
Remember me

From 1990 to 2021, the global number of lip and oral cavity cancer incidence, deaths, and DALYs increased by 142.18%, 113.94%, and 100.06%, respectively. ASIR exhibited an increasing trend (AAPC: 0.44%), whereas ASMR and age-standardized DALYs rate showed slight declines (AAPC: − 0.03% and − 0.07%, respectively) (Tables 1, 2, 3).
Table 1 Number of cases and ASR of lip and oral cavity cancer incidence in 1990 and 2021 at global, SDI, and GBD regional level, with AAPC from 1990 to 2021Table 2 Number of cases and ASR of lip and oral cavity cancer mortality in 1990 and 2021 at global, SDI, and GBD regional level, with AAPC from 1990 to 2021Table 3 Number of cases and ASR of DALYs of lip and oral cavity cancer in 1990 and 2021 at global, SDI, and GBD regional level, with AAPC from 1990 to 2021Regionally, South Asia reported the highest ASIR, ASMR, and age-standardized DALYs rate, whereas Oceania had the lowest number of cases. The lowest ASIR was observed in Western Sub-Saharan Africa, whereas North Africa and Middle East recorded the lowest ASMR and age-standardized DALYs rate. The largest increase in ASIR occurred in East Asia, whereas Western Sub-Saharan Africa had the highest growth in ASMR and age-standardized DALYs rate. In contrast, the greatest decline in ASIR was observed in High-income North America, whereas Western Europe experienced the largest reductions in ASMR and age-standardized DALYs rate (Tables 1, 2, 3).
At the national level, India had the highest incidence, mortality, and DALYs burden in 2021, followed by China, whereas Tokelau had the lowest. The highest ASIR, ASMR, and age-standardized DALYs rate values were reported in Palau, whereas the lowest were found in São Tomé and Príncipe. From 1990 to 2021, Cabo Verde showed the most significant increase in ASIR, ASMR, and age-standardized DALYs rate, whereas Kuwait experienced the largest decline (Supplementary Tables 1, 2, and 3).
According to the SDI classification, the highest incidence in 2021 was observed in the middle SDI group, whereas mortality and DALYs were the highest in the low-middle SDI group. The lowest values across all three measures were recorded in the low-SDI group. Notably, ASIR was highest in the low-middle SDI, whereas ASMR and age-standardized DALYs rate were highest in the same SDI category. The middle SDI showed the largest increase in ASIR, while the low-middle SDI showed the greatest increase in ASMR and age-standardized DALYs rate. Conversely, the high SDI group exhibited the largest decline in all three metrics (Tables 1, 2, 3).
The residual analysis confirmed an excellent model fit, with average relative error values consistently < 10.00% (Supplementary Table 4). An example of the detailed model selection process was provided in Supplementary Table 5. Additionally, the results of sensitivity analyses showed similar trends when modeling data lower/upper bounds (Supplementary Tables 6). These results further demonstrated the reliability and stability of trend analysis methods.
Sex- and age-specific trendsBetween 1990 and 2021, the incidence, death, and DALYs of lip and oral cavity cancer have increased in both men and women. While men consistently exhibited higher ASIR, ASMR, and age-standardized DALYs rate than women, the increase in ASIR was more pronounced in women (AAPC: 0.78%) than in men (AAPC: 0.26%) (Table 1). Meanwhile, ASMR and age-standardized DALYs rate declined in men (AAPC: − 0.18% and − 0.22%, respectively) but increased in women (AAPC: 0.26% and 0.24%, respectively) (Tables 2, 3).
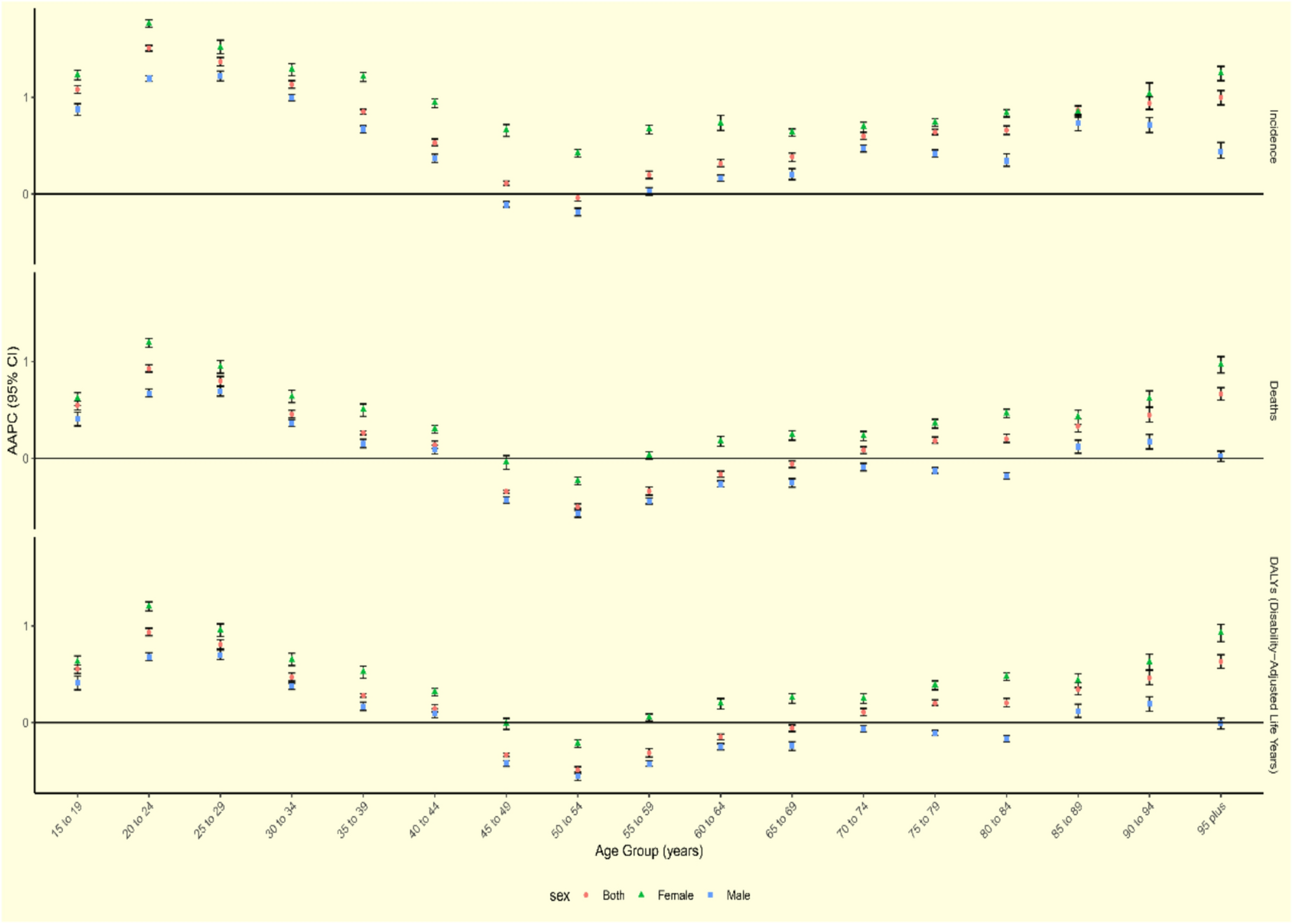
Age-wise, the highest number of incident and fatal cases was observed in the 65–69 age group, while DALYs peaked in the 55–59 age group (Supplementary Fig. 1). The highest ASIR was found in individuals aged 90–94 years, whereas ASMR and age-standardized DALYs rate peaked in individuals aged 95 years and above. Between 1990 and 2021, the ASIR, ASMR, and age-standardized DALYs rate increased in individuals younger than 44 years, with the highest AAPC in the 20–24 age group. The ASIR increased in all age subgroups except for the 50–54 age group, while ASMR and age-standardized DALYs rate declined significantly in individuals aged 45–69 years, particularly in the 50–54 age group (Fig. 1; Supplementary Table 7).
Fig. 1
The global AAPC of incidence, deaths, and DALYs for lip and oral cavity cancer from 1990 to 2021 by age group and sex. Abbreviations: AAPC, average annual percentage change; DALYs, disability-adjusted life-years
Men had higher incidence and mortality rates in most age groups (Supplementary Fig. 1). However, in the 15–19, 20–24, 90–94, and 95-plus age subgroups, women had more cases and higher ASIR, ASMR, and age-standardized DALYs rate. Additionally, women in all age groups demonstrated a steeper upward trend in ASIR, ASMR, and age-standardized DALYs rate than men, with the highest AAPC observed in women aged 20–24 years and men aged 25–29 years (Fig. 1; Supplementary Table 7).
Association between SDI and lip and oral cavity cancer burdenA significant positive correlation was observed between SDI and ASIR (ρ = 0.44, P < 0.001), indicating that regions with higher SDI had higher incidence rates of lip and oral cavity cancer (Supplementary Fig. 2). However, the correlations between the SDI and ASMR (ρ = − 0.08, P = 0.261) and between the SDI and age-standardized DALYs rate (ρ = − 0.08, P = 0.266) were not statistically significant.
Decomposition analysisBetween 1990 and 2021, DALYs due to lip and oral cavity cancer have increased globally, with the highest growth occurring in the low-middle SDI group (Supplementary Fig. 3). Population growth was the primary driver, contributing 70.75% to the increase in DALYs, followed by aging (32.85%), whereas epidemiological change contributed -3.59%, indicating a reduction in DALYs due to improved healthcare (Supplementary Table 8). The high SDI group showed the most significant impact of aging (97.50%) and population growth (107.95%), whereas the low-middle SDI group showed the largest epidemiological change effect (7.72%). The epidemiological shift had a net negative effect on DALYs in the high SDI (− 105.45%) and high-middle SDI (− 69.76%) groups. When stratified by sex, the demographic effects were similar, but the epidemiological effects were globally negative for men and positive for women (Supplementary Fig. 3).
Cross-country inequality analysisThe burden of lip and oral cavity cancer exhibited increasing disparities across SDI levels from 1990 to 2021 (Fig. 2). The age-standardized DALYs rate was disproportionately concentrated in low-SDI countries. The concentration index, reflecting relative health inequality, increased from − 0.19 (95% CI − 0.25 to − 0.13) in 1990 to − 0.23 (95% CI − 0.30 to − 0.15) in 2021, demonstrating a worsening trend in global health disparities.
Fig. 2
SDI-related health inequality concentration curves for the age-standardized DALYs rate of lip and oral cavity cancer globally, comparing 1990 and 2021. Abbreviations: DALYs, disability-adjusted life-years; SDI, socio-demographic index
Risk factor contributionsBetween 1990 and 2021, the contribution of smoking and alcohol use to lip and oral cavity cancer deaths and DALYs declined, whereas tobacco chewing showed a slight increase (Supplementary Fig. 4). In 2021, smoking has remained the leading risk factor for lip and oral cavity cancer, although its impact has decreased globally. Smoking contributed the most in the high-middle SDI regions, alcohol use in the high SDI regions, and chewing tobacco in the low-middle SDI regions. In the high and high-middle SDI groups, chewing tobacco accounted for less than 3% of lip and oral cavity cancer deaths and DALYs, whereas its impact was substantially higher in the other SDI categories.
Regionally, smoking contributed the most to the lip and oral cavity cancer burden in East Asia, alcohol use in Central Europe, and tobacco chewing in South Asia. The impact of smoking declined across most regions except East Asia, while alcohol use remained the predominant risk factor in Australasia, Central Europe, Southern Latin America, and Western Europe. Chewing tobacco contributed to less than 10% of the burden in most regions, except in South and Southeast Asia (Supplementary Fig. 4).
Age-stratified analysis showed that the contribution of all risk factors increased the most in the 25–29 age group from 1990 to 2021, whereas the largest decline was observed in the 50–54 age group (Fig. 3; Supplementary Tables 9 and 10). The impact of smoking decreased in both sexes, with a more significant decline observed in women. Alcohol use declined in most female age groups, with the sharpest reduction observed in those aged 50–54 years. In contrast, alcohol use increased among men aged < 39 years, peaking in the 25–29 age group. The impact of chewing tobacco increased, particularly among women aged 55 years and older, whereas in men, the highest increase was observed in the 40–44 age group. Temporal trends in risk factor contributions to lip and oral cavity cancer ASMR and age-standardized DALYs rate across age groups were presented in Supplementary Fig. 5–8 and 9–12, respectively.
Fig. 3
AAPC of lip and oral cavity cancer ASMR (A) and age-standardized DALYs rate (B) attributable to each risk factor from 1990 to 2021 by age group and sex. Abbreviations: AAPC, average annual percent change; ASMR, age-standardized mortality rate; DALYs, disability-adjusted life-years
Comments (0)