Patient Selection
A retrospective review of patient records from January 2010 to August 2019 was conducted to identify individuals who underwent radical esophageal cancer surgery at the institution. Following comprehensive screening, a cohort of 96 patients diagnosed with postoperative LNR in pT2-3 N0M0 ESCC was ultimately selected for inclusion in the analysis. Furthermore, detailed documentation of the precise anatomical locations of LNR was meticulously maintained for subsequent evaluation.
Inclusion criteria were as follows: (1) patients who had undergone radical surgery with complete tumor resection (R0 resection); (2) patients whose postoperative pathological examination confirmed ESCC; (3) patients with postoperative pathological staging classified as pT2-3 N0M0 (in accordance with the 8 th edition of the American Joint Committee on Cancer TNM staging system); (4) patients who had not received any form of neoadjuvant or adjuvant anti-tumor therapy; (5) patients who subsequently developed LNR following surgical intervention; (6) patients for whom radiological evidence documenting the initial site of LNR post-surgery was available.
Exclusion criteria were as follows: (1) patients whose age was below 18 years or exceeded 85 years; (2) cases with incomplete postoperative clinical and pathological documentation; (3) patients diagnosed with a secondary primary malignancy or multiple-site neoplasms; (4) cases where precise information regarding postoperative LNR was unavailable; (5) patients presenting with cervical esophageal cancer or gastroesophageal junction tumors.
Follow-up
Following esophagectomy, a standardized surveillance protocol is implemented as follows: during the initial 2-year period, patients are monitored at 2–4-month intervals; subsequently, from years two through five post-operatively, assessments are conducted biannually; beyond the 5-year mark, annual evaluations are performed. The primary diagnostic modalities employed during these surveillance visits encompass CT scans of the cervical, thoracic, and abdominal regions. Supplementary ultrasonographic examinations of the cervical or abdominal areas may be executed when deemed appropriate. Upon detection of pathological abnormalities, contrast-enhanced CT or magnetic resonance (MR) imaging is indicated for comprehensive evaluation. When clinically warranted, additional diagnostic procedures, including positron emission tomography (PET), fine-needle aspiration cytology, and histopathological examination of biopsy specimens, are utilized to establish definitive diagnoses. The surveillance terminus for all study participants was established in December 2021.
Diagnostic Criteria for LNR
The diagnosis of regional LNR is predominantly dependent upon imaging modalities, such as contrast-enhanced CT, MR, and PET. For superficial lymph nodes, a definitive diagnosis can be directly established through cytological biopsy procedures.
The diagnostic criteria for LNR have been established as follows: (1) when contrast-enhanced CT or MR imaging demonstrates a lymph node with a short-axis diameter ≥ 10 mm, or when ≥ 3 lymph nodes are identified within the same anatomical region, or when evidence of lymph node necrosis or extracapsular invasion is observed; (2) when lymph nodes are visualized within the tracheoesophageal groove, irrespective of their dimensional parameters, accompanied by clinical manifestations of hoarseness or vocal cord paralysis; (3) when sequential imaging studies reveal temporal alterations in lymphatic structures, characterized by substantial volumetric enlargement, numerical increases, or the emergence of previously undetected lymph nodes; (4) when definitive evidence of malignant metastasis is procured through fine-needle aspiration cytology or histopathological biopsy specimens; (5) when PET examination demonstrates a standardized uptake value ≥ 2.4.
Regional Lymph Node
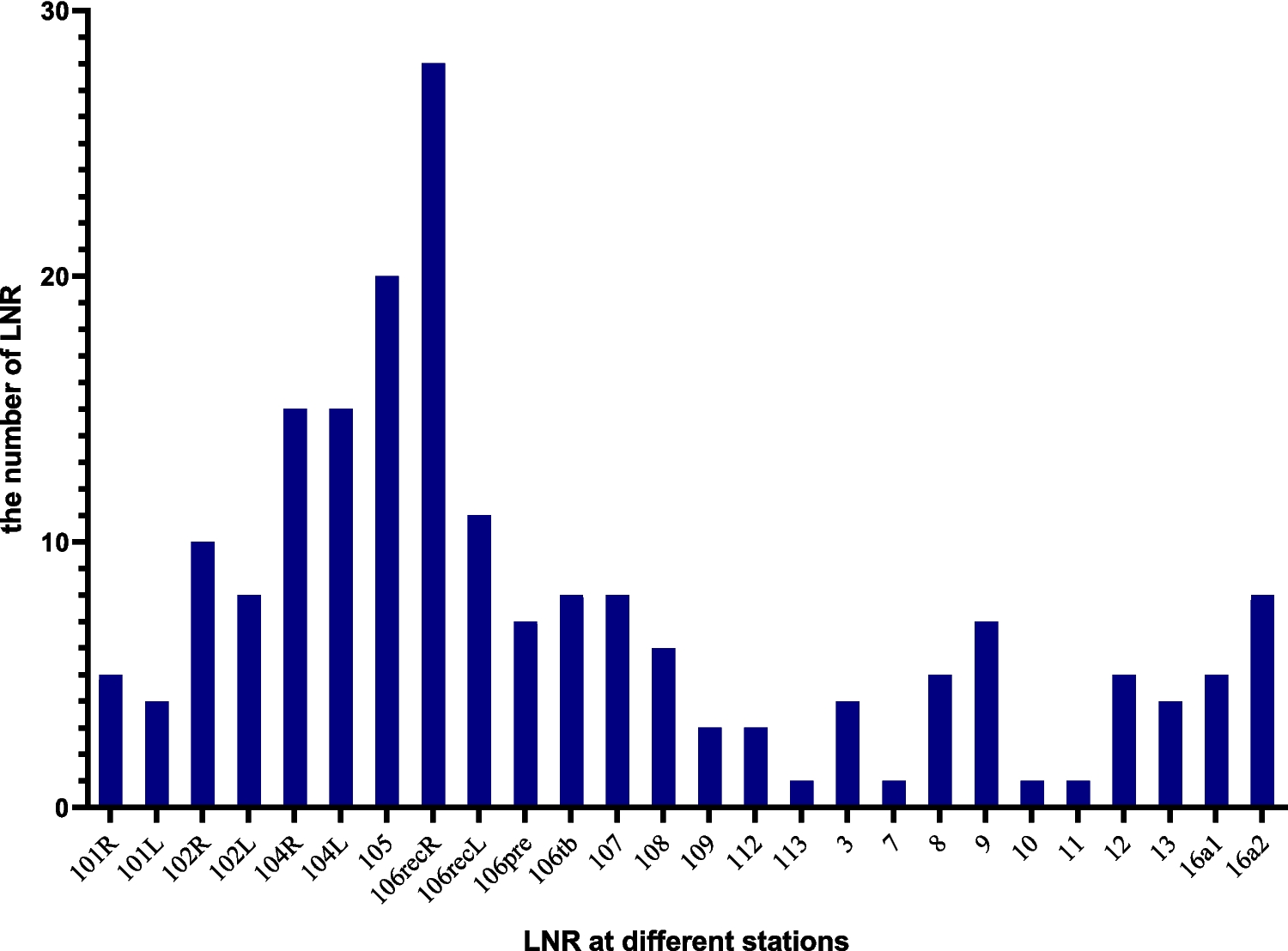
The LNR localization was determined in accordance with the standard lymph node anatomical classification delineated by the Japan Esophagus Society and the anatomical distribution of abdominal lymphatic drainage in gastric cancer. Recurrent sites were subsequently categorized into three distinct regions: the cervical lymph node drainage area, the mediastinal lymph node drainage area, and the abdominal lymph node drainage area [7, 8].
The specific lymph node zones were classified as follows: (1) cervical lymph nodes: comprising No.100, No.101, No.102, No.103, and No.104 lymph nodes; (2) mediastinal lymph nodes: subdivided into thoracic upper mediastinum nodes (No. 105, No. 106 tb, No.106recR/L, 106pre), thoracic middle mediastinum nodes (No.107, No.108, and No.109), and thoracic lower mediastinum nodes (lower No.110, No.111, No.112, No.113, and No.114); (3) abdominal lymph node region: encompassing group 1–16 lymph node regions within the abdominal cavity as designated in gastric cancer classification.
CT Images Reconstruction of LNR
Owing to the notable morphological alterations in anatomical structures, including the anastomotic site and the mediastinal stomach subsequent to radical esophagectomy, a 65-year-old male subject was designated as the reference patient for CT examination. The subject was positioned in a supine orientation on a stabilized framework, with upper extremities crossed anteriorly to the frontal region and bilateral cubital articulations naturally situated lateral to the cranium. The imaging parameters encompassed a scanning trajectory extending from the cricoid cartilage level to approximately 2 cm inferior to the bifurcation of the abdominal aorta, with subsequent image reconstruction performed at a slice thickness of 1.25 mm.
The patient’s CT scan images were imported into the radiotherapy contour delineation software system (version V1.0.0.19001) and the Pinnacle radiotherapy planning system (version 9.8.0.6007, Philips Medical Systems, Fitchburg, WI, USA) for subsequent volumetric image delineation and three-dimensional reconstruction.
With reference to anatomical landmarks, including adjacent organs, vascular structures, and osseous formations, the locations of recurrent lymph nodes were delineated on corresponding anatomical positions in the standardized patient’s CT images by two radiation oncologists in collaboration with a radiologist. The site of the initial LNR was exclusively documented. When multiple recurrent sites were identified simultaneously or within a 1-month interval, individual markings were applied, provided that the central points could be differentiated. Positive lymph nodes were designated by circular markers of a 6-mm diameter positioned at the nodal central points. In certain instances, lymph nodes demonstrated confluent patterns. Where differentiation was possible, markers were distributed with maximal uniformity; otherwise, a single marker was placed at the central point of the confluent mass.
Statistical Analysis and Image Processing
Statistical analyses of categorical and continuous variables were conducted utilizing IBM SPSS Statistics software (version 27.0; IBM Corp., Armonk, NY, USA). The Mann–Whitney U test was specifically employed for the comparative assessment of non-parametric continuous variable distributions. Statistical significance was established at P < 0.05.
The GraphPad Prism 9 software was employed for the quantitative analysis of lymph node distribution, whereas radiotherapy contour delineation software and the Pinnacle radiotherapy planning system (version 9.8.0.6007; Philips Medical Systems, Fitchburg, WI, USA) were implemented for CT image reconstruction.

Comments (0)