Stroke, a devastating condition, results in high mortality and significant, long-term disability, and represents a growing global health burden [1,2,3]. An interdisciplinary team-based approach, led and coordinated by nursing professionals, plays an important role in optimizing acute stroke treatment, preventing patient deterioration, and enhancing rehabilitation potential and outcomes [4,5,6]. When stroke patients are admitted, a stroke activation protocol initiates immediate organized medical investigations and should also, by default, set in motion standardized nursing care pathways to ascertain implementation of important clinical bedside observations and interventions [7,8,9].
This review critically examines key considerations in translating evidence-based care and acute stroke surveillance into interdisciplinary practice, with a focus on nursing in smaller stroke units embedded in general neurological settings. It initially provides a broad introduction to the role of nurses in acute stroke care, gives an overview of the usability of care bundles to optimize bedside care, and finally presents a case study illustrating how acute stroke care can be adapted to maintain high standards when nested within general neurology settings. Additionally, in light of current evidence, we reflect on elements to enhance interdisciplinary support during implementation to ensure consistent, or even rising, standards of care.
Nurses’ Role in Acute Stroke Care
The role of nurses in stroke care is well-established, and their prominence within the stroke team is expected to grow with the increasing complexity of treatments and the emergence of new therapies [10]. Stroke guidelines consistently emphasize that standardized nursing activities improve care across all stroke types, facilitate early detection of complications, and ultimately enhance patient outcomes [7, 8, 11,12,13,14]. Nurses provide a holistic perspective, taking on essential roles such as care coordinators, ensuring continuity and supporting patients and families [9, 15, 16]. Moreover, their responsibilities at the bedside include delivering effective fundamental care, preventing complications, facilitating early rehabilitation, and, throughout the patient’s stroke unit stay, applying systematic, multicomponent monitoring to identify and respond swiftly to clinical deterioration [10, 16,17,18].
Care Pathways and Unique Contributions of Acute Stroke Nursing
Care pathways, such as those developed to ensure timely delivery of thrombolysis and thrombectomy for ischemic stroke and rapid blood pressure management for acute hemorrhagic stroke, are key to achieving successful outcomes and are now standard practice [4, 19, 20]. Regardless of eligibility for reperfusion therapy, comprehensive nursing care remains vital [10, 21, 22]. However, many guidelines fail to address the specifics of what nursing care exactly entails, such as the frequency and content of neuro checks, methods of assessing different stroke types, and best systems for auditing and feedback [23, 24]. Furthermore, there is limited guidance on aligning and integrating nursing priorities within interdisciplinary activities, leaving significant gaps for the practical applicability of standardized nursing protocols [10, 25, 26].
Acute stroke nursing distinguishes itself from medical interventions through its broad applicability. It can be provided in virtually any hospital setting for any stroke patient, including those who are elderly, have severe strokes, or face multiple comorbidities [18, 27,28,29]. In contrast, medical interventions such as reperfusion therapies, though highly effective, are often limited by strict eligibility criteria [30, 31].
Stroke Units – Need to Maximize Local Use of Evidence-Based Guidelines
Stroke units, equipped with non-invasive monitoring and emphasizing an interdisciplinary approach to bedside care, have demonstrated remarkable, consistent effectiveness in improving patient outcomes over the past 25 years [32, 33]. The most recent landmark meta-analysis revealed that stroke unit care reduces mortality by saving two additional lives per 100 patients treated compared to general medical wards. Additionally, six more patients return home instead of being transferred to a nursing facility, and a further six achieve independent living [27]. The size and structure of stroke services within a hospital are shaped by factors such as population density and available resources [34, 35]. Notably, even smaller stroke units, managing as few as 100 admissions annually, have demonstrated significant benefits of stroke unit care [35].
To fully leverage the benefits of stroke unit care, it is necessary to implement locally adapted guidelines to ensure coordinated care that prioritizes safety and minimizes complications [24, 36, 37]. However, recommendations often overlook the resources required for implementation [19]. Comprehensive education and training of stroke nurses empowers evidence-based decision-making and high-quality care, but educational strategies often remain inconsistent [38,39,40,41]. Along these lines, a recent review underscores the importance of organizational support in developing effective knowledge enhancement solutions [6].
Care Bundles – From Knowledge to Bedside Use
Effectively translating and integrating new stroke care approaches into clinical practice calls for strong communication within the interdisciplinary team [21, 41]. Denny et al. [42] recently outlined strategies to foster alignment toward interdisciplinary shared goals. Key strategies include equipping hospital staff with the knowledge and resources to follow guidelines, engaging them in the implementation process, and resolving specific patient care challenges proactively. Feasible guideline adaptations are crucial, as overly ambitious objectives can hinder compliance [43].
Integrating clinical recommendations into care bundles promotes their clinical adoption and creates a direct link between evidence and clinical practice [38, 44, 45]. In recent years, care bundles have gained momentum, often replacing comprehensive guidelines due to their practicality and capacity to enhance interdisciplinary collaboration [46, 47]. Care bundles consist of succinct, evidence-based sets of interventions tailored to specific patient populations and care settings. They typically consist of three to five components. When implemented as a cohesive set, these interventions yield better outcomes than they do when applied individually [48]. Notably, care bundles have proved effective in stroke management and even in settings that deviate from traditional stroke unit structures, further highlighting their practicality and versatility [26, 47, 49,50,51,52].
Designing effective stroke care bundles involves a diverse range of healthcare professionals, including nursing staff, stroke physicians, dietitians, speech-language therapists, physiotherapists, and occupational therapists [23, 53]. These professionals must collaborate in composing care bundles and ascertain sufficient flexibility to address the unique needs of patients [54]. Other key factors influencing the design include the availability of technology and equipment for surveillance, the physical layout of the stroke unit, staff training and competency levels, and the alignment with existing care pathways [23, 24, 55,56,57]. Effective communication among healthcare providers cultivates a collaborative, multicomponent approach that prioritizes accurate documentation. By connecting evaluation systems to provide feedback on care bundle fidelity, teams can enhance the consistency and long-term sustainability of quality care provision [5, 24].
Acute Stroke Nursing Care Bundles – Description of Setting, Development, and Critical ReflectionsSetting – a Small Stroke Unit Nested Within a General Neurological Department
Landspítali, the National University Hospital (LUH) in Reykjavik, serves as Iceland’s leading stroke center. It offers thrombolysis and is the sole facility in the country capable of performing mechanical thrombectomy. The hospital primarily serves Reykjavik and surrounding area, with a catchment population of 239,000 in 2022, or approximately 65% of the country’s total population. Moreover, LUH also receives patients requiring advanced stroke treatment from across Iceland, with a total population of 376,000 in 2022 (www.statice.is).
In 2022, LUH had 408 stroke admissions, comprising 337 ischemic and 71 hemorrhagic cases [58]. For decades, LUH has functioned as Iceland’s centralized hub for stroke care, streamlining treatment pathways and promoting standardized practices nationwide. Approximately 82% of all stroke patients in Iceland are admitted to LUH, either as the first hospital of arrival or by secondary referral from other hospitals in the Icelandic stroke network. Advanced stroke services are available according to definitions of Mead et al. [19] in the form of interdisciplinary stroke expertise, access to advanced imaging, and comprehensive therapies.
A surveillance room with a capacity of four patients was established within an acute 22-bed neurological department. This dedicated stroke area provides non-invasive cardiac monitoring at each bed (without arterial lines) where beds are separated by curtains to maintain patient privacy. The staffing model features a nurse-to-patient ratio of 1:4, complemented by a specially trained licensed practical nurse (LPN) on every shift, resulting in an overall nursing staff ratio of 1:2. In Iceland, LPNs complete a three-year vocational education program. To qualify to work in the acute stroke unit they must pass the National Institute of Health Stroke Scale (NIHSS) training module and alongside nurses, participate in annual “stroke courses” and clinical case discussions to maintain their competencies. The staffing level aligns closely with the European Stroke Organization’s recommendations, which advocate for an optimal nurse-to-patient ratio of 1:2 in acute stroke care [59]. Patients initially admitted to the stroke unit can transition to step-down stroke care in the adjacent neurological unit, where nurse-to-patient ratios range from 1:4 to 1:6, plus LPNs, apart from during the night shifts when the ratio is lower.
Nursing education in Iceland maintains high standards, requiring a bachelor’s degree after four years of university-level training. Collaboration between the Faculty of Nursing and clinical specialties ensures updates, like advancements in stroke care, are swiftly integrated into the curriculum. Third-year students receive current lectures, equipping about 200 graduates annually with updated stroke care knowledge. Teaching is led by clinical nurse specialists and academic chairs, who also oversee hospital education programs. This ensures bidirectional integration of academic and clinical training.
Despite this structure, significant challenges persist in delivering specialized stroke care. Key issues include staffing shortages, high nurse turnover rates, the lack of dedicated clinical specialization programs, and difficulties in care documentation and auditing. Since the stroke unit is integrated within broader neurology, nursing staff do not work exclusively with stroke patients, making it challenging to maintain clinical stroke competency.
Developing Care Bundles: Bridging Knowledge and Practice
In preparation for the launch of the dedicated stroke unit within our neurological department, we organized a collaborative forum inviting input from key stakeholders from the local stroke team. This interdisciplinary group included representatives from dietetics, neurology, nursing, occupational therapy, physiotherapy, and speech-language therapy. Each participant provided valuable insights, helping to identify priorities for developing effective nursing care bundles. A core team of nurses and physicians worked together to reach consensus on critical issues, ensuring clarity and creating a strategy to enhance adherence to the care bundle elements. Intended as both clinical tools and educational resources, the care bundles encompass elements to enhance nurse-neurologist collaboration.
Using Borgerts et al.‘s [60] method, we systematically reviewed guidelines and up-to-date evidence to identify key elements for the care bundles. A structured, two-tiered approach was implemented for staff involvement. The first tier engaged key stakeholders within the stroke nursing team, including the head nurse of the neurological department, clinical nurse specialists, clinical staff nurses serving as opinion leaders, and the academic chair in neurological nursing. The second tier involved gathering feedback and fostering discussion with the broader interdisciplinary stroke team. This collaborative effort ensured smooth integration into the interdisciplinary pathway.
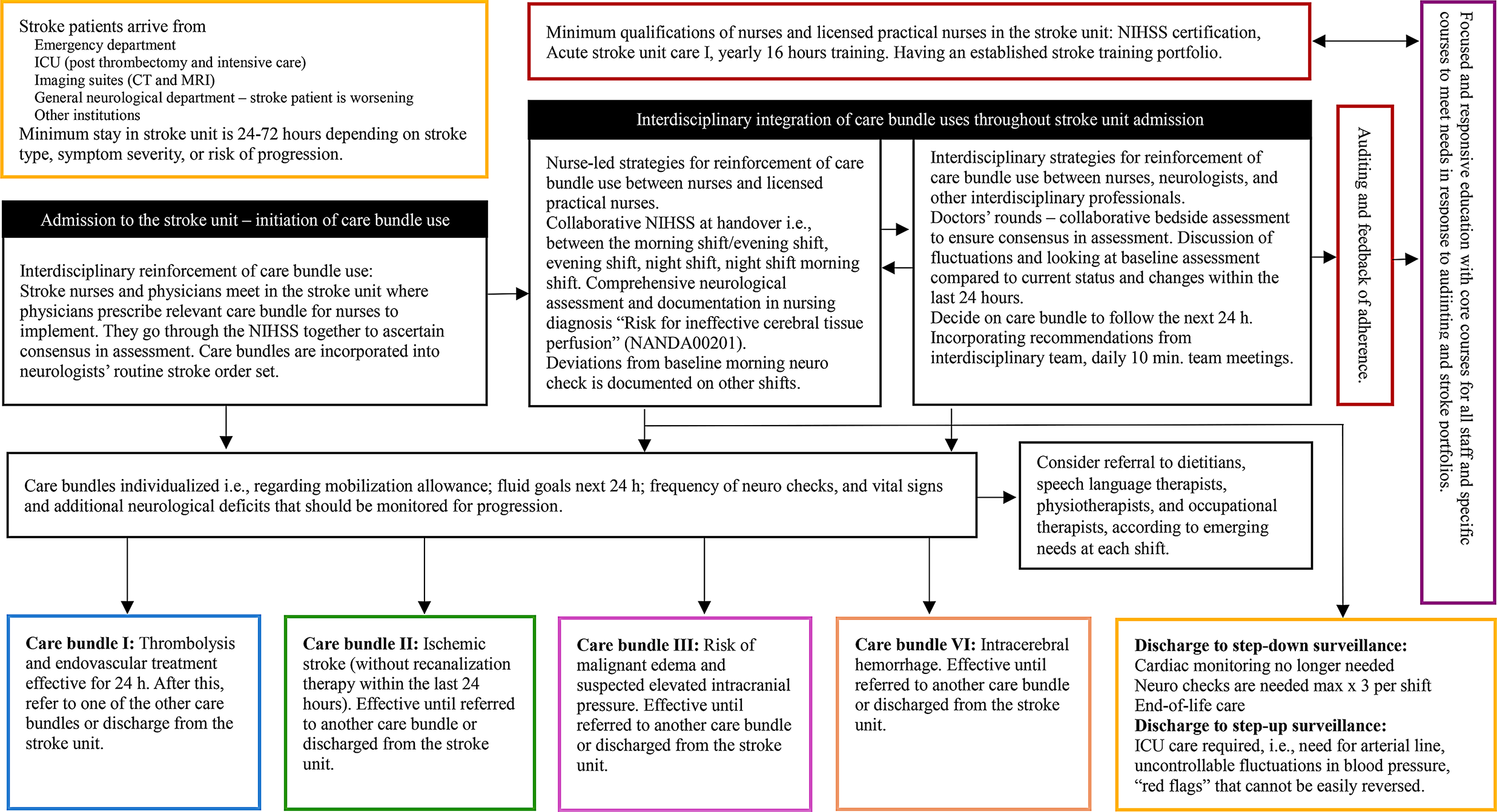
We identified a need for four distinct care bundles that, while sharing many common care components, differed in important aspects; see Table 1. These pathways included: (1) thrombolysis and endovascular treatment, (2) ischemic stroke (without recanalization therapy within the last 24 h), (3) risk of malignant edema and suspected elevated intracranial pressure, and (4) intracerebral hemorrhage. Each care bundle comprised four to five essential components, with overlapping elements across all pathways. Common components included position and mobility, fever, sugar, swallowing (FeSS), nutritional intake, neurostatus, and vital signs. Additionally, the thrombolysis and endovascular treatment bundle emphasized a critical focus on bleeding risk management. To ensure a prompt response to patient deterioration, we identified critical red flags necessitating immediate notification of the stroke physician.
Table 1 Care bundles for acute stroke nursing surveillanceKey measures for preventing complications align with established guidelines, focusing on the timely recognition and management of issues such as neurological deterioration, immobility-related problems, swallowing and nutritional challenges, signs of increased intracranial pressure, cerebral edema, fever, hyperglycemia, pneumonia, and other infections [11, 26, 61]. Beyond these standard measures, we identified issues in nursing care that required targeted attention and optimization. These included blood pressure fluctuations in hemorrhagic stroke, ensuring proper oral hygiene, and supporting paralyzed arms – all these issues are evidence-based but often considered “common sense” and thus not explicitly stated in local guidelines. To enhance care delivery, we introduced clear documentation guidelines and developed user-friendly nursing diagnoses tailored to the unique needs of the stroke unit. Additionally, the care bundles were designed to enable integration of the rapidly evolving evidence in stroke research while also being responsiv






Comments (0)