
Remember me



The present study used a non-randomized interventional pre-post study design; each participant served as their own control with measurements taken before treatment (baseline) and then following treatment. The study was conducted with the purpose of evaluating the efficacy and safety of an orthodontic device that expands the pharyngeal airway. Specifically, the study aims were to assess if the device could reduce symptoms and signs of SDB and confirm treatment mechanism of action, as assessed by subjective and objective OSA severity and intermolar width, respectively. Additionally, airway volume was measured using cone-beam computed tomography (CBCT). The study is registered in ClinicalTrials.gov (https://clinicaltrials.gov/ct2/show/NCT05661747), the protocol was approved by the WCG Institutional Review Board, and the participants’ legally authorized representatives provided written informed consent to their study dentists before participation.
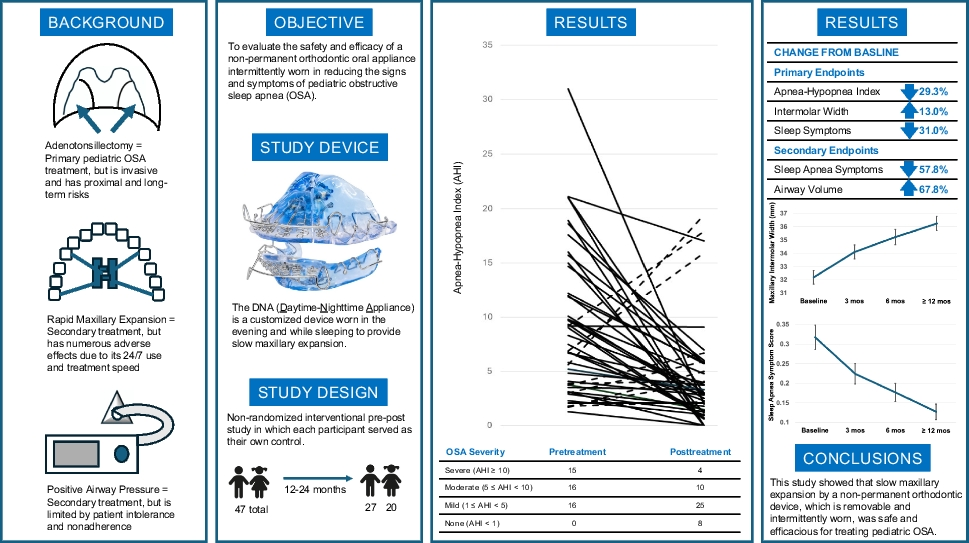
Study deviceThe DNA (Figure 1) is a customized oral appliance that is constructed from models of the patient’s teeth, using standard orthodontic acrylics and orthodontic wires for clasps and retention. The DNA may be adjusted antero-posteriorly, transversely, as well as permitting adjustments of the vertical dimension of occlusion. There is an optional extender on the device which further aids in opening the pharyngeal airway. The dentist prescribes the amount of acrylic to be utilized from a small amount of acrylic for a wire frame to complete coverage of the palate and the vertical dimension to meet the patient’s needs. At regular intervals (usually once a week, but at least once a month), the patient in most cases and/or dentist adjusts an expansion screw by 0.25 mm (or the dentist adjusts the loop) to expand the appliance as prescribed. The DNA is used in the evenings and at night by patients. Treatment usually lasts from 6 months to 24 months, but the dentist adjusts the treatment time as necessary to achieve the desired or stable results.
Fig. 1
Daytime-nighttime appliance (DNA)
Sites and participantsFive dental sites (four US sites and one Canadian site) agreed to participate in this clinical trial to confirm whether maxillary expansion with the DNA would improve SDB in children. Inclusion criteria consisted of age < 18 years, permanent teeth or mixed dentition at time of evaluation, diagnosis of sleep-disordered breathing (OSA AHI ≥ 1), in need of orthodontic treatment, and living in the USA or Canada. Exclusion criteria consisted of uncontrolled diabetes, any severe respiratory condition (e.g., chronic asthma, emphysema, and COPD), braces, and protocol nonadherence.
Endpoints and measuresThe three coprimary endpoints were as follows:
(1)Total score on the Pediatric Sleep Questionnaire (PSQ). The PSQ is a validated questionnaire for determining sleep-related breathing disorders, snoring, sleepiness, and behavior in children and was administered to participants at pre- and posttreatment (final visit).
(2)Sleep study-derived apnea-hypopnea index (AHI). Each participant received a home sleep apnea test (HSAT; Nox T3, Nox Medical, Reykjavík, Iceland or WatchPAT 300, ZOLL Medical Corporation, Caesarea, Israel) for pre- and posttreatment sleep studies at an AASM-accredited sleep center. The pretreatment sleep study was conducted within 1 year prior to the start of treatment. A sleep medicine physician not associated with the study and blinded to the pre- vs. posttreatment condition reviewed the HSAT data and assessed the participants’ degree of OSA, as they would for standard-of-care OSA management. WatchPAT 300 is cleared for ages ≥ 12 years (or > 65 pounds) and Nox T3 for ages ≥ 2 years. All children were tested with the same device at pre- and posttreatment (final visit).
(3)Intermolar width. Using a digital vernier caliper, the minimum intermolar width was measured from the cementoenamel junction of the lingual necks of the right and left maxillary first molars to reduce effects of any possible tipping of the teeth; this width was measured 3 times for each participant with the average reported. Although mandibular measurements are also usually obtained, maxillary intermolar width was the relevant measure for this study and was obtained pre- and posttreatment (final visit) as well as intermediate timepoints from consistent anatomical landmarks. Manual intermolar width using digital vernier calipers are considered generally reliable; deviations in intermolar width measurements between hand-held digital vernier calipers and digital analyses have been found to be clinically insignificant [14].
The secondary endpoints were as follows: (1) sleep-related breathing disorders (SRBD) subscale of the PSQ, which was administered at the pre- and posttreatment (final visit) plus intermediate timepoints, and (2) airway volume from cone-beam computed tomography (CBCT). CBCT images were obtained from participants by the treating dentists or referred for capture at a qualified facility for pre- and posttreatment (final visit). All dentists were taught how to reproducibly conduct CBCT measurements following a standard protocol that included strict head positioning, with a field of view characterized as large (13 cm) that was the minimum field to visualize all the required anatomy determined by a scout acquisition. Airway volume was measured by CBCT at a defined region of the pharynx described in an earlier published article [13]. A copy of the CBCT images was sent to a certified radiologist for review and a qualified dental CBCT examiner for analysis and assessment; both CBCT reviewers were not associated with the study. The analysis was sent back to the treating dentist with detailed measurements, including airway size, shape, and capacity (with airway volume measured at the narrowest point); standard orthodontic measurements; and comparison of the participant’s measurements to population standards.
All of these endpoints were measured at pre- and at posttreatment (final visit). For the objective measures, they were conducted according to standard protocols and without the DNA in their mouths. Sleep studies and CBCT images were reviewed by outside experts, minimizing bias and enhancing reliability.
Additional measures included the following: (1) device use, in which an estimate of average hours per 24-hour period of device usage were obtained from each participant at each posttreatment visit, and (2) safety parameters, which were evaluated at each visit, and included pain, tissue swelling, molar tip buccally, mandibular rotation or open bite, gingival recession, temporomandibular joint disorder, root resorption, change in bone density, loose teeth, or other concerns.
Device fabrication, fitting, use, and follow-up visitsThe orthodontic assessment by the treating dentist was conducted according to orthodontic diagnosis by the American Dental Association (ADA). The dentist obtained photographs (both intraoral and portrait), diagnostic casts of upper and lower arches, and dental radiographs (e.g., a full mouth series as needed). The dentist sent a device prescription and used these data and analyses to develop a design individualized for the participant upon which the DNA would be fabricated by a Certified Dental Laboratory (CDL). The dentist fitted the participant with the DNA and provided instructions for its use and maintenance. The instructions specified that the DNA is designed to be worn for 16 h/day (minimum of 10 h/day) for optimal results, with the best time of use when sleeping and relaxed times in the late afternoon and evening at home. From the DNA fitting date, a follow-up visit for additional adjustment within the initial 24–72 h could be scheduled with the dentist, with a subsequent 2-week visit to check the device fit, and then every 3–4 weeks thereafter (as indicated by standard-of-care orthodontic treatment). Participants completed the PSQ SRBD subscale at visits 2 weeks; 3, 6, 12 months; and additionally at 18 and 24 months (depending on the duration required for completion), with device adjustments made based on symptoms and comments made by participants and/or parents/guardians. The dentist concluded the study at any point after 6 months and up to 24 months when the participant achieved the desired orthodontic results, due to complications, or for any reason (e.g., participant request, dentist decision). Upon study completion, the dentist obtained the final diagnostic data, including a posttreatment sleep study and analysis by a sleep medicine physician, CBCT and analysis by dental examiners, intraoral radiographs (as needed), diagnostic photographs (intraoral and portrait), diagnostic casts, and case report forms. All study tests and procedures are considered standard-of-care orthodontic treatment, except for the posttreatment sleep study and posttreatment CBCT.
Treatment completion criteriaParticipant treatment was complete when the following criteria were met:
1.Space for all mandibular incisors to line up straight with either orthodontic brackets or clear aligners
2.Sufficient intercanine width for maxillary incisors to line up straight
3.Subjective improvement in sleep quality and daytime fatigue as assessed by the PSQ
4.Objective improvement in airway volume and cross section and/or AHI from HSAT
Data analysis and monitoringSample size estimateWith a power of 80%, a confidence level of 95%, alpha (possibility of Type I error) of 0.05, and an assumed improvement of 50%, it was estimated that approximately 40 participants would provide statistically significant results. At least 50 participants were needed to be enrolled in the study to allow up to 20% (N = 10) dropouts.
Data analysisThis analysis was conducted by pairing pretreatment measurements with posttreatment measurements at 3 months, 6 months, and final testing, which could be at 6, 12, 18, or 24 months. Paired t-tests were used to analyze pre- and posttreatment data for all coprimary and secondary endpoints. A linear mixed-effects model for repeated measures (MMRM) was used to analyze data for endpoints where intermediate timepoints were collected (intermolar width and SRBD subscale of the PSQ). Two separate models were constructed, one with intermolar width as dependent variable, and the other with SRBD subscale of the PSQ as dependent variable, each with fixed effects of time, age, gender, height, and weight. Missing data were imputed using expectation-maximization (EM) algorithms, with the exception of missing CBCT data from one site that did not conduct these scans on their five participants. Pearson correlations were obtained for the posttreatment-pretreatment difference scores for all endpoints and (1) participant age at pretreatment visit and (2) participant estimates of number of hours of use per 24-h period (averaged across visits). SPSS (IBM SPSS Statistics, Version 29) was used for all statistical analyses.
Data monitoringEach dental site securely uploaded the data to an independent third party who monitored the study and conducted the data analyses. The sponsor was blinded to the results and the study dentists and physicians were blinded from each other, although they did collectively attend training and protocol review.
Comments (0)