
Remember me

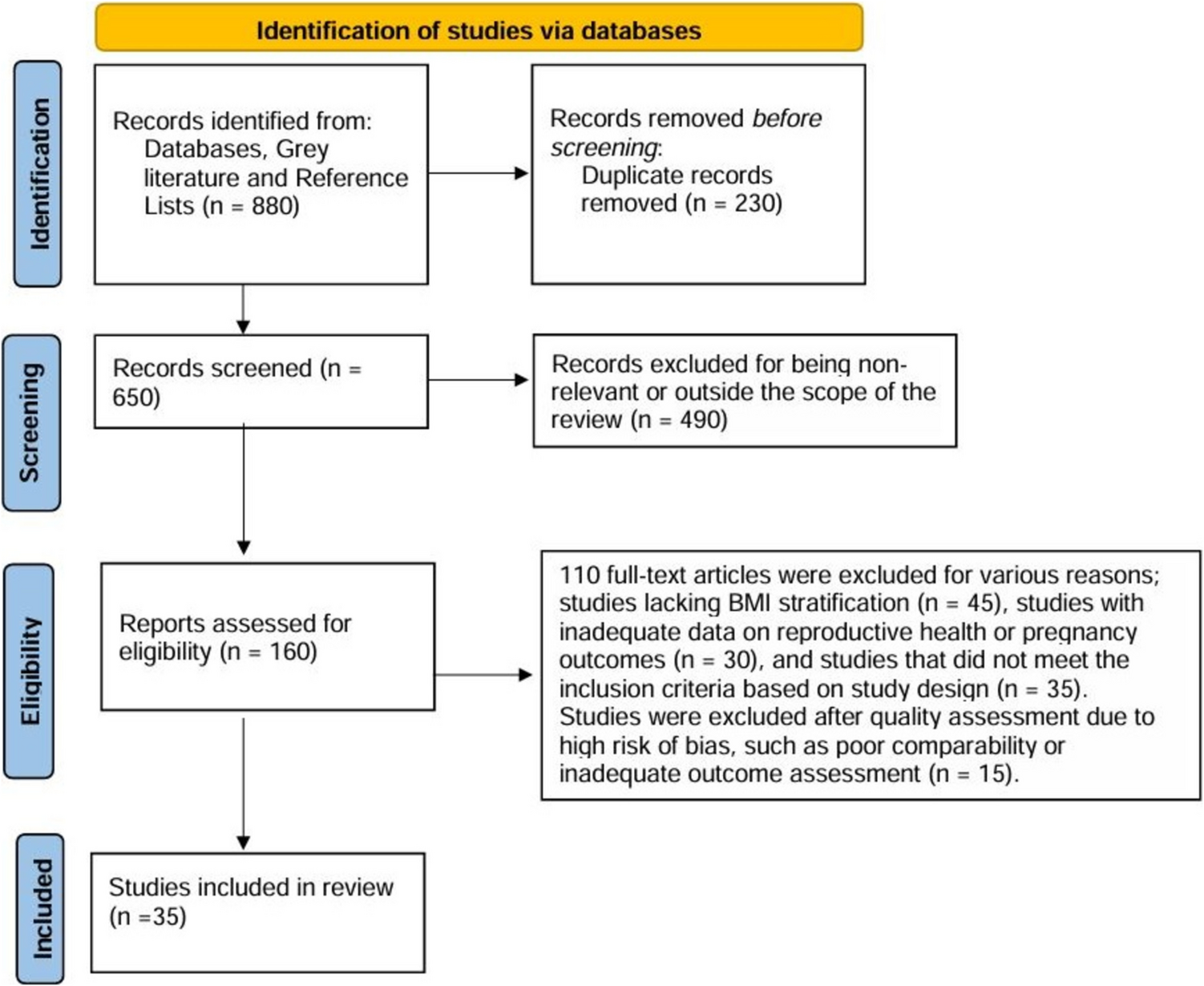



The systematic review included a total of 35 studies [15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49]. The included studies represented a wide geographical distribution, with research conducted across North America, Europe, Asia, and Oceania. Notable contributions came from the USA, UK, China, Australia, and several European countries, reflecting the global concern over obesity-related reproductive health issues and adding cultural and clinical diversity to the findings. The study designs predominantly consisted of retrospective and prospective cohort studies, along with some cross-sectional studies and analyses of clinical trial data. Sample sizes varied widely, ranging from small cohorts of fewer than 50 participants to large population-based analyses with over 10,000 subjects. The studies covered diverse populations, including women undergoing ART like in vitro fertilization (IVF), pregnant women stratified by BMI, and men evaluated for fertility. They measured parameters such as gestational and neonatal outcomes, hormonal profiles, ovarian and sperm morphology, embryo quality, and live birth rates.
Summary of the included studies’ characteristics is displayed in Tables 1, 2, 3, and 4.
Table 1 Studies regarding mechanisms linking obesity to reproductive dysfunctionTable 2 Studies regarding impact of obesity on male fertilityTable 3 Studies regarding impact of obesity on ART outcomesTable 4 Studies regarding maternal and neonatal outcomes associated with obesity during pregnancyMechanisms Linking Obesity to Reproductive DysfunctionObesity significantly influences various mechanisms linked to reproductive dysfunction, including metabolic, hormonal, and ovarian morphological changes.
Impact of Obesity-Driven Metabolic DysregulationGrieger et al. [15] identified that metabolic syndrome (MetS), which often co-occurs with obesity, is independently associated with longer time to pregnancy (TTP) and increased infertility risk. Key metabolic markers, such as raised triglycerides and reduced high-density lipoprotein cholesterol (HDL-C), were strongly correlated with infertility, highlighting the role of specific metabolic abnormalities beyond overall obesity in delaying fertility.
Hormonal Changes and Embryo QualityLin et al. [16] demonstrated that elevated leptin levels in the follicular fluid of overweight and women with obesity were negatively correlated with embryo quality. This was evidenced by reduced good-quality embryo rates and poorer clinical pregnancy and live birth outcomes among these women. These findings suggest that high leptin levels impair granulosa cell function, leading to compromised embryo development and fertility outcomes.
Dietary Interventions and Ovarian MorphologyKazemi et al. [17] reported that higher adherence to dietary quality indices, such as the Mediterranean and Dietary Approaches to Stop Hypertension (DASH) diets, was associated with improved ovarian morphology, as reflected in decreased ovarian volume (OV) and follicle number per ovary (FNPO). These effects were mediated through reductions in obesity BMI and waist circumference (WC), insulin resistance, and hyperandrogenism. The study emphasizes the potential of dietary interventions in mitigating obesity-related ovarian dysfunction.
Ovarian Antral Follicle Dynamics and Endocrine FunctionOldfield et al. [18] found that women with obesity exhibited significant alterations in ovarian antral follicle dynamics, including reduced recruitment events, fewer selectable follicles, and lower anti-Müllerian hormone (AMH) levels. Additionally, luteal phase defects were markedly more prevalent among women with obesity, affecting 76% compared to 29% in non-obese women. These disruptions occurred despite regular menstrual cycles, indicating that obesity suppresses ovarian function at multiple levels.
Impact of Obesity on Male FertilityObesity detrimentally affects male fertility through alterations in hormonal balance, sperm quality, and molecular characteristics, as well as by influencing early embryonic development.
Hormonal DysregulationBieniek et al. [19] found that men with obesity exhibited significant reductions in total testosterone, free testosterone, and sex hormone-binding globulin (SHBG) levels, alongside elevated estradiol levels. However, semen parameters such as volume, count, motility, and morphology remained unaffected across BMI categories. These findings suggest a strong link between obesity-induced hypogonadism and male reproductive dysfunction.
Decline in Sperm QualityObesity was associated with poorer sperm motility and increased DNA fragmentation. Kort et al. [20] observed that men with obesity had significantly fewer normal-motile sperm and higher sperm DNA fragmentation indices (DFI). Similarly, La Vignera et al. [21] reported increased sperm apoptosis, chromatin decondensation, and DNA fragmentation among men with obesity, emphasizing the adverse impact of elevated BMI on both conventional and non-conventional sperm parameters.
Semen Function and Epididymal ActivityMartini et al. [22] highlighted that obesity negatively affects total and rapid sperm motility, as well as epididymal function, measured by N-acetyl-glucosaminidase (NAG) levels. Seminal fructose levels were positively associated with BMI, but sperm morphology, concentration, and testosterone levels remained unchanged.
Age-BMI Interaction in Sperm ProductionPaasch et al. [23] reported that higher BMI was correlated with reduced total sperm count (TSC), total cell number (TCN), testosterone levels, and inhibin-B concentrations. The effects of BMI were most pronounced in younger men aged 20–30, where obesity significantly impacted TSC and TCN.
Molecular Effects and Embryo DevelopmentRaad et al. [24] revealed that obesity adversely affects sperm chromatin integrity, DNA methylation, and oxidative stress levels. These molecular abnormalities were linked to delayed embryonic cell cycles (CC1, CC3), indicating that paternal obesity compromises early embryonic development.
Impact of Obesity on ART OutcomesObesity is a well-documented risk factor negatively influencing outcomes in ART. Its effects span reduced ovarian response, compromised oocyte and embryo quality, impaired uterine receptivity, and altered metabolic conditions, ultimately leading to lower pregnancy and live birth rates.
Ovarian Response and StimulationWomen with obesity undergoing ART require higher gonadotropin doses and longer stimulation durations. Pinborg et al. [25] and Devranoğlu et al. [26] reported fewer retrieved oocytes and lower embryo yields in women with obesity. These patients also demonstrated lower live birth rates. Caillon et al. [27] emphasized that while obesity does not inherently compromise ovarian stimulation when protocols are adjusted, it results in increased transfer cancellations and miscarriage rates. Haghighi et al. [28] suggested that weight loss prior to ART could mitigate obstetric complications without significantly altering ovarian response.
Oocyte and Embryo QualityObesity impacts on oocyte morphology and embryo development. Leary et al. [29] highlighted smaller oocytes altered glucose metabolism, and higher triglyceride levels in embryos from women with obesity, impairing blastocyst quality. Bellver et al. [30] observed a reduction in implantation and live birth rates in ovum donation recipients with obesity, implicating poor uterine receptivity and systemic metabolic dysfunction. Zhang et al. [31] showed minimal stimulation IVF may preserve oocyte quality better than conventional protocols in patients with obesity.
Uterine Receptivity and ImplantationObesity adversely affects uterine receptivity. Luke et al. [32] found higher rates of implantation failure and reduced live birth rates in women with obesity using autologous oocytes, with donor cycles showing no such disparities, confirming uterine involvement. Bellver et al. [30] further underscored the role of obesity in reducing implantation rates across BMI categories.
Pregnancy and Live Birth OutcomesObesity is associated with lower live birth rates and higher miscarriage risks. Veleva et al. [33] and Chavarro et al. [34] reported significantly reduced live birth rates in women with obesity undergoing ART, alongside increased miscarriage risks. These adverse outcomes persisted despite weight loss interventions. Kim et al. [35] linked obesity to diminished ovarian reserve, but not to gamete production in ART.
Metabolic Syndrome and ART ChallengesMetS exacerbates poor ART outcomes. He et al. [36] noted poorer ovarian response, fewer retrieved embryos, and reduced cumulative live birth rates in women with MetS undergoing ART, necessitating metabolic management prior to treatment. Kudesia et al. [37] showed increased cycle cancellations and fewer usable embryos in women with obesity, particularly those with PCOS.
Tailored ART ProtocolsPersonalized approaches may alleviate some adverse effects. Orvieto et al. [38] demonstrated that patients with obesity achieved comparable oocyte and embryo quality to non-obese patients when large follicles (> 15 mm) were aspirated, suggesting that stimulation response, rather than intrinsic oocyte quality, is the limiting factor. Legge et al. [39] reported no significant differences in clinical pregnancy or live birth rates between BMI groups when protocols were adjusted, highlighting the importance of individualized stimulation.
Maternal and Neonatal Outcomes Associated with Obesity During PregnancyObesity during pregnancy is a significant risk factor for adverse maternal and neonatal outcomes. These outcomes include gestational complications, altered delivery modes, and neonatal metabolic and physical health risks.
Maternal ComplicationsObesity increases the likelihood of gestational hypertension, diabetes, and excessive gestational weight gain. Aly et al. [40] and Joy et al. [41] reported that maternal obesity significantly raises the risks of hypertension, gestational diabetes mellitus (GDM), and cesarean delivery, with severity of obesity correlating with increased risks. Sabolović Rudman et al. [42] observed that women with obesity and GDM experienced higher gestational weight gain and hypertension rates compared to their normal-weight counterparts. Shen et al. [43] highlighted prepregnancy obesity as a key predictor of gestational weight gain and cesarean delivery, emphasizing the need for early intervention.
Mode of DeliveryObesity is a leading factor for increased cesarean delivery rates: Magriples et al. [44] noted that women with obesity and overweight women had higher cesarean delivery risks, independent of gestational weight gain or infant size. Melchor et al. [45] confirmed a strong association between obesity and cesarean delivery, with an adjusted odds ratio (aOR) of 2.76 for women with obesity compared to those with normal BMI.
Neonatal OutcomesObesity influences neonatal health through macrosomia, increased neonatal intensive care unit (NICU) admissions, and altered metabolic profiles. Dickey et al. [46] reported that maternal BMI affects neonatal outcomes differently in singleton versus twin pregnancies, with singletons showing a higher risk of macrosomia while NICU admission rates were elevated across all BMI groups in twins. Adwani et al. [47] noted higher rates of macrosomia and perineal injuries in women with obesity, particularly in class III obesity. Melchor et al. [45] observed a two- to threefold increase in macrosomia rates among mothers with obesity, with associated neonatal complications such as higher NICU admissions.
Risk of MiscarriageObesity is linked to increased miscarriage risk, particularly in the first trimester. Bhandari et al. [48] found a higher likelihood of early pregnancy losses in women with obesity with recurrent miscarriage, often linked to metabolic and endometrial dysfunction.
Impact of Gestational Diabetes MellitusObesity exacerbates the adverse effects of GDM. Yogev et al. [49] observed that while obesity and morbid obesity both impair pregnancy outcomes, insulin treatment improves results compared to diet-only interventions.
Preterm BirthThe relationship between obesity and preterm birth is complex. Dickey et al. [46] reported that obesity in singleton pregnancies reduces preterm birth risks, but the effect does not extend to twin pregnancies. Shen et al. [43] and Melchor et al. [45] found no significant difference in preterm birth rates across BMI groups.
Figure 2 summarizes the multifaceted effects of obesity on male and female reproductive function, ART outcomes, and pregnancy-related complications.
Fig. 2
Multifaceted Effects of Obesity on Male and Female Reproductive Function, ART Outcomes, and Pregnancy-Related Complications. ART: assisted reproductive technique; GDM: gestational diabetes mellitus; NICU: neonatal intensive care unit
Comments (0)