Over the past two decades, Neurofilament light chain has garnered significant attention as a potential biomarker for monitoring disease progression in MS.
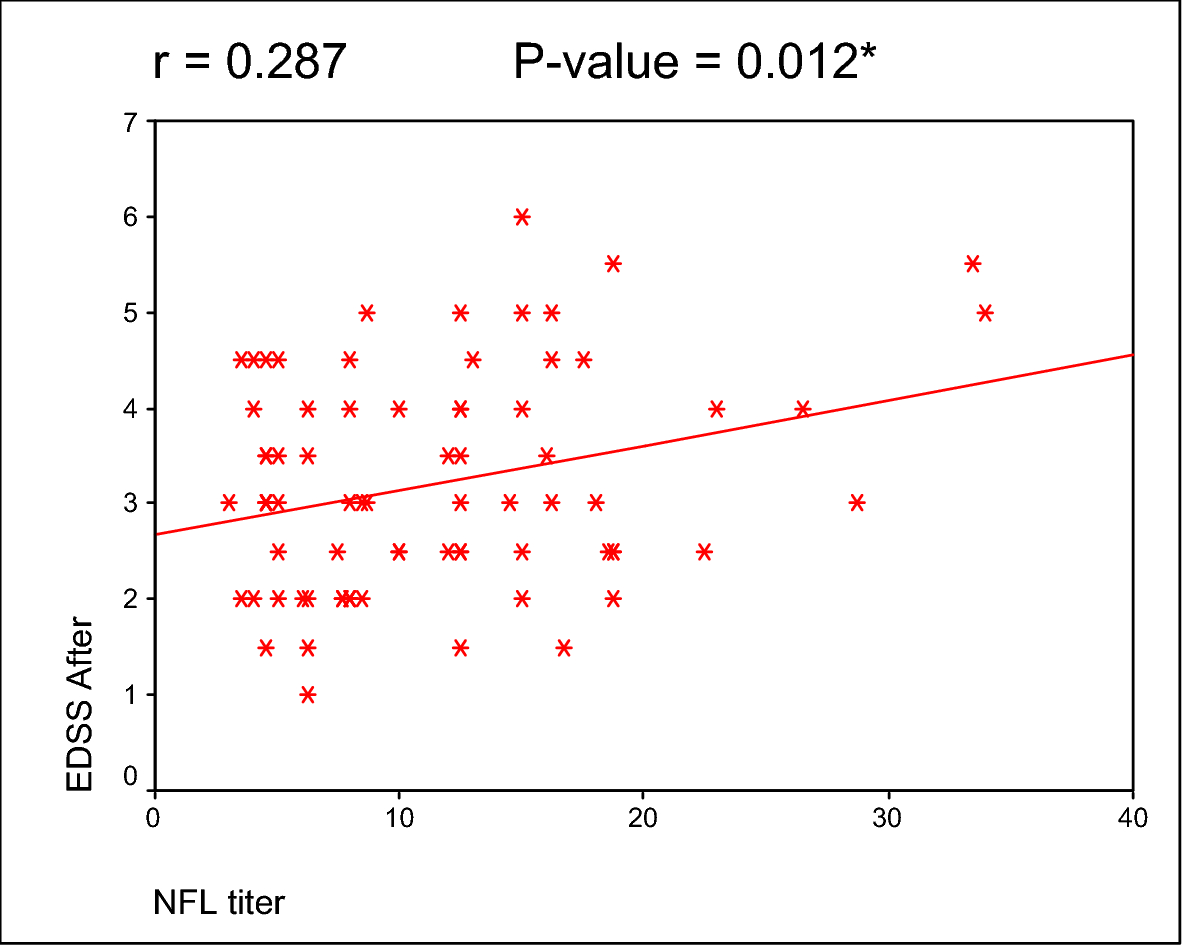
Numerous studies have demonstrated that elevated sNfL concentrations correlate with higher neurological disability scores [4, 13]. For instance, a longitudinal cohort study revealed that higher sNfL levels during periods of active inflammation were associated with greater disability progression [14], a finding that aligns with our results showing a significant correlation between sNfL levels and EDSS progression at one-year follow-up (p = 0.012). Conversely, Brune et al. found that by analyzing the association of sNfL concentrations with single components of disease worsening, patients with high sNfL at baseline had no increased risk of EDSS progression in the follow-up period, highlighting potential variability across studies [10].
Our study also found no statistically significant correlation between sNfL levels and either patient gender or age, which aligns with previous observations indicating no gender differences in sNfL concentrations. However, while our study did not find an association with age, earlier research has reported a positive correlation between sNfL levels and age [10,11,12].
Our study further established a significant association between sNfL levels and radiological markers of disease burden, including the presence of more than 10 T2 brain lesions (p < 0.001) and lesions in the periventricular and spinal cord regions (p = 0.023 and p < 0.001, respectively). Similarly, Brune et al. reported that higher baseline sNfL concentrations in RRMS patients were strongly linked to increased T2 lesion counts. These findings are supported by prior research showing progressively higher sNfL levels with increasing T2 lesion burden in both the brain and spinal cord [15].
Finally, a recent Egyptian cohort study investigated sNfL as a biomarker for neurodegeneration in MS patients without clinical or gadolinium-enhanced MRI evidence of disease activity. The study concluded that sNfL levels were significantly elevated in MS patients compared to healthy controls (p < 0.001). Furthermore, the EDSS score was identified as the sole independent predictor of sNfL levels (β = 0.415, p = 0.002) [16].
The significant correlation between sNfL levels and radiological markers, such as the presence of periventricular and spinal cord lesions, as well as a high T2 lesion burden, highlights its potential as a complementary tool to MRI. These findings align with prior research showing that sNfL reliably reflects inflammatory and neurodegenerative processes visible on imaging. The clinical implications of our findings are profound and highlight the prognostic significance of sNfL in MS. Elevated levels of sNfL are linked to increased loss of brain and spinal cord volume, as well as the progression of long-term disability. One practical implication of these findings is that sNfL could serve as a marker for treatment stratification, helping to identify patients who might benefit from moving to more aggressive therapies aimed at reducing further neuronal damage.
This study provides valuable insights into the role of sNfL as a biomarker in MS, but several limitations should be noted. First, it was a single-center study with a small, homogeneous cohort of Egyptian patients, which may limit the applicability of the findings to more diverse populations. Larger, multicenter studies are needed to confirm the results. Second, while sNfL levels were measured at baseline and correlated with clinical and radiological parameters over a one-year follow-up, longer-term studies are necessary to assess its prognostic value over extended periods and its potential in predicting transitions to progressive MS subtypes. Third, causality cannot be inferred from the observed correlations between sNfL, disability, and lesion burden. Interventional studies exploring treatment impacts on sNfL levels and clinical outcomes would strengthen the understanding of its clinical utility. Lastly, the absence of serial sNfL measurements limits the assessment of changes over time-related to disease activity. Future studies should include longitudinal sampling for a clearer picture.



Comments (0)