
Remember me


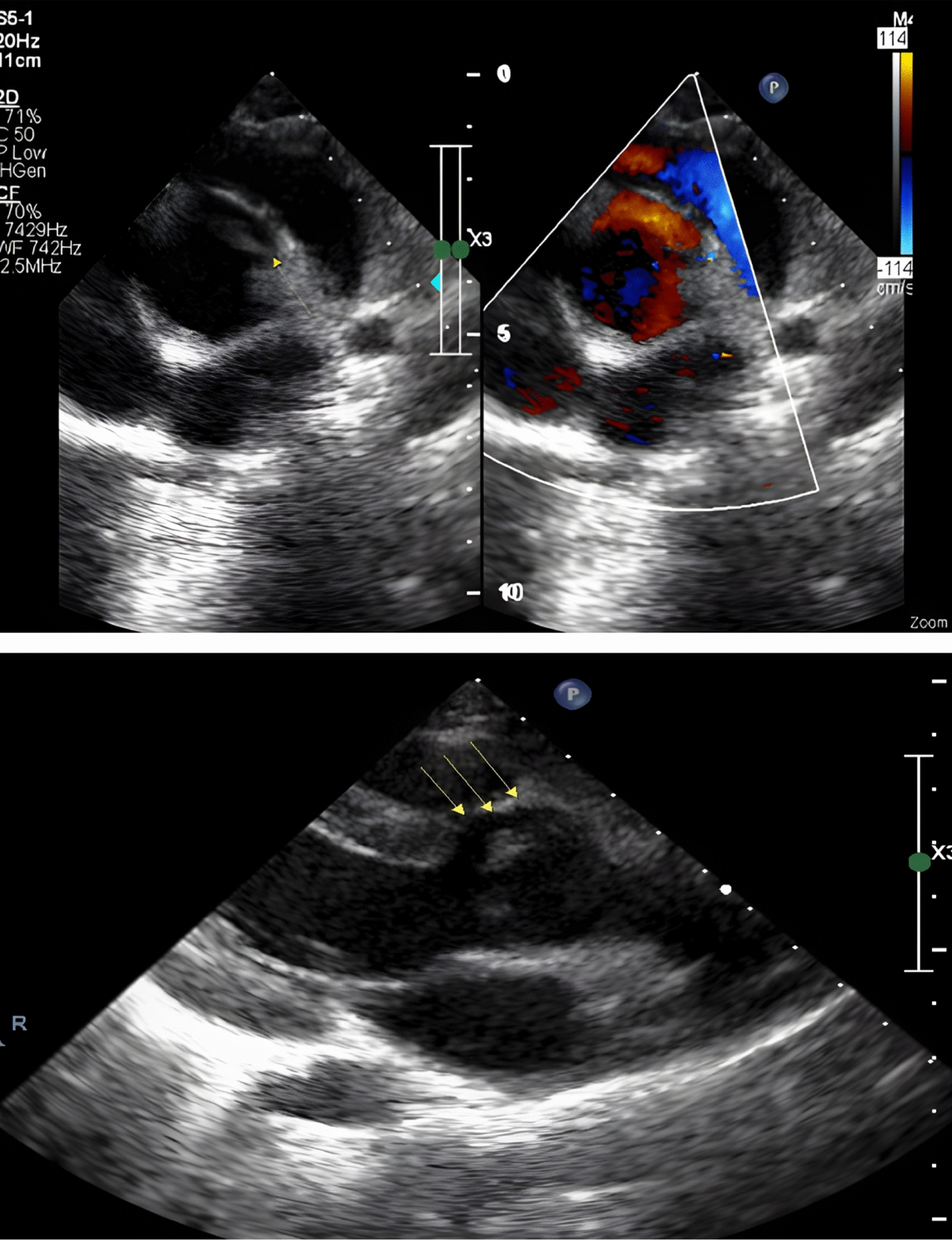




Many challenges have limited the 2D echocardiographic assessment of the TV, given the non-planar geometry of the valve orifice, the lack of simultaneous visualization of the three leaflets in a single plane, and the wide range of leaflet numbers. Recently, 3DE has been considered the gold standard for imaging the TV and planning procedural interventions in regurgitant valves [4, 5]. Rheumatic tricuspid valves exhibit unique characteristics that help differentiate them from other primary valve diseases, such as carcinoid valves, which often display commissural sparing features. The first two cases showed mildly thickened leaflets by 2DE. However, more key features were clearly recognized on 3D images, especially commissural fusion at one commissure (anteroposterior commissure in case 1) and three commissures (anteroposterior, anteroseptal, and posteroseptal commissures as in case 2), giving a morphologically bi-leaflet valve. Moreover, thickened, fused, and shortened chordae tendinae were described. Interestingly, the third case shared some morphological findings, such as thickened leaflets with a reduced excursion, with rheumatic valves. Still, the presence of open, non-fused commissures was a clear-cut point that precluded the rheumatic diagnosis. Thus, the diagnosis of carcinoid tricuspid valve was reached in concordance with the clinical and imaging workup. One more advantage is the accurate planimetry of the orifice area, first, by acquiring a high frame rate, single beat, or multi-beat 3D volume of the tricuspid valve, including part of the septum and the aortic valve; second, by selecting the multiplanar reconstruction option and adjusting the slicing planes at the tips of the leaflets and perpendicular to the orifice in the two orthogonal planes in diastole and last, short-axis images of the valve orifice will be created in the third image with the ability of direct area tracing. This feature was extremely useful in the three cases to identify the stenotic degree while being load independent in the presence of hemodynamically significant tricuspid regurgitation or atrial fibrillation (differences between 2 and 3DE are highlighted in Fig. 4). A useful practical workflow of 3DE assessment of TV involves several key steps:
Fig. 4
Central illustration highlighting the differences between 2 and 3DE in TV stenosis assessment
1. Patient Positioning and Probe Selection: Use standard echocardiographic windows (apical, parasternal, subcostal) for transthoracic 3DE or midesophageal positions for transesophageal 3DE. Optimize patient position to minimize lung artifact and maximize right heart visualization [3, 6].
2. Data Acquisition: Acquire a full-volume 3D dataset using ECG gating, typically over 4–7 cardiac cycles to balance spatial and temporal resolution. For focused assessment, use a narrow-angled, single-beat 3D zoom mode to improve resolution of the TV apparatus. The American Society of Echocardiography recommends optimizing 2D images before 3D acquisition to ensure high-quality datasets [3, 6].
3. Orientation and Display: Reconstruct the TV in an en face view from the right atrial or right ventricular perspective. The septal leaflet should be positioned at the 6 o’clock position for consistency, as recommended by the American Society of Echocardiography and the European Association of Echocardiography [3, 6].
4. Multiplanar Reconstruction (MPR): Use MPR to align orthogonal planes through the annulus and leaflets, allowing precise measurement of annular dimensions, leaflet morphology, and coaptation. This is essential for accurate quantification, as 2D measurements systematically underestimate annular size and do not account for nonplanarity [3, 6].
5. Quantitative Measurements: Measure annular area, perimeter, major and minor axes, and leaflet tethering. Dedicated 3D software that accounts for annular nonplanarity is preferred for accuracy. For regurgitation, use color Doppler 3DE to localize jets and planimeter the vena contracta area [3, 6].
Comments (0)