
Remember me



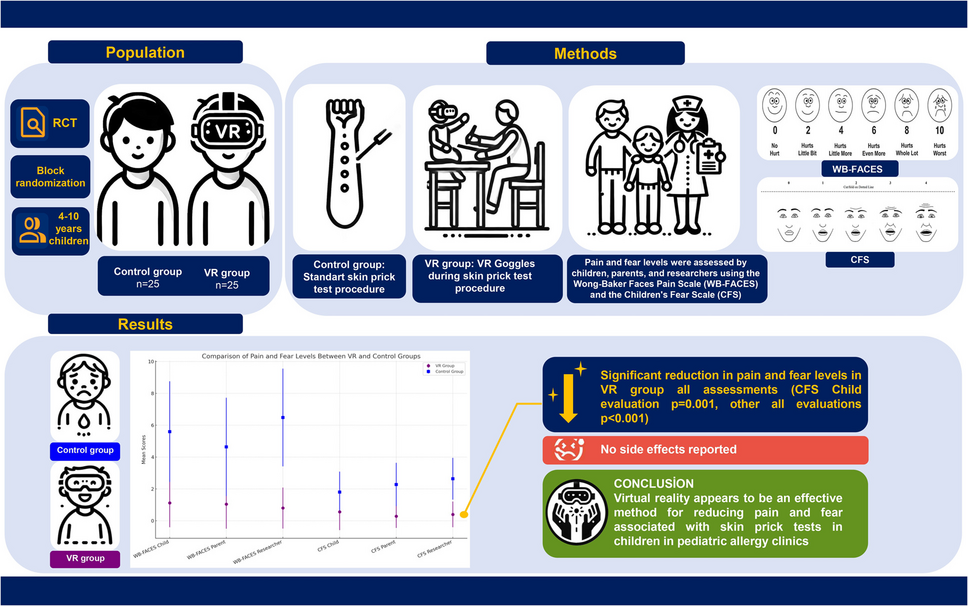
This parallel-group, single-blind, prospective, randomized controlled trial screened children evaluated at the skin testing unit of a tertiary pediatric allergy referral center in Türkiye between March and June 2024 (ClinicalTrials.gov registration NCT06421779). The study adhered to the CONSORT guidelines [28].
Sample size and randomizationThe number of participants was determined using data obtained from the reference study by Erdoğan et al. [19]. Power analysis was performed based on Wong-Baker FACES® Pain Rating scale data from the reference study comparing the VR group with the control group, which used the same scale as our primary outcome measure. At calculation by G*Power 3.1.9.7, the effect size was 0.92, the alpha margin of error was 0.05, and the statistical power was 80%, and it was determined that at least 19 participants in each group would be required. The analysis showed that a total sample size of 38 participants would be sufficient to detect significant differences. In consideration of potential losses of 10% that might occur during the study, we planned to include at least 21 participants in both groups for a total of 42 participants.
Previous studies have shown that gender and age affect pain and fear associated with invasive procedures in children [29]. Seventy-five children aged 4–10 years who met the inclusion criteria were divided into two groups as the VR group (n = 25) and the control group (n = 25) by block randomization using gender (boys and girls) and age group variables (4–6 years/preschool and 7–10 years/school). A blocked randomization list was developed using an online randomization tool [30]. This age group was selected since the Wong-Baker FACES® Pain Rating Scale (WB-FACES®) and the Children’s Fear Scale (CFS), which we use for pain and fear assessment, have a common validation age range for Turkish children.
Study populationThe criteria for inclusion in the study were (1) age 4–10 years and (2) the skin prick test being required due to allergic diseases, and (3) being scheduled to undergo a skin prick test an aeroallergen panel.
Exclusion criteriaExclusion criteria were (1) the presence of chronic diseases (except for allergic diseases), (2) vision, hearing, and speech disorders, (3) psychiatric and neurological diseases (including epilepsy, cerebral palsy, developmental delays, autism spectrum disorders, any condition affecting cognitive function or ability to cooperate with procedures), (4) mental status, learning and perception disorders, (5) a history of pre-procedure sedative, analgesic or narcotic drug use within the previous 24 h, (6) a history of active infection, (7) being scheduled to undergo a skin prick test other than an aeroallergen panel, (8) contraindications for skin prick testing, and (9) recurrent skin prick test history.
EthicsThis study was approved by the Clinical Research Ethics Committee of Aydın Adnan Menderes University (Approval Number: 2024/66) in accordance with the “Declaration of Helsinki.” All participants took part voluntarily, personal written informed consent being obtained from the parents of all children, and verbal consent from the children before participation.
Data collection toolsData were collected by means of a case report form created using WB-FACES® and CFS. Both scales are suitable for personal, parental, and researcher evaluation [31, 32]. In the present study, children’s personal, parental, and researcher reporting data were evaluated for both scales.
Wong-Baker FACES® Pain Rating Scale (WB-FACES®)WB-FACES® was developed by Wong and Baker in 1981 and revised in 1983. WB-FACES® is a reliable scale that has been validated for the Turkish population [33,34,35]. The scale is used to diagnose pain in children aged 3–18 years. It consists of six facial expressions, each representing an increasing degree of pain scored from 0 to 10 from left to right (0 = very happy face/no pain, 10 = a crying face/worst pain imaginable) (Fig. 1) [31].
Fig. 1
The Wong-Baker FACES® Pain Rating Scale
Children’s Fear Scale (CFS)The CFS was developed by McMurtry et al. in 2011 [32]. It was adapted into Turkish by Gerçeker et al. in 2018 in the context of children aged 4–10 years [36]. It consists of five facial expressions representing a range from neutral (0) to extreme fear (4) (Fig. 2).
Fig. 2
The Children’s Fear Scale
Virtual Reality (VR)Virtual reality represents an advanced technology that offers a 360-degree visual and audio simulation that surrounds the user and allows him to look in all directions [37]. In this study, the VR procedure was performed using a smartphone (Samsung Galaxy S23 Ultra), a VR goggle (Schulzz VRG Pro), and a VR underwater experience video (2160p resolution video suitable for VR format) capable of attracting the attention of the age groups involved. A small, open-design VR goggle that does not cover the forehead and in which the phone is placed externally was preferred to facilitate the assessment of the scales during the procedure.
ProcedureAll children were admitted to the skin testing unit with their parents. The researcher informed the participants and parents about the skin prick test and scales (WB-FACES® and CFS). Before the procedure, all participants were asked verbally about their baseline fear status concerning the skin prick test. Standard care in our clinic typically includes parental presence, verbal reassurance from healthcare providers, and allowing children to bring a comfort item. No formal distraction techniques such as toys, videos, or music were routinely used. For this study, participants were specifically instructed not to use any additional distraction methods to ensure the intervention effect could be properly evaluated.
VR equipment and setupWe deliberately selected an open-design VR goggle (Schulzz VRG Pro) that positions the smartphone externally to minimize coverage of facial areas. Headset straps were carefully adjusted for each patient to avoid covering the forehead area. Virtual reality goggles were sterilized after each participant’s use.
InterventionParticipants in the VR group wore VR goggles for approximately 2 min before the skin prick test and watched a VR underwater experience video throughout the procedure (Fig. 3). The control group underwent the routine skin prick test procedure without any distraction intervention.
Fig. 3
Illustration of VR-assisted skin prick testing
Assessment protocolTo enable comprehensive pain and fear evaluation, we implemented a multi-faceted assessment approach: (1) behavioral observations of visible indicators such as body tension, movement, and verbal expressions during the procedure, (2) formal pain and fear scale assessments conducted immediately after the procedure, and (3) evaluation by three different assessors (child, parent, and trained observer nurse) to capture multiple perspectives and minimize assessment bias.
Data collectionAll assessments occurred immediately after completion of the skin prick test (before the 15–20 min observation period for reading results). To minimize observer bias, a different specialist nurse (not the one who performed the procedure) who was specifically trained in the use of WB-FACES® and CFS scales conducted the pain and fear assessments. This observer nurse had prior experience in pediatric pain and fear assessment and received additional training on proper scale administration before the study. For children in the VR group, scale assessments were conducted directly after removing the VR goggles while the experience was still fresh in their memory. The evaluation sequence was standardized: first, the trained observer nurse asked the child to indicate their pain and fear levels, then asked the parent to provide their assessment, and finally completed her own evaluation. All assessments were recorded independently before any discussion between evaluators.
Skin prick testSkin prick tests were performed over the same period by a nurse with at least 5 years’ relevant experience. All patients underwent the same aeroallergen skin test panel. The tests were performed using a prick test applicator (MedBlue One, Türkiye) on the flexural aspect of the forearm by standard guidelines using standardized glycerinated extracts (1% weight/volume) from LOFARMA (Milan, Italy).
Statistical analysisSPSS version 23.0 statistical software (IBM SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Categorical variables were presented as numbers (%), and continuous variables as mean ± SD and median values (interquartile range (IQR)). Univariate analyses including categorical data were performed using the χ2 test. Data normality was assessed using the Shapiro–Wilk normality test, after which parametric values were analyzed using the Student’s t-test and non-parametric variables using the Mann–Whitney U test. A p-value of < 0.05 was considered statistically significant.
Comments (0)