of ventilator adjustments to optimize patient care. Of particular interest is the ability to measure expiratory time constant (RCEXP) to enhance adjustments in tidal volume (VT), positive end-expiratory pressure (PEEP), respiratory rate (RR), and, consequently, minute ventilation. This holds true mostly using closed-loop system adaptive modes of ventilation [1]. The goal is to minimize dynamic hyperinflation and its impact on both lung stress–strain and hemodynamic impairment from intrinsic PEEP. Although the concept of pulmonary time constants dates back to the 1950s, perhaps its most significant application was introduced 20 years ago with the advent of closed-loop intelligent ventilation platforms. [2].
This narrative review provides a brief orientation and history of this concept. It then defines expiratory time constant (RCEXP), including reference values and findings of different methods used to obtain it. The review also considers the behavior of RCEXP given different lung pathologies, including its conceptual limitations in light of these clinical investigations and the implications of these findings for patient management.
Brief history of pulmonary time constantsA time constant describes the equilibration characteristics of pressure, flow, and volume over time between two points in the patient–ventilator circuit. This theoretical model was based upon the simple premise of a constant pressure generator connected to a single compartment with fixed resistance and a compliance component. In other words, it describes passive pressure control ventilation, whereby a fixed airway pressure produces an exponential curve for changes in pressure, flow, and volume changes between the proximal airway and the alveoli [3, 4]. Although the time constant can be determined for both inspiration (i.e., the inspiratory time constant is essentially influenced by ventilator settings during the inspiratory phase) and exhalation, only the RCEXP is a result of passive elastic recoil of the lung and the chest wall. This distinction is important for understanding the respiratory mechanics of passive exhalation; therefore, this review will focus solely on RCEXP.
The distinct shape of any exponential curve is based upon two parameters that remain constant for any particular condition. First is the “amplitude constant,” which signifies the magnitude of the applied pressure driving ventilation at breath initiation (start of inspiration) or breath termination (start of exhalation). Second, the “time constant” represents the magnitude of inspiratory or expiratory volume with corresponding flow. The term expiratory time constant may be misleading and confusing as it should refer to a different portion of exhaled flow (and thus volume) during an exponential process per the same amount of time (hence the term constant). The time-constant concept, originally designed to explain the physiology of lung emptying, has major limitations when applied to patients with healthy or heterogeneous diseased lungs under mechanical ventilation. In this context, exhalation is influenced by components that introduce additional resistance, such as the endotracheal tube, the ventilation circuit's resistance, and the resistance of the mechanical ventilator expiratory valve. As a result of these complexities, the term expiratory time “constant", which was initially meant to indicate a consistent duration of defined parts of passive exhalation, does not accurately reflect the actual dynamics of airflow during exhalation in real-life clinical scenarios [5, 6].
Previous literature uses varying abbreviations for the expiratory time constant, often called ‘‘RCEXP’’ (the product of resistance and compliance), while the measured value is typically denoted by the Greek letter “tau” (τ). This review uses both terms interchangeably.
Definition and physiological basis of RCEXPRCEXP is a product of respiratory system compliance (CRS) and respiratory system resistance (RRS) with the resulting unit in seconds (Eq. 1) [7]:
$$ }_}}} = }_}}} \times }_}}} = \frac}_}} \left( } \right)}}}\left( }2}} \right)}} \times \frac}\left( }2}} \right)}}}}\left( }/}} \right)}} = \frac}_}} \left( } \right)}}}}\left( }/}} \right)}} = } \times \frac}}}} = } $$
(1)
where ΔP is the difference between plateau pressure and PEEP, pressure, V’ is expiratory flow, L—liters, s—seconds.
Exhalation is a mostly passive process utilizing the stored elastic energy from respiratory distension from inspiration to drive expiratory flow following the expected exponential decay. RCEXP represents the time when such exponential change would be complete if the rate of change were maintained at its initial level rather than decreasing [4]. In other words, it is the linear expression of a distinctly nonlinear phenomenon. Expressing τ as “incomplete” change (I) uses the base of natural logarithms (e) such that I/e = 100% ÷ 2.718 = 37%, and thereby completed change at 1τ would be 63%; at 2τ it would be calculated as 37% ÷ 2.718 or ~ 14% incomplete and ~ 86% complete, etc. Following such exponential kinetics, 63%, 86%, 95%, 98%, and 99% of VT are exhaled by one, two, three, four, and five τ, respectively [7, 8].
Interestingly, only “one” or the “first” RCEXP appears in most clinical studies, leaving the duration of the rest of the exhalation without numeric expression.
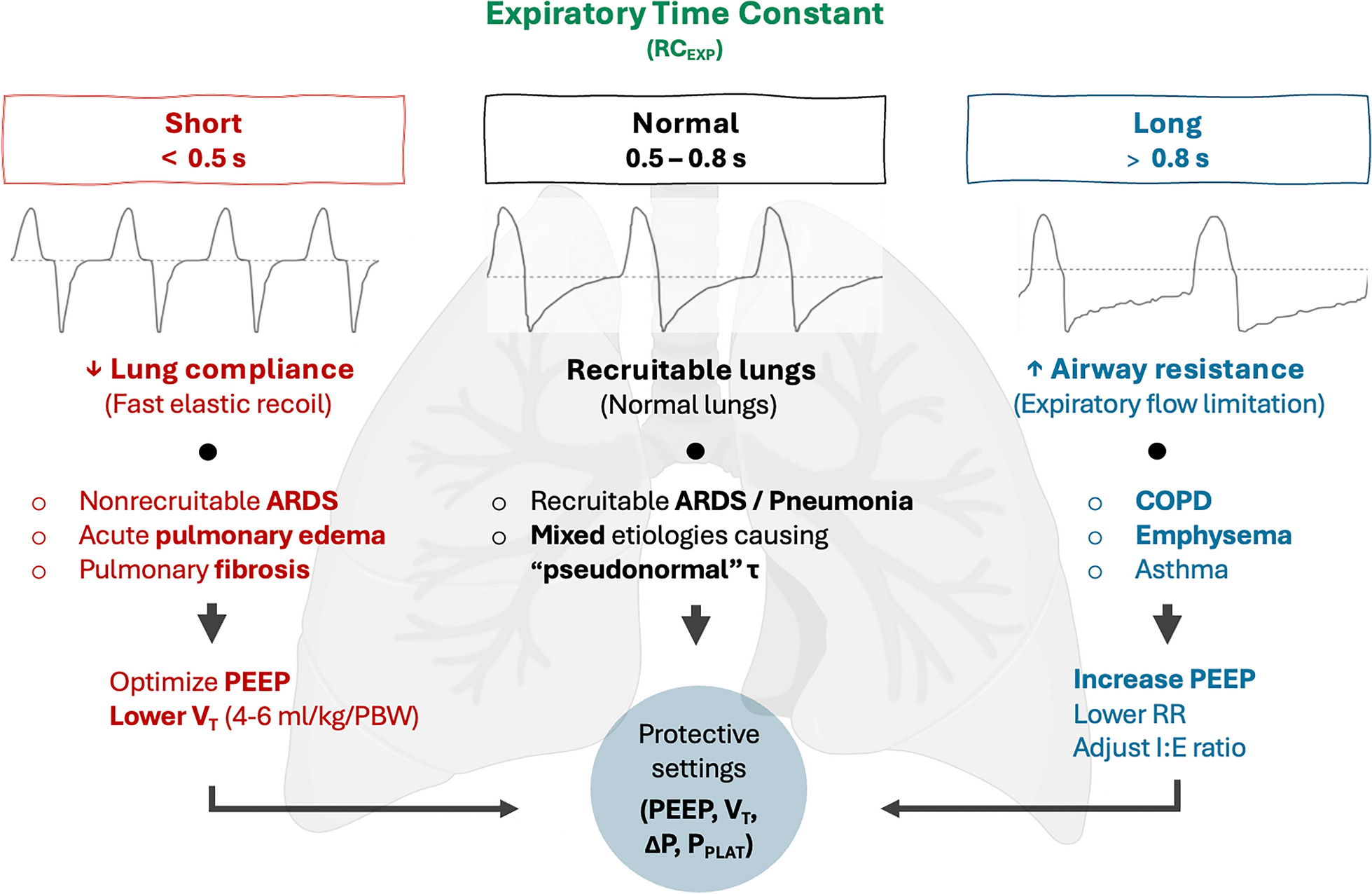
Reference values of RCEXPThe average reference values for adult patients with preserved lung function on invasive mechanical ventilation range between 0.5 and 0.8s, with a mean value of around 0.6s (Table 1) [2, 9,10,11,12,13,14,15,16]. However, coexisting pathologies may render RCEXP to appear normal (i.e., RCEXP pseudo-normalization). This may result from conditions associated with high RRS but low CRS. These values should be taken in context with set inspiratory variables, most notably VT and PEEP. Even in healthy postoperative patients without known previous lung disease, RCEXP slightly differs, depending on the applied methodology to obtain RCEXP [9,10,11,12, 14].
Table 1 Typical range of time constants in passive intubated patients with various disease statesThe importance of this concept is the following: [1] when RRS is held constant, equilibration time for flow, volume, and pressure is directly proportional to CRS (i.e., as CRS decreases with a stiffer/smaller lung, equilibration time also decreases), and [2] when CRS is held constant, equilibration also is directly proportional to RRS (i.e., as RRS increases, equilibration time is prolonged). In addition, the actual time needed for equilibration depends upon the magnitude of VT or associated driving pressure (ΔP) and PEEP. This provides the context in which time-constant values should interpreted. Table 2 summarizes the major RCEXP determinants in two common clinical entities—ARDS and COPD.
Table 2 Major RCEXP determinants in two common clinical entities—ARDS and COPDAs mentioned previously, by definition, a near-full exhalation should be completed in three-time constants (i.e., 95% of VT) [7]. However, due to the physics of pressure and flow equilibration over time, 95% of VT is exhaled sooner. The first, second, and third RCEXP are not equal but progressively shorter, with mean τ1, τ2, and τ3 of 0.6s, 0.4s, and 0.3s, respectively, regardless of whether pressure-controlled ventilation (i.e., variable flow) or volume-controlled (i.e., constant flow) ventilation was used [14]. The phenomenon described arises from the rapid decrease in airway pressure coupled with a more gradual reduction in airflow during the early phase of exhalation. As a result, the significant resistance introduced by the endotracheal tube (ETT) produces longer RCEXP during early exhalation but progressively declining RCEXP during later parts of exhalation, where ETT-induced resistance applies to a much lesser degree.
The concept of time constant deviates from reality, because both RRS and CRS change during either phase of ventilation. This is especially relevant during passive exhalation, because ΔP decreases with lung volume, while RRS increases (i.e., decreased in radial traction supporting peripheral airway patency). In addition, depending on the PEEP, CRS may change during exhalation resulting in progressive alveolar collapse. Therefore, using the single exponential model using single values or CRS and RRS to demonstrate RCEXP provides only an overall rough approximation of what is observed clinically [17].
Methods to determine RCEXPIn the context of a single-compartmental model, two linear equations have been proposed to calculate RCEXP. The first method involves calculating the product of CRS and expiratory resistance [7, 18]. The second method examines the change in VT during exhalation with the corresponding change in expiratory flow rate. The resulting RCEXP is determined by dividing VT by the peak expiratory flow (PEF). This method was initially described by Marini and later refined by Brunner (Eq. 3), who included a correction factor to account for incomplete exhalation [19]. The resulting RCEXP using these two methods are essentially the same, because the product of CRS and RRS equals the fraction of VT over PEF (Eq. 1):
where RE is expiratory airway resistance
The nonlinearity of the flow/volume waveform (V’/V curve) during passive exhalation indicates that expiratory flow starts at a relatively high rate in the early phase (i.e., PEF) and then decays exponentially. This decay signifies the combined effects of reduced ΔP and increased small airway resistance (i.e., diminished radial traction) as the alveolar volume decreases [20, 21]. In the latter part of exhalation, the flow becomes more linear. In certain pathological states, as in patients with small airway obstruction, such as COPD, this reflects the imposed resistance of the artificial airway, primarily the ETT [22,23,24].
In pulmonary disease, the shape of the V’/V curve varies. This reflects the different severity levels and the uneven distribution of lung compartments with differing resistances, volumes, and elastic recoil properties. In addition, these factors are further altered by the resistances introduced by the artificial airway and ventilator circuit. Thus, using a first-order linear model fails to capture the complexity of various lung pathologies [5].
Early physiological studies of passive lung emptying in paralyzed patients derived RCEXP from specific sections of the V’/V curve and the corresponding VT. This section of the V’/V curve is significantly transformed from primarily exponential to linear flow decay by evaluating the difference in flow between two-timepoints and their corresponding VT, as proposed by Aerts (Eq. 4), Lourens (Eq. 5), and others [9,10,11,12, 22, 25]:
$$_=\frac_}}}^}}}_- }}^}}}_-\text}}$$
(4)
$$_=\frac_}}}^}}}_- }}^}}}_-\text}}$$
(5)
RCEXP can also be measured directly from the start of exhalation until 63% of VT has been exhaled to obtain the first RCEXP [14,15,16, 26,27,28]. The advantage of such measurement compared to derived or calculated time constants is the ability to measure consecutive RCEXP (i.e., second, third, etc.) and, therefore, independently assess the physical characteristics of nearly whole (i.e., 95% VT) of the V’/V curve without needing to use “slicing” method and assess the time constant for each slice [14]. Reference ranges for RCEXP using various methods in postoperative patients are shown in Fig. 1.
Fig. 1
Physiological values of RCEXP in passive, healthy postoperative patients under pressure-controlled ventilation (PCV) and volume-controlled ventilation (VCV) using different methods to obtain RCEXP. The upper and lower limits of the reference range are displayed as dashed red lines [14]
With the advancement of electric impedance tomography and high-resolution computed tomography, it is also possible to detect regional RCEXP differences across the lungs [29, 30]. However, this aspect is beyond the scope of this review. Table 3 outlines the pros and cons of each method for determining RCEXP and its bedside application. Table 4 summarizes clinical studies with corresponding RCEXP values across different pathologies in adult human subjects.
Table 3 Pros and Cons of different methods to determine RCEXP and its clinical application at bedsideTable 4 Studies involving human subjects with various lung pathologies and their corresponding RCEXPThe RCEXP inequalities and non-linear modelingTheoretical modeling provides a basic insight into volume distribution across the compartments in the non-homogenous lung. Such models comprise more than one theoretical compartment. In their study, Chatburn et al. aimed to determine major factors influencing VT distribution and concluded that RCEXP was the primary factor determining VT distribution between the compartments [34]. Most pathologies requiring mechanical ventilation in clinical care encounter RCEXP inequalities, resulting in heterogeneous VT distribution [29, 35]. To counteract these effects, modulation of VT and PEEP—both major determinants of RCEXP—help equalize the homogeneity to redistribute VT across the lung, as elucidated further in the text.
The nonlinear methods for studying RCEXP measure its values throughout the exhalation to examine regional volume distribution and flow heterogeneity during tidal ventilation (i.e., the viscoelastic, resistive, and elastic properties of both the lung and chest wall) [24, 36]. This was achieved by dividing the expired VT into five equal-volume “slices” (hereafter referred to as compartments) [6, 23]. In this method, expired flow and volume are measured from an inflection point (i.e., the point of maximum slope following PEF on the V’/V curve). The rationale for doing so is that [1] RCEXP can only be calculated when the V’/V curve becomes more linear and [2] eliminate mechanical artifacts associated with the opening of the expiratory valve.
Parsing the V’/V curve into equal volume compartments facilitates the identification and characteristics of “fast” and “slow” (i.e., flow-limited) lung compartments. In doing so, RCEXP values can be calculated for each segment, as well as the mean RCEXP for the entire cycle [6, 31]. Multiple studies have evaluated the patterns of lung emptying in two common clinical scenarios—chronic obstructive pulmonary disease (COPD) and acute respiratory distress syndrome (ARDS).
Characteristics of RCEXP across volume compartments in COPDImportant findings regarding the effect of mechanical ventilation on RCEXP were described by Kondili et al. [23]. Based on their data at zero positive end-expiratory pressure (ZEEP), total RCEXP (i.e., including imposed resistance) increased during exhalation, with mean values τ ranging from 1.19s during the initial phase of expiration to 3.75s in the terminal phase: an increase of 2.56s (average change of 0.64s per volume compartment). When imposed mechanical resistance was removed as a factor, RCEXP of the respiratory system remained virtually unchanged. This is the result of expiratory flow limitation (EFL) caused by small airway collapse, making imposed resistances negligible in this patient population.
PEEP of 5 and 10 cmH2O had a noticeable effect on RCEXP, blunting the slope of the RCEXP curve between compartments. Specifically, at a PEEP of 5 cmH2O, the average τ decreased by 0.36s for compartments 2–4 (19–24%), with the greatest impact observed in compartment 5, where τ decreased by 1.6s (43%). PEEP of 10 cmH2O produced substantially greater reductions in RCEXP as the average τ decreased by 0.7s to 1.53s for compartments 2–5 (39–54%). Again, PEEP had its most pronounced influence on compartments 4 and 5, with an average reduction in τ of 2.17s (58%). In other words, PEEP reduced the heterogeneity of regional lung emptying (Fig. 2A).
Fig. 2
Effects of PEEP on RCEXP in terms of compartments in A patients with COPD—increasing PEEP levels reduces the heterogeneity of regional lung emptying and thus promotes exhalation. B patients with ARDS—effect of ZEEP (dotted lines) on τ of the total respiratory system including artificial airways (τ tot) and τ of the respiratory system alone (τ RS) and PEEP 15 cmH2O (dashed lines). COMP-1–5—compartments 1–5, ZEEP—zero end-expiratory pressure, PEEP—positive end-expiratory pressure, COPD—chronic obstructive pulmonary disease. Figures were reconstructed from the original study by Kondili et al. [23] (A), and Guttmann et al. [6] (B)
Lourens et al. studied RCEXP by comparing subjects with moderate and severe COPD under ZEEP conditions [22]. RCEXP was measured between compartments at 100%, 75%, 50%, and 25% of expired VT. When using the V’/V technique, RCEXP of the fast compartment (100–76% incomplete exhalation) was indistinguishable between severe and moderate COPD (τ of 0.85 and 0.79s, respectively). In contrast, pronounced differences were found between severe and moderate cohorts in the slower compartments (75–51%, 50–26%, and 25–0% incomplete exhalation), which τ increased from 0.85s in the fast compartment to 2.84s and 3.42s and 4.2s, respectively, in severe COPD (almost fivefold total increase in RCEXP). In contrast, they found milder increases in RCEXP among moderate COPD subjects, wherein values of τ increased from an initial value of 0.79s in the early compartment to 1.05, 1.25, and 1.47s, respectively, in the compartments towards the end of exhalation (almost twofold total increase in RCEXP).
Thus, an abrupt rise in RCEXP in severe COPD occurring once expired volume reached the 75% (incomplete) threshold at ZEEP signifies marked deterioration of peripheral airway conductance and the need for PEEP to support expiration. PEEP also would be indicated in moderate COPD, although it is reasonable to predict the impact on pulmonary mechanics and/or gas exchange would likely be less pronounced.
Finally, the most salient clinical finding was that 3τ measured at V’/V 75% (incomplete expiration) approximated the actual time for complete exhalation within 0.4 ± 2.4s. It was also used to assess the severity of COPD [22]. This reflects that in COPD patients, airway resistance becomes the major limitation to exhaled flow.
Characteristics of RCEXP across volume compartments in ARDSGuttmann et al. were the first to study RCEXP in ARDS using the V’/V method. They reported a τ of 0.69 ± 0.22s whose values differed marginally across expired volume compartments [6] The explanation of this finding was discovered when investigators analyzed total airway resistance into its imposed and respiratory system subcomponents. In ARDS, the resistive characteristics of the lung and chest wall contributions accounted for up to 50% of RCEXP. Although it may seem that RCEXP was within the normal range (i.e., 0.69s), it must be stressed that the mean VT used was 989 ml, which confirms that VT is one of the major determinants of RCEXP. This is also confirmed by other studies in ARDS patients who reported recruitable lungs, higher VT, and normal or even prolonged RCEXP [15, 26].
Kondili et al. [31] studied the effects of PEEP on RCEXP and they also examined the effects of imposed mechanical resistance. Their RCEXP data was presented as both total its respiratory system subcomponent (RCEXP–RS). Across all volume compartments, the mean values of τ for total RCEXP exceeded those of RCEXP–RS: τ of 0.82s vs. 0.61s (ZEEP), 0.77s vs. 0.52s (PEEP of 5 cmH2O), 0.74s vs.0.57s (PEEP of 10 cmH2O) and 0.68s vs. 0.55s (PEEP of 15 cmH2O). Thus, the lungs and chest wall accounted for 52 to 61% of total RCEXP and were somewhat higher than those reported by Guttman and colleagues.
The effects of PEEP on total RCEXP and RCEXP–RS were more complex and informative when assessed by its impact on fast and slow lung compartments. In contrast to the inconsistent relationship between total RCEXP and estimated RCEXP–RS that were observed among COPD subjects in response to PEEP, the τ-compartment patterns found in ARDS mirrored one another despite their marked separation in values of τ [31]. Consistent with the findings of Guttmann and colleagues [6], PEEP largely homogenized values of τ across compartments (Fig. 2B). This contrasted with total RCEXP and RCEXP–RS under ZEEP conditions, wherein fast vs. show compartments were salient (albeit not as stark as that found with ZEEP in their COPD subjects).
Chelucci et al. [17] used respiratory inductive plethysmography to measure thoracic volume rather than gas volume during tidal ventilation. They observed distinct fast and slow lung compartments, wherein RCEXP of the slow compartment was 11–13-fold longer than the fast compartment, irrespective of VT size (10 vs. 5 mL/kg) and PEEP (13 cmH2O) vs. ZEEP. In the presence of PEEP, the fast compartment had mean τ values 16% greater at 10 vs. 5 mL/kg (0.58 vs. 0.50s, respectively), whereas corresponding slow compartment τ values were unchanged (6.44 vs. 6.46s, respectively). Removal of PEEP resulted in marked reductions in RCEXP in both the fast (40% decrease from τ of 0.58 to 0.35s) and slow (27% decrease from τ of 6.44 to 4.67s) compartments. The impact of PEEP on RCEXP in ARDS suggests it counters the compressive hydrostatic or elastic forces acting upon open lung units with negligible peripheral obstruction. Without additional information (i.e., volumetric capnography phase characteristics), the interpretation of slow compartment changes RCEXP remains problematic.
Generalizing the characteristics of RCEXP in ARDS, and particularly the impact of PEEP, should be done with caution. It should consider that ARDS evolves through overlapping phases of acute lung injury that alter both lung morphology and mechanics, as well as the impact of age (i.e., age-related increases in closing volume) as well as alterations in the chest wall components (i.e., both the
Comments (0)