Pathophysiology of Acne
Acne vulgaris is a multifactorial disorder, involving both genetic and environmental factors, affecting the pilosebaceous unit [4]. It has been related to the interplay among follicular hyperkeratinization, sebaceous gland dysfunction, hyperproliferation of Cutibacterium acnes, and inflammation, further exacerbated by oxidative stress, and modulated by several factors including hormones and metabolic alterations [4]. Hormonal imbalances associated with acne lead to increased androgen levels, which, in turn, increase sebum production and promote keratinocyte proliferation [18]. This proliferation, together with abnormal differentiation of follicular epithelial cells observed in patients with acne, leads to follicular hyperkeratinization [18].
Additionally, lipid oxidation, particularly of squalene, generates lipoperoxides that trigger inflammatory cascade responses [19]. Sebum oxidation also creates a microaerophilic environment supporting Cutibacterium acnes growth, contributing to microbiota dysregulation. In turn, bacteria activate toll-like receptors on sebocytes and keratinocytes, leading to pro-inflammatory IL- 6, IL- 8, and IL- 12 release and produce porphyrins, inducing reactive oxygen species (ROS) production [20]. This leads to neutrophil recruitment and aggregation, resulting in additional release of ROS and perpetuating inflammation in a self-reinforcing cycle. Lipid peroxidation products also contribute to further disruption of follicular homeostasis [19].
Metabolic factors, including insulin resistance and hyperinsulinemia, further exacerbate acne by stimulating sebocyte hyperactivity and androgen synthesis, linking acne to obesity and metabolic syndrome (MetS) [21,22,23]. Dyslipidemia also amplifies oxidative stress and inflammation, reinforcing the acne-obesity-MetS axis [21,22,23].
Take Home Message
Acne vulgaris is driven by follicular hyperkeratinization and sebaceous gland dysfunction, with lipid oxidation and skin microbiota dysregulation contributing to impaired follicular homeostasis, inflammation and oxidative stress. Metabolic alterations, such as obesity, further exacerbate these pathogenetic processes through hormonal imbalances, insulin resistance, and dyslipidemia, amplifying inflammation and oxidative stress.
The Role of Hormones in Acne
It is well established that endocrine mechanisms play a pivotal role in the etiopathogenesis of acne [24]. Several different hormones and growth factors, including androgens, estrogens, glucocorticoids, insulin, IGF- 1, fibroblast growth factors, and epidermal growth factors, are involved in the pathogenesis and the progression of acne, through their binding with high-affinity receptors [24]. Androgens, mainly testosterone and its active metabolite 5α-dihydrotestosterone (5α-DHT) that is converted via 5α-reductase type 1, an enzyme expressed mainly in facial sebocytes and sweat glands, represent the most significant endogenous contributors to the development and maintenance of acne [25]. Indeed, androgen levels correlate with acne severity, and many endocrinopathies characterized by hyperandrogenism, such as polycystic ovary syndrome, late congenital adrenal hyperplasia, and ovarian, adrenal, or pituitary tumours, are associated with acne [25]. However, current experimental research on the pathophysiology of acne is depicting a more complicated background. In particular, the environmental exposures to endocrine disrupting chemicals have proved to alter the androgen receptor-mediated signal transduction within the pilosebaceous unit [26]. In addition, IGF- 1, acting via the AKT/mTORC1/SREBP1 signalling pathway, not only primarily results in an overproduction of sebum, abnormal keratinization of follicles, and perifollicular inflammation, but it increases also the conversion of testosterone to 5α-DHT. Moreover, sebocytes per se can also synthesize androgens in situ, and the interaction of local active androgen production with circulating IGF- 1 exerts worsens the effects on the pilosebaceous unit [26].
Take Home Message
Endocrine mechanisms play a crucial role in the pathophysiology of inflammatory dermatological conditions, with androgens, IGF- 1, and environmental endocrine disruptors contributing to sebaceous gland activity, inflammation, and disease progression. The interplay between systemic hormones and local androgen synthesis further exacerbates these effects, highlighting the complexity of hormonal regulation in skin health.
Acne and Obesity
The link between acne and obesity is complex and multifaceted, as highlighted by various studies exploring their association [27]. Acne vulgaris, the most common skin disorder in the Western world, affects teens and young adults [28]. One potential connection between obesity, MetS and acne is represented by the role of adipokine-driven inflammatory cytokines, which contribute to systemic inflammation and may exacerbate acne [29]. The rising prevalence of obesity among adolescents raised interest in understanding the interplay between these conditions, yet findings from different studies remain inconsistent [30]. For instance, a population-based retrospective cohort study on 643 preadolescents and age- and sex-matched controls found a positive correlation between higher body mass index (BMI) and acne risk [31]. Preadolescents with acne had a higher median BMI percentile compared to controls (75.0 vs. 65.0, respectively), with 16.7% of patients with acne suffering from obesity. Additionally, increasing BMI was associated with a higher likelihood of receiving systemic acne treatment, suggesting a relationship between obesity, acne severity, and therapeutic needs [31]. Conversely, a nationwide cross-sectional study in Israel, which included 600.404 adolescents, found an inverse association between BMI and acne [23]. The prevalence of acne decreased progressively from underweight to obesity. Participants with a severe obesity exhibited the lowest odds of acne (adjusted odds ratio [aOR]: 0.53 for males and 0.50 for females), indicating a potential protective effect of higher BMI in this cohort [23].
Further evidence points to a link between obesity, body composition, and acne severity [32]. A prospective case–control study involving 320 individuals revealed that patients with acne vulgaris had significantly higher BMI, body fat percentage, and fat mass compared to healthy controls. Notably, these parameters were particularly elevated in patients with moderate to severe acne. Female patients demonstrated higher body fat percentages, while male patients showed increased fat-free body mass and total body water. These findings suggest that body composition metrics may predict acne severity and could help identify patients at risk of metabolic complications [32].
Take Home Message
While obesity and acne are frequently associated, the relationship appears to vary by populations, age, and sex. Some studies suggest that higher BMI increases the risk and severity of acne, while others indicate a protective effect. These discrepancies highlight the need for further research to clarify the underlying mechanisms.
Acne and Cardiovascular Risk
Acne vulgaris, traditionally viewed as a localized dermatological condition, is now recognized for its potential systemic implications, including an association with increased cardiovascular risk [33, 34]. This chronic inflammatory skin disorder affects approximately 85% of adolescents and a substantial proportion of adults, with emerging evidence linking it to metabolic dysregulation and cardiovascular comorbidities such as hypertension, dyslipidemia, insulin resistance, and MetS [33, 34].
Acne pathogenesis involves the dysregulation of innate and adaptive immune responses, with increased levels of pro-inflammatory cytokines such as TNF-α, IL- 17 [35]. These inflammatory mediators are also key players in the development of atherosclerosis, endothelial dysfunction, and insulin resistance-critical pathways in cardiovascular diseases (CVDs) [36].
The IGF- 1 and the mTORC1 signaling pathways, which are implicated in acne development, also contribute to metabolic and cardiovascular disorders [37]. IGF- 1 promotes sebaceous gland proliferation and sebum production in acne, while simultaneously influencing lipid metabolism and insulin sensitivity. The mTORC1, involved in lipid synthesis and cellular growth, exacerbates both acne and metabolic dysfunctions that predispose individuals to CVDs [33, 37].
Furthermore, it has been suggested that individuals with acne present frequently with dyslipidemia, probably also under androgenic influence, characterized by elevated total cholesterol, triglycerides, and low-density lipoprotein (LDL) cholesterol, along with reduced high-density lipoprotein (HDL) cholesterol levels [33, 34]. These lipid abnormalities are well-established risk factors for atherosclerosis and subsequent cardiovascular events. Studies on lipid profiles in patients with acne revealed that men, in particular, exhibited significant lipid derangements, including elevated triglycerides and LDL-cholesterol levels [33, 34]. This dyslipidemic profile enhances the atherogenic potential, contributing to the early onset of subclinical atherosclerosis [33, 38]. The higher androgenic hormonal effect in acne, coupled with chronic inflammation, creates a synergistic risk for cardiovascular pathology [33, 38].
Insulin resistance is a common feature in both acne and CVDs. Studies have shown that individuals with acne, especially adult males, exhibit higher fasting insulin levels and impaired glucose tolerance compared to controls [33]. Insulin resistance contributes to endothelial dysfunction, hypertension, and dyslipidemia, all of which are pivotal in the pathogenesis of CVDs [39].
Hyperinsulinemia, a consequence of insulin resistance, exacerbates acne by stimulating androgen production, increasing sebaceous gland activity, and promoting keratinocyte proliferation [39]. Simultaneously, it accelerates atherogenesis through pro-inflammatory pathways and adverse lipid profile alterations [33, 37]. The bidirectional relationship between acne and metabolic disturbances underscores the systemic nature of the disease and its cardiovascular implications [33, 37].
Hypertension, a major cardiovascular risk factor, has been associated with acne, particularly in males with persistent post-adolescent acne [34]. The androgen-driven pathogenesis of acne parallels mechanisms contributing to elevated blood pressure [40]. Androgens influence vascular tone by modulating the renin–angiotensin–aldosterone system (RAAS), enhancing sodium retention, and increasing sympathetic nervous system activity [33, 40].
Inflammatory cytokines such as IL- 6 and TNF-α, elevated in acne, also play a role in hypertension [33, 40]. IL- 6 promotes vascular inflammation and stiffness, while TNF-α contributes to endothelial dysfunction and arterial remodeling. These overlapping pathways highlight the inflammatory-hormonal axis linking acne to hypertension and broader cardiovascular risk [33].
Obesity and MetS are significant mediators in the acne-CVDs link. Patients with acne often exhibit higher BMI, increased waist circumference, and visceral adiposity, all of which are components of MetS. The adipose tissue in obesity acts as an endocrine organ, secreting pro-inflammatory adipokines that perpetuate systemic inflammation [33, 34, 37]. The mTORC1 signaling pathway, central to acne pathogenesis, is also activated in obesity and MetS, promoting lipid accumulation, insulin resistance, and inflammatory responses. Dietary factors, such as high glycemic index foods and dairy consumption, further exacerbate both acne severity and metabolic disturbances, reinforcing the interconnectedness of these conditions [33, 34, 37]. As a result, the recognition of acne as a potential marker for cardiovascular risk necessitates a paradigm shift in clinical management [33, 34]. Dermatologists and primary care providers should adopt a multidisciplinary approach, incorporating cardiovascular risk assessment into routine acne care. Screening for metabolic parameters such as lipid profiles, fasting glucose, insulin resistance, and blood pressure should be considered, particularly in patients with severe or persistent acne.
Lifestyle modifications, including dietary interventions, weight management, and smoking cessation, play a crucial role in mitigating cardiovascular risk in patients with acne [33, 34]. Pharmacological therapies targeting both acne and metabolic dysfunctions, such as metformin, have shown promise in improving insulin sensitivity and reducing inflammatory markers [41]. Additionally, anti-androgen therapies and isotretinoin may influence lipid metabolism, warranting careful cardiovascular monitoring during treatment [42].
Recognizing acne as part of a broader systemic inflammatory spectrum offers opportunities for early cardiovascular risk stratification and preventive interventions, ultimately improving long-term health outcomes in affected individuals.
Take Home Message
Acne vulgaris is a systemic inflammatory condition linked to dyslipidemia, insulin resistance, hypertension, and increased cardiovascular risk. Metabolic screening should be integrated into acne management, particularly in high-risk individuals. Targeted interventions, including dietary modifications, weight management, and drugs, may improve both dermatological and cardiometabolic outcomes.
The Role of Nutrition in Acne
The relationship between nutrition and acne remains a subject of ongoing research. While historically debated, growing evidence suggests that specific dietary components influence sebaceous gland activity, bacterial proliferation, and inflammation—key factors in acne development [43]. High-glycemic index foods, dairy products, chocolate, and saturated fats have been identified as potential aggravators [44, 45]. Additionally, alcohol, processed foods, gluten, and sugary beverages may contribute to acne flares, although further studies are needed to confirm these associations [46, 47].
Acne extends beyond physical manifestations, significantly impacting self-esteem, social interactions, and psychological well-being. Given its substantial effect on quality of life, identifying dietary triggers could serve as an adjunctive strategy in acne management [48]. Clinicians should consider personalized dietary recommendations alongside conventional treatments, encouraging patients to minimize acne-exacerbating foods while promoting a balanced, nutrient-rich diet [49].
Acne vulgaris is a chronic inflammatory condition influenced by multiple factors, including gut microbiota and diet [50, 51]. The Western diet, characterized by high saturated fat and high-glycemic index foods, is linked to acne through dysregulated nutrient signaling, increased sebum production, and Cutibacterium acnes overgrowth [52, 53]. A diet rich in fats and sugars may alter gut microbiota diversity, promoting inflammation and intestinal permeability, thereby exacerbating acne symptoms [54]. On the other hand, several dietary patterns have shown potential benefits in acne management. A vegetarian diet, emphasizing plant-based foods while limiting animal products, has been associated with improved acne outcomes [55]. Some studies suggest that eliminating dairy and high-glycemic foods may reduce acne severity by lowering IGF- 1, a key driver of sebum production and inflammation [56]. Vegan diets, which are rich in phytoestrogens and isoflavones, may further support acne reduction by modulating androgen activity and decreasing inflammatory markers [57], though more research is needed to confirm these effects.
Dietary modifications, particularly reducing dairy, processed foods, and high-glycemic foods while adopting plant-based patterns, may serve as supportive strategies for acne management [58]. However, further large-scale, well-controlled studies are necessary to establish definitive dietary guidelines for patients with acne. Until then, integrating dietary adjustments with medical interventions may provide a holistic approach to reducing acne severity and improving patient outcomes [59].
Take Home Message
Emerging evidence suggests that diet plays a role in acne development, with high-glycemic foods, dairy, and processed foods acting as potential aggravators. While more research is needed, adopting a nutrient-rich, plant-based or Mediterranean-style diet may help manage acne symptoms by reducing inflammation and sebum production. Personalized dietary recommendations, alongside conventional treatments, could offer a comprehensive approach to improving acne management.
The Impact of Mediterranean Diet on Acne
Numerous studies have expanded the role of the MedDiet beyond its well-established benefits in cardiovascular diseases to include dermatological diseases. In the context of acne, the MedDiet appears to have a positive impact, influencing both the risk of developing acne and its severity.
A community-based case–control study by Skroza et al. evaluated adherence to the MedDiet using a 10-point MedDiet scale in 293 individuals (93 individuals with acne and 200 healthy controls) [60]. Interestingly, logistic regression analysis showed that familial hypercholesterolemia, type 2 diabetes, and hypertension were strong risk factors for acne (AOR 8.79, 95% CI 1.67–46.22; 3.32, 95% CI 1.27–8.63; and 2.73, 95% CI 1.07–6.96, respectively), while the MedDiet represented a protective factor (score ≥ 6, AOR 0.31, 95% CI 0.11–0.89) [60].
Bertolani et al. conducted a study in 35 normal weight individuals aged 14—30 years affected by acne and treated in line with the European Dermatology Forum (EDF) guidelines [61]. Individuals were divided into 2 groups based on a questionnaire score assessing the adherence to the MedDiet: the Mediterranean Group (score ≥ 6, n = 27) and the Western Group (score < 5, n = 8). IGF- 1 levels were measured in all individuals before and after treatment and then compared to healthy population. IGF- 1 levels were higher in individuals with acne than in controls and in the Western group than in the Mediterranean group [61]. A case–control study by Ah-Thiane et al., enrolling 40 normal weight women with mild-to-severe acne, and 40 healthy controls, reported a significant negative association between acne severity and adherence to the MedDiet [58]. Further insights were provided by Barrea et al. in a cross-sectional study of 102 individuals (51 with acne, BMI 24.7 ± 4.1 kg/m2, and 51 healthy controls, BMI 24.6 ± 1.7 kg/m2) [62]. The authors reported worse body composition, including a lower phase angle (PhA) and reduced adherence to the MedDiet, in individuals with acne compared to controls, independent of age, sex, and BMI. Furthermore, both PhA and adherence to the MedDiet were significantly reduced in individuals with severe acne compared to those with mild or moderate forms [62]. Notably, PhA, a simple and accessible parameter derived from bioelectrical impedance analysis, serves as an indicator of cellular integrity and has recently been recognized as a surrogate marker of inflammation, with lower values indicating greater inflammatory status [63]. In contrast, a recent case–control study of 242 university students (71.9% normal weight) found no significant association between adherence to the MedDiet and acne diagnosis or severity [49].
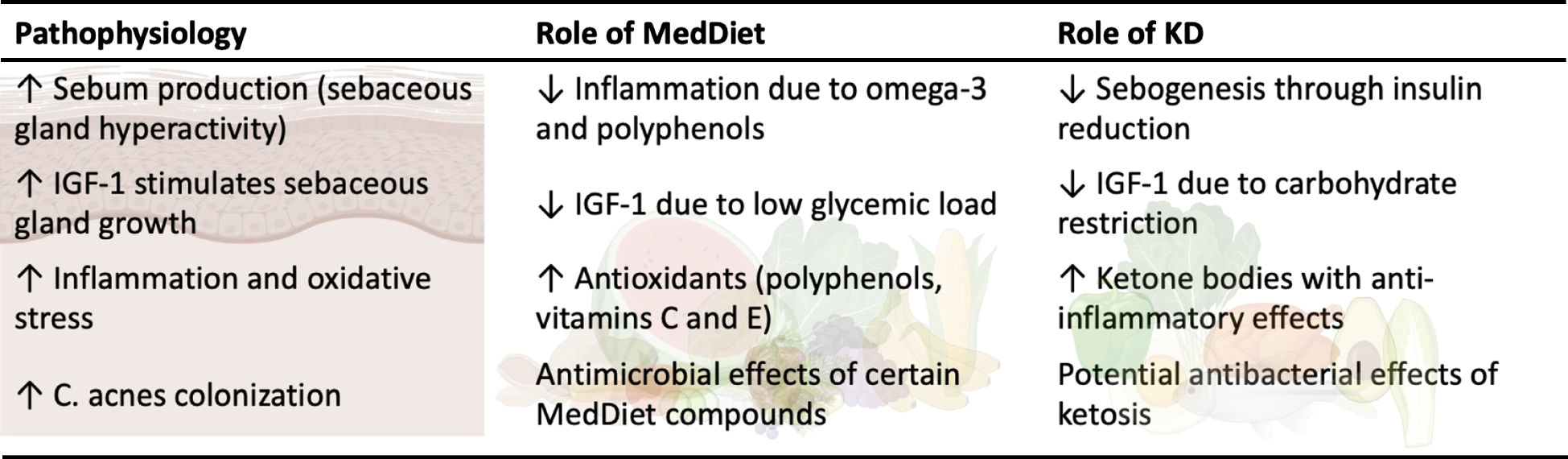
These findings underscore the potential role of the MedDiet in mitigating acne severity through mechanisms likely involving its anti-inflammatory and antioxidant properties [64]. Specifically, the high intake of fruits, vegetables, whole grains, and extra virgin olive oil associated with the MedDiet provides a rich source of polyphenols, vitamins, and omega- 3 fatty acids, which can reduce oxidative stress and modulate inflammatory pathways implicated in acne pathogenesis [64]. Additionally, the low glycemic load of the MedDiet may help regulate IGF- 1, a key driver of sebaceous gland activity and acne development [65].
However, study heterogeneity, small sample sizes, varying dietary assessment tools, and population differences limit generalizability (Table 1). Most studies are observational, precluding causal inferences. Longitudinal, randomized controlled trials are needed to confirm the MedDiet’s benefits in acne management.
Table 1 Clinical studies on the Mediterranean Diet and the Very Low-Energy Ketogenic Therapy in individuals with acne
Take Home Message
The MedDiet shows promise in reducing acne severity, likely due to its anti-inflammatory, antioxidant, and low glycemic properties. While findings suggest benefits, limitations of current research highlight the need for robust, randomized controlled trials to confirm its efficacy.
The Impact of the Ketogenic Diet on Acne
The first insights into the possible effects of ketosis on acne progression date back over ten years [66, 67]. The connection between ketogenic therapy and acne would find its rationale in the reduction of the glycaemic load of the diet, which, by regulating glycaemic and insulinemic homeostasis, would lead to beneficial effects on skin quality. In particular, the reduction of insulin levels would first of all inhibit the activity of IGF- 1, blocking a series of events involved in the pathogenesis of acne, such as hyperproliferation of keratinocytes in the pilosebaceous ducts, androgen-mediated hyperproduction of sebum, altered desquamation of the follicular epithelium, and proliferation of Propionibacterium acnes in the stratum corneum [66, 67]. The potential of ketosis i





Comments (0)