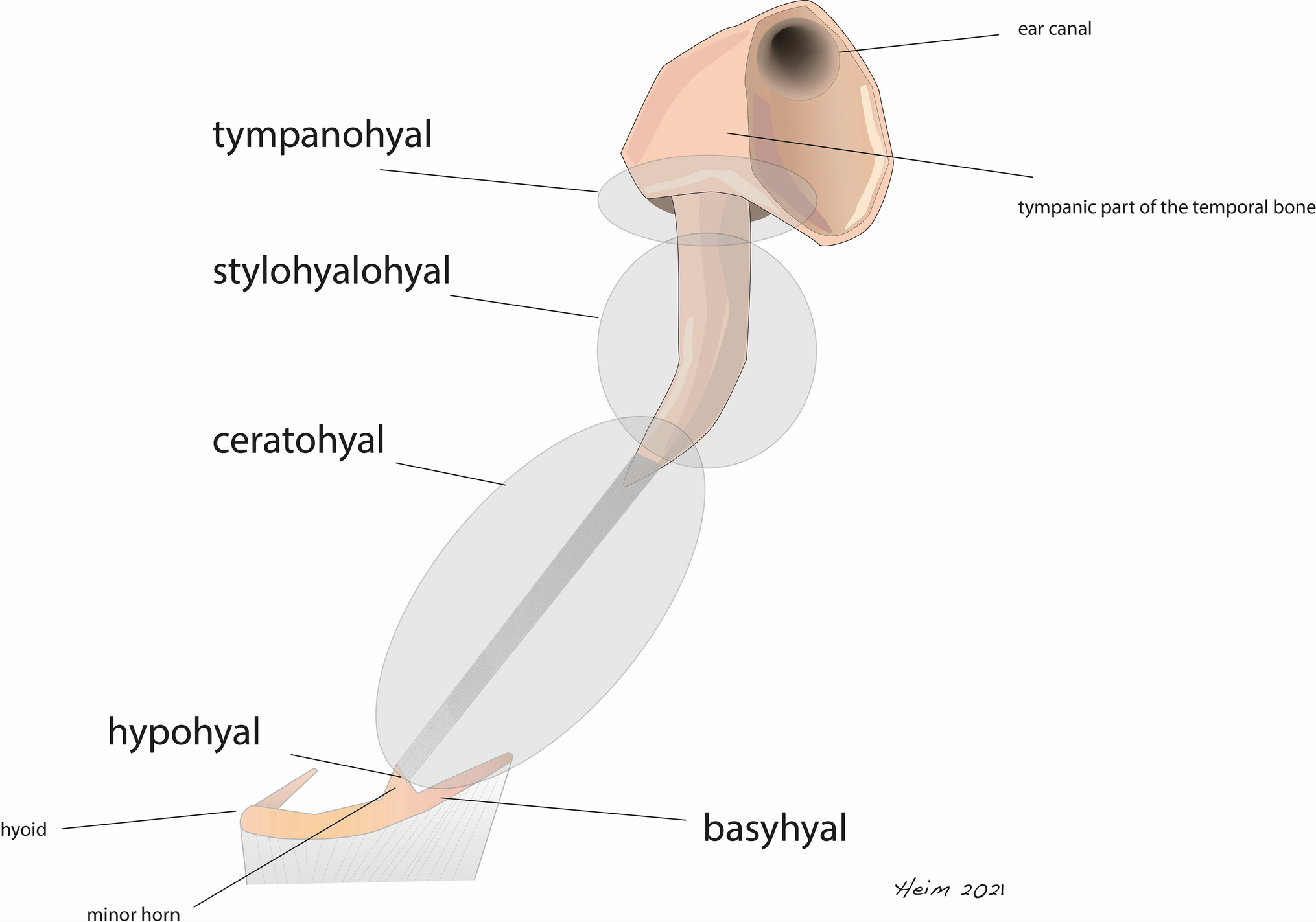
Our study revealed histological findings of enlarged styloid processes (SP) and ossified stylohyoid ligaments (SHL) causing Eagle syndrome. Currently, there is still discord about which anatomical structure, arising from the Reicherts cartilage, defines the origin of the single parts of the stylohyoid chain. Lenegele and Dhem suggest that small styloids emerge only from the tympanohyal part, while at the same time the stylohyal and ceratohyal part degenerate into the ligament. Further, they claim that in large styloids, the stylohyal part evolves into bone tissue until the age of eight [5]. Revilla and Stuyt assert that the SP mainly emerges from the stylohyal component and the tympanohyal part contributes only to the base of the SP [3]. In a recent study, we determined that two different anatomical variants cause Eagle syndrome [15]. Type I describes an enlarged SP. Type II describes the ossification of parts of the SHL. To the best of our knowledge, this differentiation is not considered in the literature of histological investigations on Eagle syndrome. We could not identify clear indicators of whether the SHL or the SP primarily originates from the tympanohyal or stylohyal component. However, the anatomical shape, the osseous ultrastructure, and the density of the cancellous bone showed only small differences between the groups.
In all tips of the SP and the distal parts of the ossified SHL, we found ligament insertion sites. The tip of the SP or likewise the most distal part of the ossified SHL plays an important role in the growth pattern of the structure. We found fibrous cartilage as well as hyaline cartilage caps in most of the specimens. Earlier studies reported about cartilaginous caps, while a recent histological investigation of ten cases found none of these caps and no evidence of enchondral ossification [18]. We found numerous cartilage caps with signs of calcified cartilage tissues and tidemarks as a sign for enchondral ossification. Lengele and Dhem [6] already mentioned this process as a possible cause for growth in an early paper. Nevertheless, Jeyaraj [18] hypothesized that traction forces and mechanical stress may induce metaplasia in mesenchymal components of the SHL and pluripotent periosteal cells, leading to the elongation of the SP. We assume that osteogenesis is additionally emanating from the fibrous cartilage tissue at the tip of the SP and distal part of the SHL. Likewise, Kim et al. investigated positive staining for HSP-70 and HO-1 in ten samples of elongated SPs. HO-1 is known for a downregulation of osteoclasts and upregulation of osteogenous differentiation. Dense staining was shown in the apical periosteal tissue. HSP-70 is a marker for bone apposition. Summarizing our findings, we believe that both groups of cartilaginous tissue play a role in the growth of SP and ossification of SHL.
In all but one case of type II specimens and two-thirds of type I specimens we discovered cartilage islets. Most of these islets showed enchondral ossification. Previous studies suggested that the cartilage islets are remnants of the Reichert’s cartilage and have the potential for enchondral ossification and subsequently for growth of the styloid or ossification of the SHL [19]. In our study, we were able to confirm this theory by showing clear ossification from hyaline islets.
The SHL has the potential for ossification processes [20]. Historically, but also in recent literature tonsillectomy is considered as a predisposing factor [21]. Further, trauma in the head and neck area is discussed to be a risk factor for ossification processes in the SHL [22]. Recently, researchers discovered an association between root canal treatment and ossification of the SHL, with a stronger correlation than tonsillectomy, age and trauma [23]. However, in three cases of our study, we found signs for osteogeneses in the ligament. The reason for the rare finding in only three cases may be the absence of ligament tissue in almost all of our specimens. Nevertheless, evidence for ossification within ligament tissue could be shown.
Ectopic calcification of soft tissue is known as inappropriate biomineralization [24]. Fibroblasts and osteoblasts are almost indistinguishable by gene expression profiles. Further, there are no specific genes expressed by osteoblasts that indicate biomineralization. Moreover, osteoblasts can be seen as sophisticated fibroblasts, which have the ability to form a mineralized extracellular matrix when exposed to a sufficient environment and stimulus [25].
Based on the micro-CT findings in our latest study [15], we expected an increased mineralization of type I bone tissue compared to type II. Since type I tissue originates from the skull base and type II bone emerges from newly formed bone in the ligament. The comparability of mineralization processes in both group is limited by the rather small number of specimens. However, the mean overall mineralization of bone tissue was higher in type I styloids compared to type II ossified ligaments. Since we discovered rather soft bone tissue within the ligaments during surgery of symptomatic type II cases, we suppose that early stages of ligament ossification have the potential to be responsible for severe symptoms. Surgery may be then performed in an early stage of ossification and mineralization which might be the reason for decreased mineralization processes of the type II specimens in comparison with type I styloids.
The overall bone structures within the two types were rather similar. Both types showed lamellar bone (Table 1). Even though subperiosteal bone apposition could not be determined in every case, we consider it to be an important growth mechanism for the thickening of the SP. In earlier studies, Lengele and Dhem observed peristyloid calcified tissues that could be followed from the distal part, down to the tip of the SP. These phenomena could be detected in short and long styloids [6]. In the present study, the subperiosteal apposition could be observed in most of the cases. Frequently, an intermediate stadium of fibrous cartilage forming into bone tissue could be noted. One case even showed an osteoma-like bone apposition (Fig. 4d).
Table 1 Listing of all specimens including the patients’ age and sex, as well as histological characteristics related to bone metabolismThe present study has some limitations. Due to the limited number of specimens, the results of the semiquantitative evaluation are not fully representative. Further, the bone samples showed a wide diversity within the structure which made it difficult to define regions of interest. Some of the samples may have been incomplete which did not allow to evaluate the tip, ligament or other structures of every sample for comparison. Other histological characteristics showed an anatomically wide distribution within the bone sample.
Despite the limited number of cases, certain peculiarities were observed that can be distinguished between the histologically differentiable type I and type II. Surgically, operating on type II cases was more challenging. Since the ossified ligament was often significantly more mobile in the neck and frequently adhered to the soft tissues, the surgeries took, on average, one-third longer. The duration of symptoms prior to surgery was highly heterogeneous, ranging from 3 weeks to 12 years. The average pain intensity across all cases and symptoms showed no significant difference between the two groups. However, it became evident that tinnitus and ear noises occurred only in type I cases which we explain through the fact that the styloid attached to the skull base in type I has the ability to irritate the middle ear and inner ear. Similarly, foreign body sensations were more common in the type I group. Improvements in symptoms after surgery were comparable in both groups; however, ear problems persisted the longest which may be due to the fact that central nervous disorders often show a memory-like effect even when the focus is erased.




Comments (0)