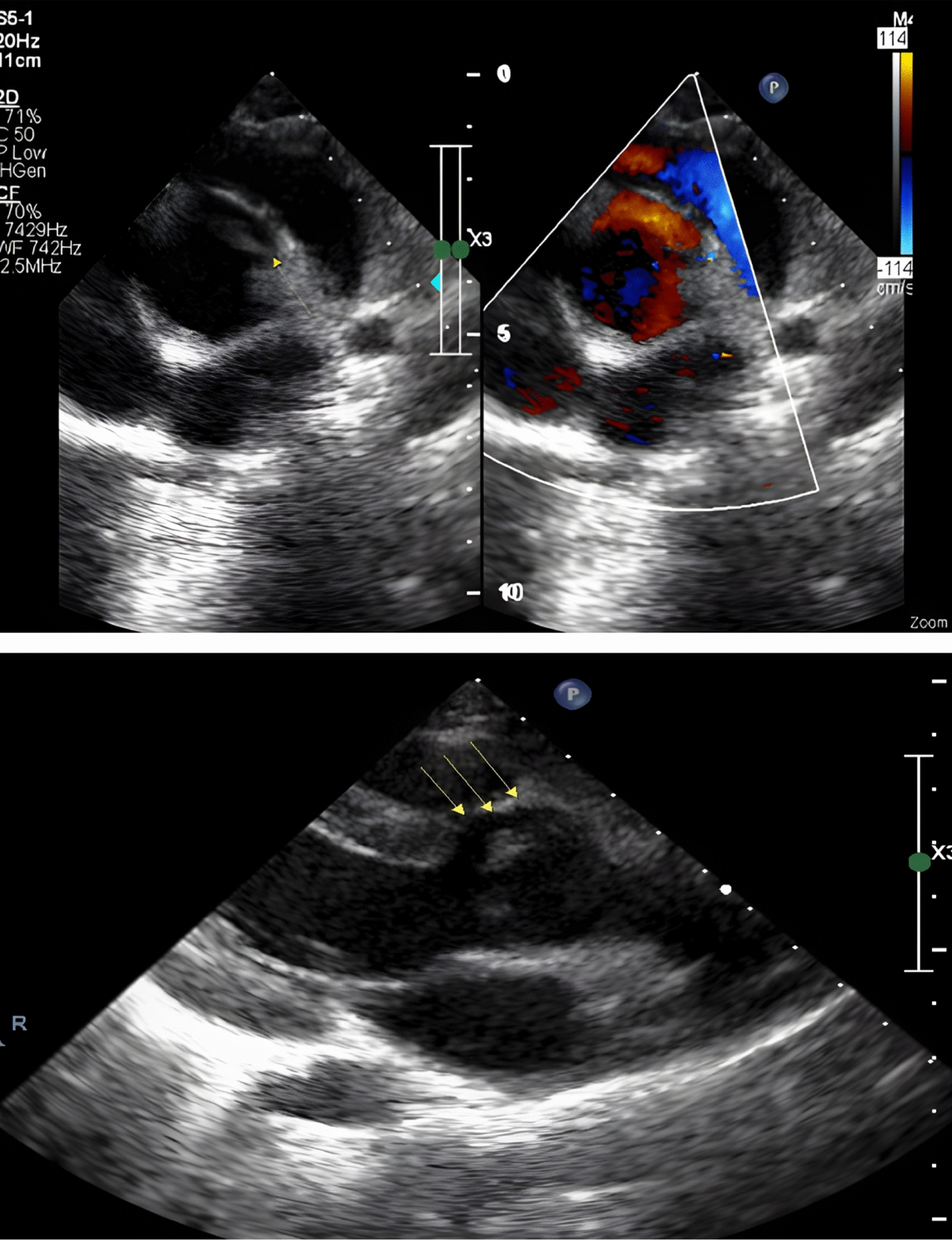
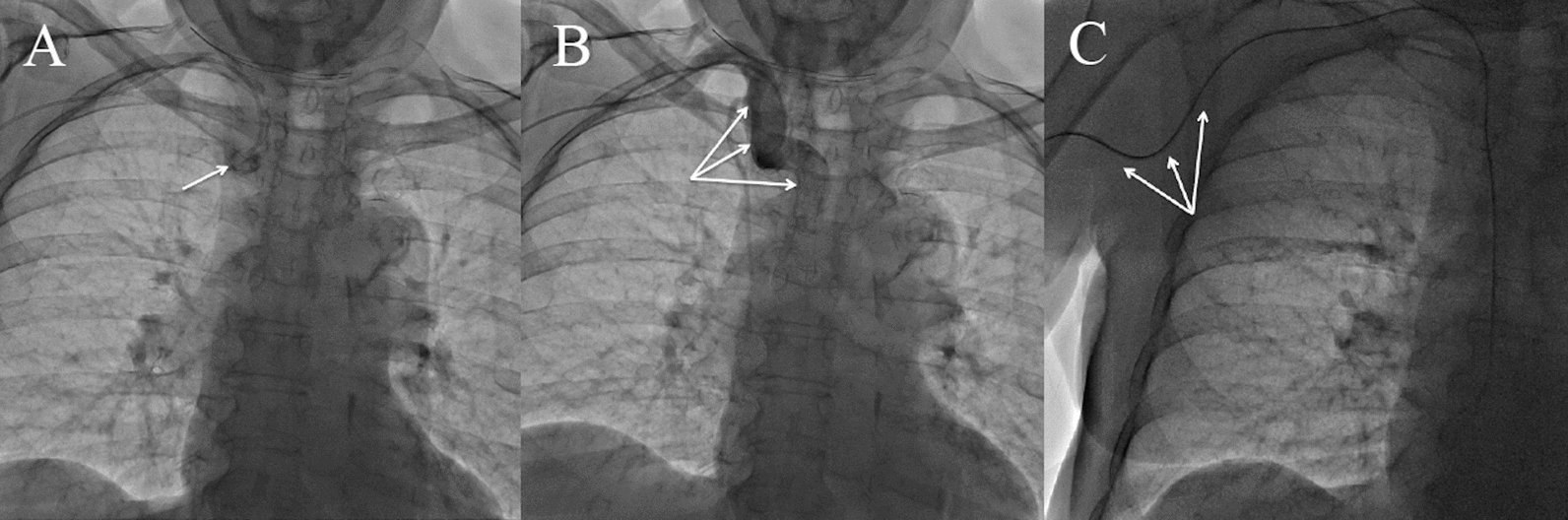
A tunnel between the ascending aorta and the left ventricle is a rare congenital heart disease more commonly observed in males and located above the coronary sinus. In our case, although no specific cause for this disease has been identified, various etiologies have been proposed, ranging from congenital to acquired. However, prenatal diagnosis has ruled out the acquired theory. Proximal coronary anomalies, such as an intra-tunnel coronary ostium or coronary ostial atresia, have been documented. Additionally, aortic valve anomalies, including bicuspid aortic valve and dysplasia, have been reported in previous case studies. Pulmonary valve stenosis with subvalvular pulmonary stenosis due to a tunnel has also been reported [1]. ALVT results in steal from the aorta to the ventricle and continuous murmur during diastole without impacting systemic circulation during systole. This is because during systole the left ventricle contracts and generates pressure exceeding that of the aorta, making systolic flow across the tunnel unlikely and thus not producing a murmur [5]. However, none of these conditions except for the murmur were found in our case. Regarding the diagnosis of this disease, various methods have been mentioned, including chest X-ray, transesophageal echocardiography (TEE), echocardiography, and magnetic resonance imaging (MRI). Previous studies have suggested that a high degree of aortic regurgitation in newborns may indicate the possible presence of this tunnel. In our study, this symptom was also present and the child had severe aortic regurgitation. Regarding the treatment of this condition, it has been stated that surgical intervention is recommended upon diagnosis, as delaying the procedure may lead to deterioration in the patient’s clinical condition. Two surgical methods for tunnel closure, using sutures or a patch, have been previously reported. The former, suture closure, has been associated with aortic valve distortion. In our case, we opted for the patch closure technique. Previous studies have reported cases of ALVT closure using device closure, but in our case, given the tunnel’s entry point in the right aortic sinus, specifically between the right coronary ostium and left and right aortic commissures, device closure posed significant risks [6]. In a study conducted over 11 years at a medical center involving 7 patients diagnosed with ALVT, results revealed that two patients died during follow-up, four underwent surgical tunnel closure, and one patient underwent a Bentall procedure. In this study, it was reported that 5 out of 7 patients were female. Among these, five cases were type 2, one case was type 3, and one case was type 4. Of this number, 6 cases demonstrated a tunnel ostium located above the right coronary artery, and one case showed an ostium located above the non-coronary cusp. In our case as well, the tunnel ostium was located above the right coronary artery. Aortic regurgitation was reported in only two cases from this group, both in older individuals (aged 11 and 45 years), whereas in our case, despite the patient being only 5 years old, severe aortic regurgitation was reported. This disease is classified into four types: Type 1 (a slit-like ostium at the aortic root without valve distortion), Type 2 (large extracardiac aneurysm), Type 3 (intracardiac aneurysm of the septal tunnel, with or without right ventricular outflow tract obstruction), and Type 4 (a combination of Types 2 and 3). Based on previous studies, most cases were of Type 2, whereas in our case, it was Type 3 [1]. This is significant because, in Type 1, given the anatomical conditions, it is possible to close the tunnel using a device [2]. Spontaneous closure of ALVT has been observed only in very rare, asymptomatic patients with a small tunnel. Surgery should be performed early in life and the technique chosen should be such that it stabilizes the aortic annulus without deformity and also closes the aorto-ventricular window (7).







Comments (0)