
Remember me



Radiotherapy for head and neck cancer frequently causes tissue damage within the direct radiation portals, affecting the oral cavity, salivary glands, and taste buds. Oral mucositis is the most common and severe complication of cytotoxic cancer treatment, sometimes even life-threatening. In patients receiving radiation therapy for head and neck cancers, it is the primary dose-limiting side effect, often disrupting treatment or causing premature termination. These interruptions can hinder effective tumour control and negatively impact patient survival outcomes [11].
Coconut oil, also known as copra oil, is an edible oil extracted from the pulp or kernel of mature, dried coconuts harvested from the coconut palm (Cocos nucifera). It is predominantly composed of saturated fatty acids (SFA), which make up approximately 90% of its total composition. Mucositis, a major side effect of radiation therapy, has been effectively mitigated through the use of various medications and substances, including coconut oil.
To date, no technique has completely prevented mucositis; however, many have proven effective in reducing its severity and associated discomfort. Coconut oil, renowned for its numerous health benefits—including antimicrobial, anti-inflammatory, antifungal, anticancer properties, and its role in wound healing—has been widely recognized by researchers over the past few decades for its therapeutic potential. Due to these favourable attributes, coconut oil shows promise in preventing mucositis, alleviating discomfort, reducing trismus, and combating fungal infections during radiation therapy.
The findings of this study align with those of Ogbolu et al., who demonstrated that at a minimum inhibitory concentration (MIC) of 25%, coconut oil exhibited 100% sensitivity in Candida species susceptibility, compared to 88% sensitivity for fluconazole. They also noted that fluconazole was more fungistatic than fungicidal, even at higher doses, while in-vitro tests showed some fungicidal activity of capric acid and lauric acid, evidenced by decreased infectivity titre [13].
Similarly, a study by Shino et al. investigated the antibacterial efficacy of probiotics, ketoconazole, coconut oil, and chlorhexidine against Candida albicans isolated from young patients with early childhood caries. The study highlighted coconut oil's antifungal effectiveness, which was found to be comparable to ketoconazole and superior to probiotics in its advanced antifungal activity against Candida albicans [14]. Additionally, Bergsson et al. demonstrated the susceptibility of Candida albicans to various fatty acids and their 1-monoglycerides [15].
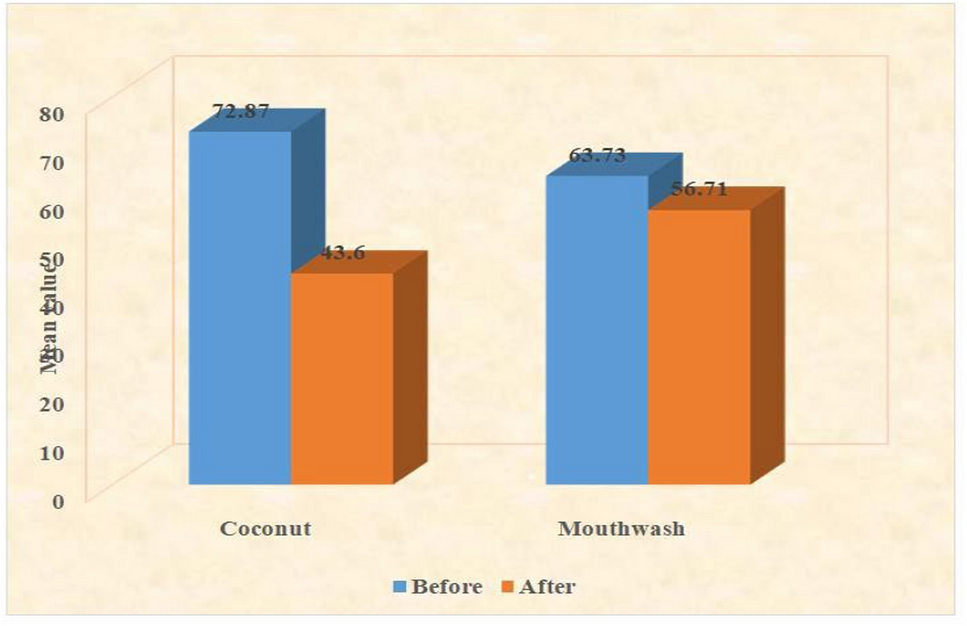
In our study, we observed a significant reduction in the number of Candida colonies following coconut oil pulling (p < 0.001, highly significant) (Fig. 3). Notably, mucositis onset was delayed in the test group compared to the control group. By the end of the first week of radiation therapy (1000 cGy), half of the control group had developed grade 1 mucositis, progressing to grade 2 by the end of the second week (2000 cGy). In contrast, no mucositis was observed in the test group during the same period.
Fig. 3
SDA plate showing candida colony culture before and after study
By the third week (3000 cGy), all control group subjects had mucositis, with 75% advancing to grade 3 by the fourth week (4000 cGy). Conversely, mucositis in the test group became apparent only by the sixth week (6000 cGy), with only two-thirds of patients reaching grade 2 by the end of the treatment. Remarkably, several subjects in the test group did not develop mucositis at any point during the therapy (p = 0.001). The peak severity of mucositis was significantly lower in the test group compared to the control group.
These results are consistent with the findings of Mustafa et al., who observed that the treatment group receiving zinc sulfate had a median radiation therapy (RT) dose of 3600 cGy (3½ weeks) at the onset of mucositis, compared to 2000 cGy (2 weeks) in the control group. In their study, mucositis first appeared at 1800 cGy during the second week, peaked at the start of the third week, and reached its maximum severity by the middle of the fourth week before gradually declining. The difference in mean mucositis scores between the treatment and control groups became statistically significant after 2400 cGy (2½ weeks) and remained significant up to six weeks post-treatment [17].
Our findings also corroborated those of Karbassi et al., who demonstrated that patients in the experimental group treated with propolis experienced delayed mucositis onset and significantly reduced severity compared to the placebo group. The experimental group exhibited milder symptoms, with overall moderate mucositis severity [16].
During oil pulling, lauric acid in coconut oil reacts with sodium hydroxide present in saliva to form sodium laureate, which likely plays a key role in its anti-inflammatory effects by preventing bacterial adhesion to soft tissues. Additionally, the antioxidant properties of lauric acid help protect the oral mucosa from infection and inflammation [17]. Asokan et al. further highlighted that the emulsification of oil begins within five minutes of initiating oil pulling therapy, which contributes to its therapeutic benefits [18].
The mechanism of coconut oil pulling therapy, as explained by Peedikayil et al., involves the mechanical shear forces applied during swishing, which emulsify the oil and significantly increase its surface area. This process enables the oil to coat the tissue surfaces, reducing bacterial co-aggregation [17].
Our study demonstrated a significant delay in the onset of mucositis in the coconut oil group (3rd week, 19th–23rd day) compared to the benzydamine mouthwash group (1st week, 4th–7th day) (p < 0.001). The severity of mucositis was also markedly lower in the coconut oil group, with 66.1% of participants experiencing only grade 1 mucositis (p < 0.001). Notably, some participants in the coconut oil group did not develop mucositis at all throughout radiotherapy (p = 0.001). Furthermore, coconut oil improved mucositis grades during subsequent weeks (24.1%, p < 0.001).
Additionally, significant improvements were observed in associated complications of radiation-induced oral mucositis such as pain (p < 0.001) and trismus Table 7 (p = 0.006) along with overall enhancement in quality of life (p = 0.009).
To date, no single intervention has been able to fully prevent or treat oral mucositis. Importantly, no prior studies in the literature have reported on the use of coconut oil pulling as an anti-inflammatory agent for radiation-induced oral mucositis. In our study, none of the participants reported any side effects associated with coconut oil use.
Table 7 Number of patients showing the onset of trismus in both the groups
Comments (0)