Summary of Findings
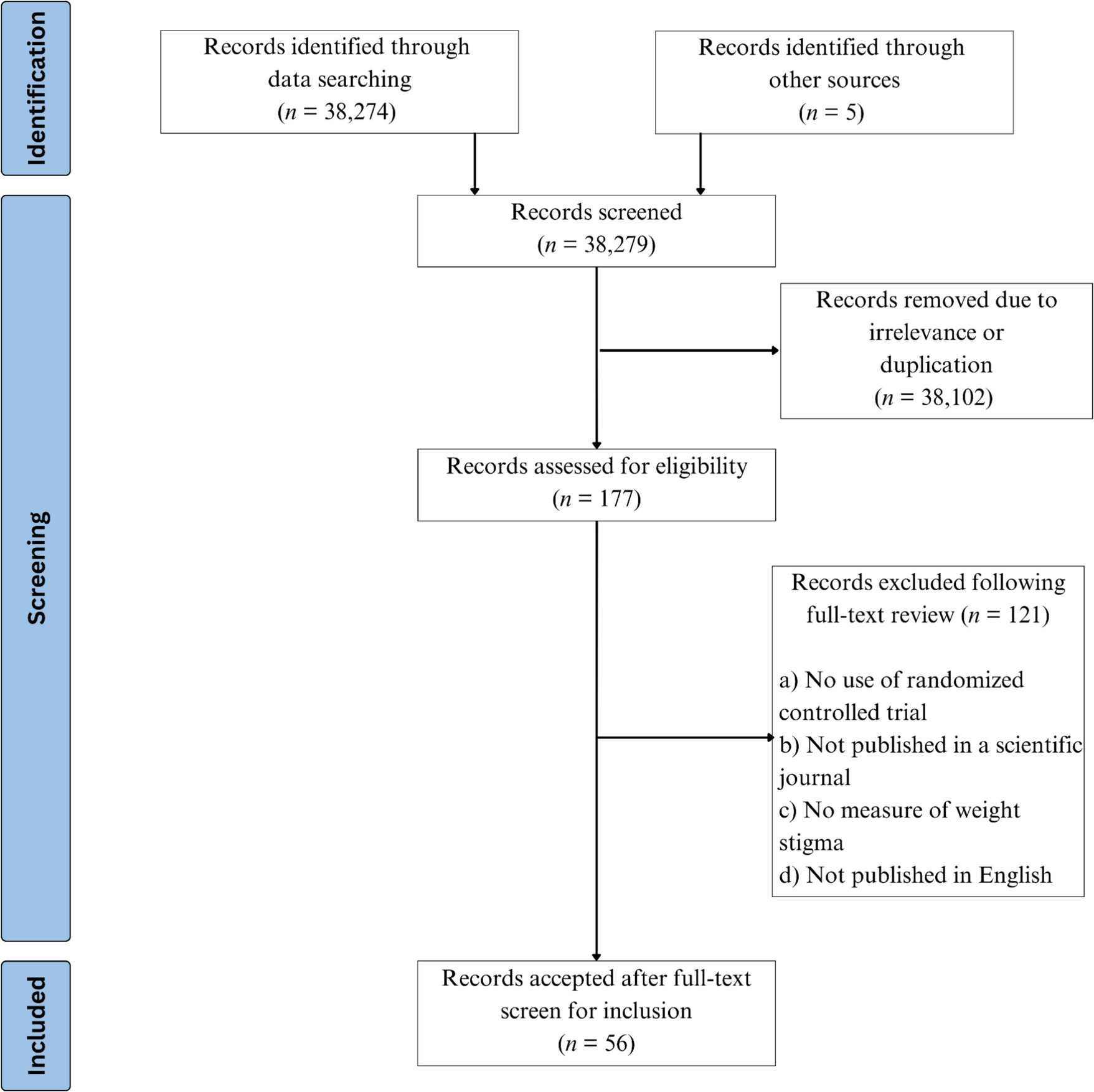
Among 38,274 articles, 56 RCTs met the inclusion criteria. Of these, 22 focused on adult populations, 16 on college students, 15 on healthcare and wellness professionals or students, two on children, and one on college students and adults in separate studies. A summary of the studies is presented in Table 1. A total of 23 RCTs were rated as poor, 21 as fair, and 12 as good (Supplemental Table S1). A narrative analysis revealed eight distinct strategies: 1) shifting causal attributions and reduction of controllability beliefs, 2) weight-inclusive frameworks, 3) empathy evocation, 4) cognitive dissonance, 5) building a connection with individuals with higher weight, 6) education on caring for individuals with higher weight, and 7) multiple methodologies. The results for the identified themes are discussed below.
Table 1 Summary of Randomized Controlled Trial Study CharacteristicsShifting Causal Attributions and Reducing Controllability Beliefs
Weight stigma can stem from the misconception that obesity is solely due to individual, controllable factors such as laziness or lack of discipline [27]. Some studies highlighted the impact of genetics, biology, and environmental influences on dismantling negative stereotypes [28]. We identified 15 articles that presented participants with scientific evidence on the complex nature of obesity, with two articles conducting two studies each [29,30,31,32,33,34,35,36,37,38,39,40,41,42,43]. All studies targeted external weight bias with varying results.
Nine studies employed this strategy to reduce weight bias among general adults, with seven reporting success [29, 31, 33,34,35,36,37,38, 42]. Among these, five used written materials, one used a five-minute educational video, and another invited individuals with obesity to discuss the causes of obesity. Two studies did not observe changes in weight-biased attitudes. Hilbert had participants view an hour-long interactive slideshow on weight controllability, which did not change stigmatizing attitudes relative to the control group [33]. Similarly, Berry and Myrne’s study using Obesity Canada’s ‘Bust the Bias’ short video, which explained that exercise may not impact body weight, had no impact on explicit or implicit bias, measured by the Fat Phobia Scale and the Implicit Association Test (IAT), respectively [29].
Interventions among college students yielded more consistent success, with three studies reporting at least partial improvements [32, 33, 40]. Frederick et al. found that college students who read articles challenging the controllability of fatness and condemning weight discrimination reported lower anti-fat attitudes and greater acceptance of size diversity [32]. O’Brien et al. conducted two experiments with college students, providing the intervention groups with either a food addiction or a diet and exercise explanation for obesity [40]. In the first experiment, students who received the food addiction explanation showed reduced anti-fat attitudes, particularly in the dislike subscale, which measures explicit prejudice toward higher body weight, and the willpower subscale, which assesses the belief that obesity results from a lack of self-discipline. However, in the second experiment, the decrease was limited to the dislike subscale, and the intervention group showed no significant difference from the control group. Hilbert’s intervention, although ineffective among their adult sample, successfully reduced explicit weight stigma among college students [33].
Three studies focusing on healthcare workers or students demonstrated changes in their participants’ weight-biased attitudes [39, 41, 43]. Persky et al. found that students who learned about the genetic mechanisms of obesity reported less negative stereotyping than those who read about a control topic [41]. O’Brien et al. found that healthcare students who learned about uncontrollable reasons for obesity reported reduced implicit anti-fat attitudes compared to those who learned about controllable causes or an unrelated health topic (control). Although intervention participants reported decreased dislike, explicit anti-fat prejudice did not differ across groups [39]. Speirs et al. reported that practitioners who received a food addiction explanation for obesity had lower anti-fat attitudes on the willpower subscale but not the dislike subscale compared to those who received a disease explanation [43].
Lastly, one study targeted elementary children [30]. Although children who read about an uncontrollable cause (biology) reported more positive attitudes toward an overweight peer than a controllable cause, overall group differences in attitudes were not significant.
Weight-Inclusive Initiatives
Weight-inclusive initiatives focus on body acceptance, self-compassion, and the promotion of health and well-being independent of body size, encouraging individuals to adopt healthy behaviors without emphasizing weight loss. Eleven studies employed weight-inclusive initiatives [44,45,46,47,48,49,50,51,52,53,54]. Seven of these studies focused on adults [44,45,46,47,48, 51, 52], with five comprising women [44, 45, 47, 48, 51]. Alleva et al. and Cha et al. reduced external weight bias by asking participants to write about the capabilities of a larger woman’s body and by displaying photos of higher-weight women exercising [44, 46]. Notably, we rated Alleva et al.’s study as good quality based on the NIH assessment. The remaining studies focused on internalized weight bias. Three studies implemented weekly sessions centered on self-compassion and mindfulness [45, 48, 51]. One study combined short videos of a woman expressing gratitude for her body’s functions [47], and another study asked participants to read a self-help book chapter about acceptance and commitment therapy [52].
Three studies with college students reported mixed results with weight-inclusive interventions [49, 50, 54]. Two studies focused on external weight bias. Wilson et al. reported a reduction in anti-fat attitudes among participants who attended sessions on increasing body acceptance and developing healthy dieting behaviors, with the effects sustaining after one month [54]. However, Lee et al. found that loving-kindness meditation, intended to foster compassion for oneself and others, failed to reduce fat-phobia bias [50]. Similarly, Huelleman et al., whose study was rated as good quality per the NIH assessment, found differences in internalized weight bias between participants who engaged in self-kindness and mindfulness writing exercises and those who wrote about appearance ideals for women or did not complete any writing exercises [49].
The final study targeting healthcare students also employed loving-kindness meditation. Using the Attitude Toward Obese Persons Scale and the IAT to measure explicit and implicit weight bias, respectively, found no differences in explicit or implicit weight stigma compared to the control group [53].
Inducing Empathy
Empathy-inducing interventions included narratives, personal testimonials, or immersive activities designed to help participants understand weight stigma’s emotional and psychological impact [55]. Two studies targeted external weight stigma [56, 57], and both rated good quality per the NIH assessment. Rodriguez et al. had college students experience life with higher weight by walking across the campus wearing a fat suit, but this did not significantly lower anti-fat attitudes compared to controls [56]. Matharu et al. focused on healthcare students and reported partial success in changing participants’ weight-biased attitudes [57]. Their intervention involved a 60-minute dramatic reading of The Most Massive Woman Wins and a group discussion. Participants in the intervention group reported reduced anti-fat attitudes compared to the control group. However, there were no differences in implicit weight bias across groups.
Cognitive Dissonance
Festinger’s cognitive dissonance theory suggests that inconsistencies between beliefs, attitudes, and actions create psychological discomfort, motivating individuals to resolve the discrepancy by adjusting their beliefs and attitudes [58]. Three studies examined cognitive dissonance as a strategy for preventing weight stigma among college students [59,60,61]. Two studies focused on external weight bias. One, rated as good quality per the NIH assessment, presented participants with either a cognitive dissonance intervention, highlighting inconsistencies between their attitudes and values of kindness and equality, or a social consensus intervention, suggesting their views were more stigmatizing than their peers [59]. The cognitive dissonance intervention reduced explicit anti-fat attitudes, whereas the social consensus intervention showed no difference from controls. Another study employed a similar cognitive dissonance strategy [60]. They found that, at the one-week follow-up, intervention participants reported lower explicit anti-fat attitudes than the control group, but implicit attitudes remained unchanged. Lastly, Kramer et al. explored cognitive dissonance through two writing-based interventions aimed at addressing both external and internal weight bias [61]. These writing interventions required participants to either give advice to hypothetical pre-teenage girls about body image based on personal experience or argue against legal policies discriminating against individuals with higher weight. Both interventions reduced explicit anti-fat bias compared to the control, but only the former led to reductions in implicit bias.
Building Connection
Interventions designed to build connections emphasize shared humanity, values, and positive contact with “outgroup” individuals. This category of intervention includes the induction of “a sentimental longing or wistful affection for the past” to increase social connections and thereby reduce weight stigma. Six studies employed interventions under this category [62,63,64,65,66,67]. Three studies targeted adults. Brochu et al. and Dunaev et al. targeted external weight bias and found reduced weight bias attitudes in the intervention groups compared to the control groups. In Brochu et al.’s study, intervention participants read about weight-related issues in the United States, emphasizing a shared identity as Americans [64]. These participants reported lower levels of weight bias compared to control participants. In Dunaev et al.’s study, intervention participants who imagined interacting with a confident and attractive person with obesity reported lower levels of weight bias than those who imagined interacting with an insecure and unattractive person with obesity [65]. Myre et al. addressed internal weight bias, focusing solely on female participants [67]. They exposed intervention group participants to images of active individuals with obesity paired with positive words related to physical activity. Women in the intervention group reported reduced internalized weight bias, and this effect persisted for one week.
The remaining three focused on college students. Koball and Carel’s study reported reduced external weight bias [66]. Intervention participants who engaged in direct interaction with a confederate with obesity exhibited lower weight bias and greater behavioral intentions to interact with individuals with obesity compared to those in the control group and who watched a video of a positive interaction between friends of mixed weight status. The other two studies were conducted by Turner et al. Both involved asking participants to imagine a sentimental, nostalgic interaction with a higher-weight individual [62, 63]. In two samples, participants in the nostalgic interaction condition exhibited more positive attitudes toward higher-weight individuals compared to the control [62]. Similarly, the second study found that the nostalgia intervention led to more positive attitudes than the control [63].
Providing Education on Caring for Individuals with Obesity
Educational interventions were also used. These aimed to challenge stereotypes surrounding weight stigma, provide evidence-based information, and teach techniques to counteract weight bias. Three studies used this strategy [68,69,70]. Hague and White targeted the general adult population with an educational module covering the causes of obesity, the negative effects of weight stigma, and strategies to address it [68]. Participants reported reduced anti-fat attitudes after the intervention, with effects sustained for six weeks.
Two studies focused on reducing external weight stigma by increasing education on caring for larger individuals among healthcare professionals and students. Sherf-Dagan et al. developed a good-quality study, as rated by the NIH assessment, of a 15-minute online educational module covering obesity, the definition and impact of weight bias, strategies for reducing weight bias, and a quiz [69]. The intervention decreased fat-phobic attitudes over 30 days, though there were no changes in anti-fat attitudes between groups over time. Oliver et al. designed a longer educational intervention for healthcare students, covering obesity prevalence, the impact of weight bias in healthcare, and strategies for reducing bias in clinical settings [70]. Beyond watching and discussing a video on weight bias and completing reflective journaling exercises, the intervention group received two additional training sessions, personalized feedback on their weight bias scores, case-based learning scenarios requiring critical thinking, and a group discussion on their reflections. The intervention group reported more favorable beliefs about individuals with obesity but not in their attitudes toward individuals with obesity compared to the control group.
Combining Multiple Approaches
Sixteen studies employed interventions that combined two or more strategies [71,72,73,74,75,76,77,78,





Comments (0)