
Remember me





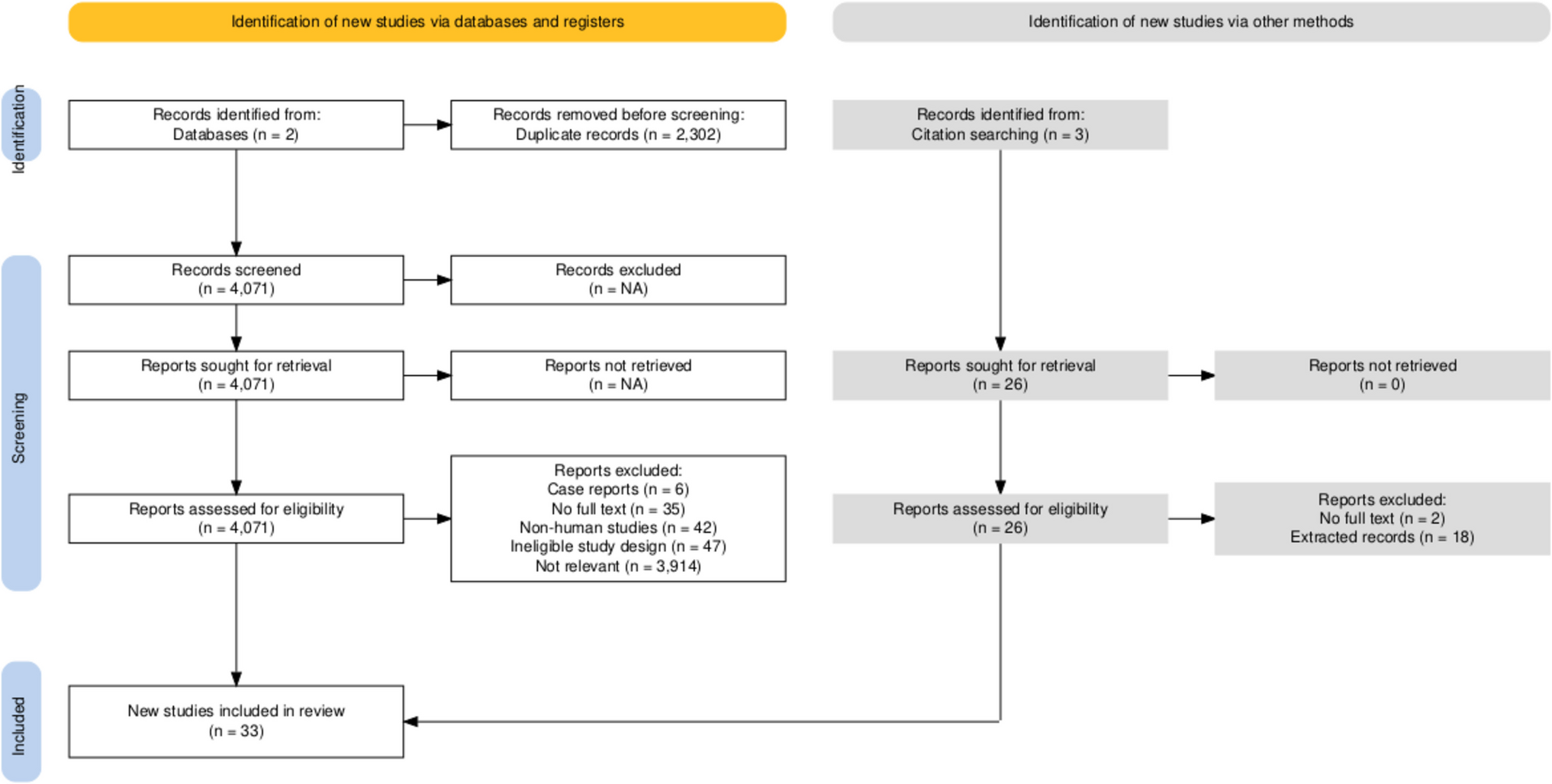
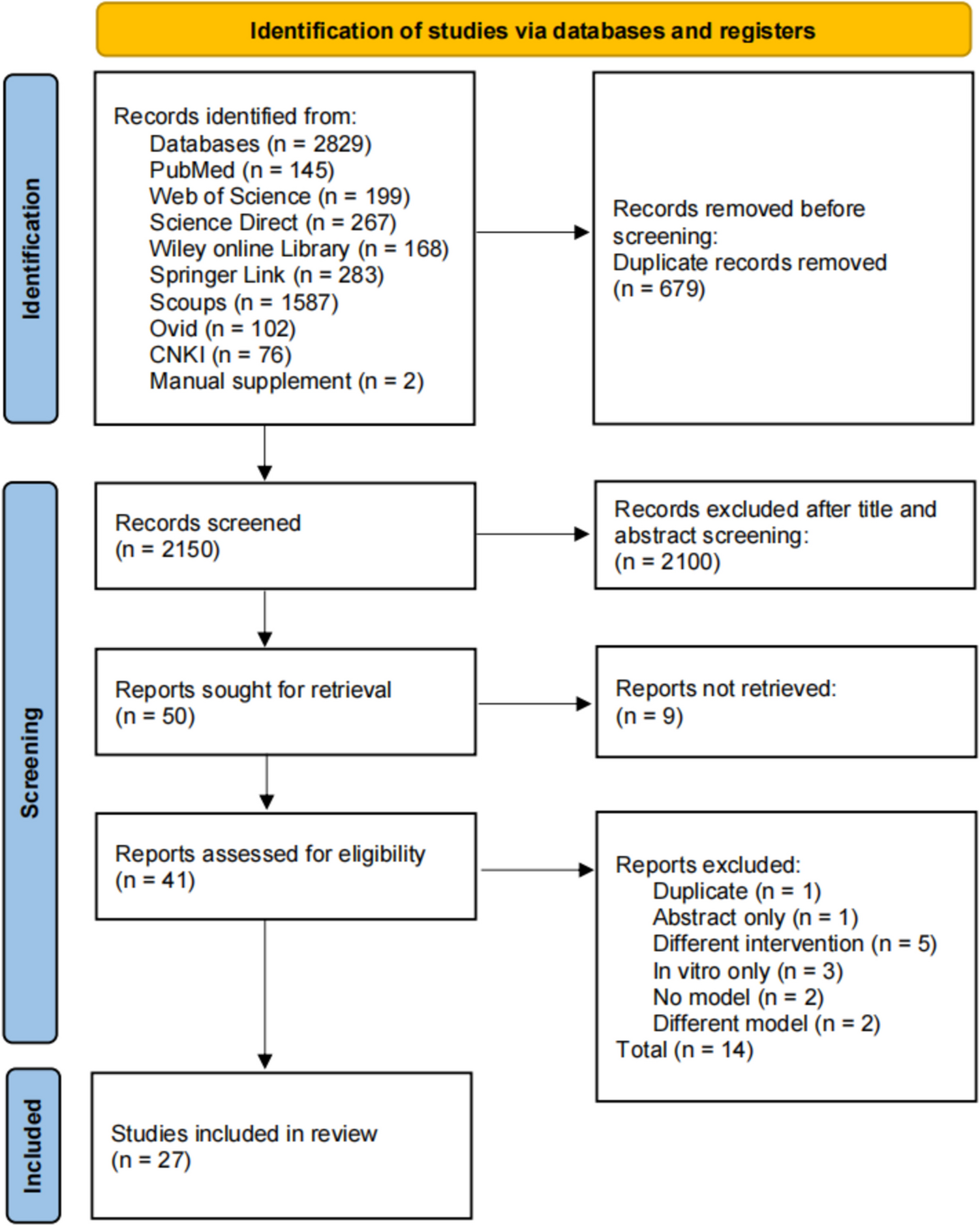
The literature search yielded 6373 results, and 2302 duplicates were removed, leaving 4071 records for title and abstract screening. Reports were excluded due to being irrelevant (n = 3914), no full text (n = 35), non-human studies (n = 42), ineligible study design (n = 47) and case reports (n = 6). Additional hand searching found another six eligible articles. Overall, 33 studies [11, 15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46] were included in the qualitative analysis (Fig. 1).
Fig. 1 Included studies
Included studiesThere were no restrictions to the population and we collected data on studies that included any patients (general population/community dwelling older adults) (n = 29), patients with osteoporosis (n = 6), patients on haemodialysis (n = 8), patients on post-menopausal (n = 8), patients with aortic stenosis (n = 4), patients with type 2 DM (n = 2), patients with CKD (n = 2), patients at high risk for atherosclerotic aortic plaques (n = 1), patients on bisphosphonate therapy (n = 1), patients with pseudoxanthoma elasticum (n = 2), patients with secondary hyperparathyroidism (n = 2) and patients with AMI (n = 1). Twelve studies used alendronate, eight studies used etidronate, eight studies used denosumab, three studies used ibandronate, three studies used zoledronate, two studies used risedronate, one study used calcitonin and one study used teriparatide (Table 1).
Table 1 Literature summaryTen studies were conducted in the United States of America (USA), seven in Japan, two in Australia, two in Netherlands, two in Spain, one in Denmark, one in Italy, two in Taiwan, one in Iran, two in the UK and one in Turkey. The smallest study included 12 patients [19] and the largest study included 141,202 patients [35]. Follow-up time varied between a minimum of 1 month and a maximum of 3.9 years (Table 2).
Table 2 Study demographicsLiterature qualityCohort studies were rated as good/good (n = 9), good/fair (n = 3), fair/fair (n = 5) or fair/poor (n = 1) quality by both reviewers (Supplementary Table 2). A case control study included was rated as good by both reviewers (n = 1) (Supplementary Table 3). RCTs were rated as low/low (n = 2), low/low-unclear (n = 5), low-unclear/low-unclear (n = 2) and low/high (n = 4) risk of bias by both reviewers (Supplementary Table 4). There was some publication bias as visualised in the funnel plots (Supplementary Figs. 1–6).
Background of skeletal riskTable 3 provides a summary of patient characteristics in terms of their background skeletal risk (baseline vertebral BMD (n = 6), lumbar spine BMD (n = 9), femoral neck BMD (n = 9), previous vertebral fracture (n = 2), vitamin D intake (n = 8), calcium intake (n = 11) and phosphate binder intake (n = 5)).
Table 3 Background of skeletal riskBackground of cardiovascular riskTable 4 provides a summary of patient characteristics in terms of their cardiovascular risk (DM (n = 19), HTN (n = 12), hyperlipidaemia (n = 5), HF (n = 2), CKD (n = 10), osteoporosis (n = 9), previous MI (n = 2), previous stroke or TIA (n = 3)).
Table 4 Background of cardiovascular riskOutcomes of interestData were collected from 33 studies. Seven studies reported CAC; eight studies reported AAC; one study reported common carotid artery calcification; two studies reported mitral annulus calcification; one study reported iliac arteries calcification; one study reported lower limb arterial calcification; one study reported femoral artery calcification; one study reported total arterial calcification; nineteen reported aortic calcification (any site); five studies reported aortic valve area (AVA) (Table 2). Three studies reported ejection fraction (EF). EF is not strictly a marker of vascular/valvular calcification; we reasoned that EF would be influenced by valvular and vascular calcification and is included as an exploratory, hypothesis generating endpoint. Of interest, six studies reported on carotid intima-media thickness (IMT), but, as this represents atherosclerotic plaque not necessarily calcified, we chose to not analyse these data. Furthermore, as there was not a specific search term for IMT, we also cannot be certain that we have captured all literature reporting on osteoporosis medications and IMT.
Major findings from the included studies are described in Table 2. Etidronate resulted in less progression in coronary artery, femoral artery, thoracic and abdominal aortic calcification in seven studies [17, 19, 26, 29, 34, 41, 43]. Alendronate resulted in less progression in AAC and aortic stenosis in two studies [11, 28], and no difference in progression of CAC, aortic calcification and aortic stenosis in five studies [15, 16, 24, 30, 37]. Ibandronate resulted in no difference in AAC progression in one study [18]. Risedronate resulted in less progression in AAC and vascular calcification in two studies [23, 42]. Denosumab resulted in less progression in CAC and AAC in three studies [32, 35, 46], and no difference in AAC, aortic stenosis and CAC progression in three studies [15, 27, 37]. Zoledronate resulted in no difference in AAC progression in one study [33].
Meta-analysisFifteen studies, including a total of 2344 patients, had data available for meta-analysis (Fig. 2A–E). Specifically, studies that reported aortic calcification (any site) were not able to be analysed as varying units of measurements were used, for example, reporting on a percentage of the cohort that experience regression/progression of calcification as opposed to some measure of change in calcification. Therefore, we focused our analysis on outcomes for which units of measurable change were reported for a more targeted and clinically relevant analysis. Other studies not included were due to a lack of control group or specific results that were required for analysis. Parameters like mitral annular calcification and pulse wave velocity were unable to be analysed due to a lack of sufficient data.
Fig. 2


A Forest plot of standardised mean difference for change in abdominal aortic calcification (AAC) and coronary artery calcification (volume) (CAC-volume). B Forest plot of standardised mean difference for change in abdominal aortic calcification (AAC) and coronary artery calcification (volume) (CAC-volume) in patients on etidronate. C Forest plot of standardised mean difference for change in abdominal aortic calcification (AAC) and coronary artery calcification (volume) (CAC-volume) in patients on haemodialysis. D Forest plot of standardised mean difference for change in coronary artery calcification (Hu) (Geers et al. (denosumab users)) and coronary artery calcification (Hu) (Geers et al. (alendronate users)). E Forest plot of standardised mean difference for change in aortic valve area/aortic stenosis (AVA-AS) and change in ejection fraction (EF)
Abdominal aorta calcificationSix studies, including 1815 patients, reported on change in AAC as an outcome of anti-resorptive therapy [23, 27, 28, 34, 36, 41]. Suzuki included patients on haemodialysis and treated them with denosumab; Hashiba included patients on haemodialysis and treated them with etidronate; Bartstra included patients with pseudoxanthoma elasticum and treated them with etidronate; Okamoto included patients with kidney transplant and treated them with denosumab; Samelson included post-menopausal and osteoporotic patients and treated them with denosumab as a secondary analysis of a larger fracture reduction trial; Kanazawa included patients who were post-menopausal, were osteoporotic and had type 2 diabetes mellitus. When pooled together, the rates of AAC progression were similar (SMD = − 0.45 [95% confidence interval − 0.99 to 0.08, tau2 = 0.33; n = 935; I2 = 84%; Fig. 2A]), where SMD represents the difference in the change in vascular outcome (AAC) between treatment and control groups. Focusing specifically on patients on etidronate, four studies with a total of 1721 patients studied the effects of etidronate on change in AAC [23, 27, 28, 36]. When pooled together, the rates of AAC progression were similar (SMD = − 0.41 [95% confidence interval − 1.24 to 0.41, tau2 = 0.58, n = 889; I2 = 89%; Fig. 2B]). Focusing specifically on haemodialysis patients, four studies with a total of 1736 patients, studied the effects of haemodialysis on change in AAC [23, 27, 28, 34]. When pooled together, the rates of AAC progression were similar (SMD = − 0.08 [95% confidence interval 0.31 to 0.16, tau2 = 0.019, n = 898; I2 = 2%; Fig. 2C]).
Coronary artery calcification (volume)Four studies, including 239 patients, reported on change in volume of CAC (CAC-volume) as an outcome of anti-resorptive therapy [16, 19, 32, 34]. Chen included patients who were on haemodialysis and had secondary hyperparathyroidism and treated them with denosumab; Hill included osteoporotic patients and treated them with alendronate; Ariyoshi included patients on haemodialysis and treated them with etidronate; Bartstra included patients with pseudoxanthoma elasticum and treated them with etidronate. When pooled together, the rates of CAC-volume progression were similar (SMD = − 1.19 [95% confidence interval − 2.92 to 0.55, tau2 = 2.96; n = 120; I2 = 91%; Fig. 2A]), where SMD represents the difference in the change in vascular outcome (CAC-volume) between treatment and control groups. Focusing specifically on patients on etidronate, two studies with a total of 154 patients studied the effects of etidronate on change in CAC (CAC-volume) [16, 32]. When pooled together, the rates of CAC-volume progression were similar (SMD = − 2.34 [95% confidence interval − 5.26 to 0.58, tau2 = 4.27, n = 77; I2 = 96%; Fig. 2B]). Focusing specifically on haemodialysis patients, four studies with a total of 185 patients studied the effects of haemodialysis on change in CAC (CAC-volume) [16, 34]. When pooled together, the rates of CAC-volume progression were similar (SMD = − 0.46 [95% confidence interval − 1.33 to 0.42, tau2 = 0.0.35, n = 93; I2 = 88%; Fig. 2C]).
Coronary artery calcification (Hu)Three studies, including 218 patients, reported on change in volume of CAC (CAC-Hu) as an outcome of anti-resorptive therapy [15, 16, 46]. Chen included patients who were on haemodialysis and had secondary hyperparathyroidism and treated them with denosumab; Hill included osteoporotic patients and treated them with alendronate; Geers included patients with aortic stenosis and treated them with either denosumab or alendronate. When pooled together, the rates of CAC-Hu progression were similar (when including those treated with denosumab in Geers et al.) (SMD = − 0.28 [95% confidence interval − 2.09 to 1.53, tau2 = 2.48; n = 112; I2 = 97%; Fig. 2D]) and CAC-Hu (when including those treated with alendronate in Geers et al.) (SMD = − 0.67 [95% confidence interval − 1.72 to 0.38, tau2 = 0.784; n = 104; I2 = 94%; Fig. 2D]), where SMD represents the difference in the change in vascular outcome (CAC-Hu) between treatment and control groups.
Aortic valve area (aortic stenosis)Four studies, including 353 patients, reported on change in aortic valve area or aortic stenosis (AVA-AS) as an outcome of anti-resorptive therapy [11, 20, 21, 37]. Skolnick had no specific exclusion criteria for the population and treated the patients with bisphosphonates, calcitonin or selective oestrogen receptor modulators; Pawade included patients with aortic stenosis and treated them with denosumab or alendronate, but helpfully provided data for ‘any antiresorptive use’; Alishiri included patients with aortic stenosis and osteoporosis and treated them with alendronate; Innasimuthu included patients with aortic stenosis and treated them with alendronate or risedronate. When pooled together, there was a significant small increase in AVA-AS (SMD = 0.56 [95% confidence interval 0.07 to 1.06, tau2 = 0.18; n = 165; I2 = 76%; Fig. 2E]), where SMD represents the difference in the change in vascular outcome (AVA-AS) between treatment and control groups. This means that the rate of progression in stenosis was marginally slower in those on anti-resorptives.
Ejection fractionThree studies, including 201 patients, reported on percentage change in EF as an outcome of anti-resorptive therapy [11, 20, 21]. Skolnick had no specific exclusion criteria for the population and treated the patients with bisphosphonates, calcitonin or selective oestrogen receptor modulators; Innasimuthu included patients with aortic stenosis and treated them with alendronate or risedronate; Alishiri included patients with aortic stenosis and osteoporosis and treated them with alendronate. When pooled together, there was no increase in EF (SMD = 0.26 [95% confidence interval − 0.14 to 0.66, tau2 = 0.038; n = 63; I2 = 62%; Fig. 2E]).
Sensitivity analysisTo account for clinical heterogeneity (e.g. study populations and interventions trialled), a leave-one-out sensitivity analysis was conducted for the above outcomes (Supplementary Table 5). Exclusion of Samelson only resulted in an overall significant reduction in AAC. Exclusion of any study except Hill resulted in an overall significant reduction in CAC-volume. Exclusion of any study except Hill resulted in an overall significant reduction in CAC-Hu (Geers et al. (denosumab users) and Geers et al. (alendronate users)) and overall significant increase in AVA-AS. Exclusion of Skolnick only resulted in an overall significant increase in EF.
Comments (0)