
Remember me


A 60-year-old man was admitted to the hospital with a complaint of “lower back pain accompanied by pain and numbness in both lower limbs for 5 months.” He has a history of hypertension and has been on long-term antihypertensive medication for blood pressure control. The patient also reported long-standing numbness and discomfort in the head and both upper limbs. He had previously been diagnosed with cervical spondylosis at another hospital, but this condition had not received adequate attention. Upon admission, cranial MRI revealed no abnormalities. Thoracic CT demonstrated: 1. pulmonary emphysema; 2. scattered pulmonary nodules bilaterally; 3. aortic and coronary artery calcification. Lumbar CT showed: 1. degenerative changes of the lumbar spine, including disc bulging from L2/3 to L5/S1 and disc protrusion at L5/S1; 2. bilateral sacroiliac joint degeneration. Admission diagnoses: 1. lumbar spinal stenosis; 2. hypertension, high-risk group. The patient is scheduled to undergo elective posterior lumbar laminectomy, decompression, and spinal canal enlargement surgery under general anesthesia.
The patient came into the operating room at 12:10 p.m. on the day of surgery. Standard monitoring was applied, revealing a noninvasive blood pressure (NBP) of 138/81 mmHg, oxygen saturation (SpO2) of 95%, and heart rate (HR) of 58 bpm. After 3 min of pre-oxygenation via face mask for denitrogenation, general anesthesia induction was initiated with sequential intravenous administration of dexamethasone 10 mg, sufentanil 20 µg, propofol 100 mg, and cisatracurium besylate 10 mg. Once the patient achieved a Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) score ≤ 1 and a bispectral index (BIS) of 50–60, an ID 7.0 reinforced endotracheal tube was inserted orally to a depth of 23 cm.
Mechanical ventilation parameters were set to the pressure control–volume guaranteed (PCV-VG) mode, with a tidal volume (Vt) of 450 mL, respiratory rate of 13 bpm, inspired oxygen concentration of 80%, and peak airway pressure ranging from 12 to 18 cmH2O. General anesthesia was maintained with sevoflurane (titrated to a minimal anesthetic concentration (MAC) of 0.8–1.2 and a BIS value of 40–60), remifentanil, and cisatracurium besylate as needed. Simultaneously, an arterial catheter was inserted into the left radial artery for invasive blood pressure monitoring.
Surgical procedures commenced at 13:55. During the laminectomy, an accidental tear of the dura mater was observed, resulting in cerebrospinal fluid (CSF) leakage. A sterile gauze pad was immediately placed over the area, but within approximately 3 min, the gauze was completely soaked, likely due to CSF infiltration, with an estimated volume of about 100 mL. The surgeon applied gelatin sponge compression, and after observing for 10 min, no further CSF leakage was noted, allowing the surgery to proceed.
The procedure lasted approximately 5 h and 30 min. The patient’s vital signs remained stable throughout, with an estimated blood loss of 500 mL and a urine output of 2500 mL. The patient received 3050 mL of crystalloid solution, 500 mL of hydroxyethyl starch, and 400 mL of autologous blood reinfusion.
Fifteen minutes after the surgery, spontaneous respiration returned, but the patient could not be awakened. Given stable blood pressure and heart rate, the anesthesiologist opted for continued monitoring without intervention. After around 2 h with no signs of consciousness, both pupils were observed to be equal in size but slightly larger than normal. An arterial blood gas analysis was performed, yielding the following results: pH 7.37, pCO₂ 40 mmHg, pO₂ 230 mmHg, Na⁺ 145 mmol/L, K⁺ 3.4 mmol/L, Ca2⁺ 1.14 mmol/L, lactate 1.1 mmol/L, Hct 31%, hemoglobin concentration 98 g/L, HCO₃− 23.1 mmol/L. No significant abnormalities were found, so vital signs monitoring was continued.
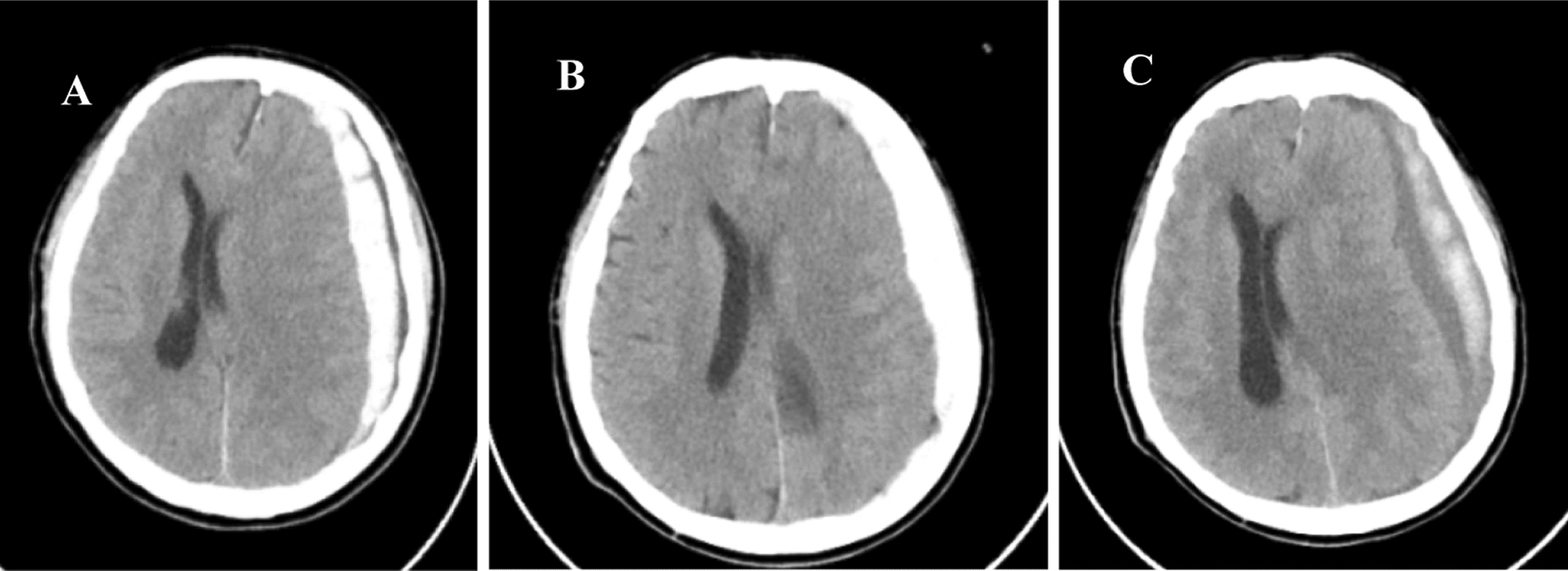
After approximately 90 min, the patient began coughing and was unable to tolerate the endotracheal tube, prompting extubation, although consciousness had not returned. A neurosurgical consultation was urgently requested, and by then, the left pupil had dilated, raising concerns of intracranial hemorrhage. The patient was transported under close monitoring to the imaging department for a cranial CT scan, which revealed an extensive left hemispheric subdural hematoma and a suspected brain herniation; the estimated blood loss was approximately 75 mL (Fig. 1A).
Figure. 1
A Noncontrast computed tomography (CT) of the brain demonstrates an extensive left hemispheric subdural hematoma and a suspected brain herniation; B follow-up CT of the brain demonstrating a slight reduction in midline shift compared to the initial scan; C the CT scan revealed a large subacute subdural hematoma in the left cerebral hemisphere, now larger than before, with progression of subfalcine and uncal herniation
An emergency craniotomy for hematoma evacuation was advised. However, the patient’s family declined the surgery due to financial constraints. The patient was subsequently transferred to the intensive care unit (ICU) for advanced life-support treatment, including noninvasive mechanical ventilation, dehydration therapy to reduce intracranial pressure, anti-infection therapy, nutritional support, and continuous monitoring. Unfortunately, these measures showed limited effectiveness.
On postoperative day 7, a repeat cranial CT scan showed a slight reduction in midline shift compared to the initial scan (Fig. 1B). The surgical option was again discussed with the family, but they continued to resist. A CT scan on postoperative day 23 revealed a large subacute subdural hematoma in the left cerebral hemisphere, now larger than before, with progression of subfalcine and uncal herniation (Fig. 1C). As the family still declined surgical intervention, standard supportive treatment continued.
On postoperative day 45, the patient’s family requested discharge against medical advice. The patient passed away 7 days after discharge.
Comments (0)