Surgical robots, known for their precision, stable operation, reproducibility, fatigue resistance, and immunity to radiation, have been increasingly applied in orthopaedics. These systems assist orthopaedic surgeons in performing various procedures with greater accuracy, particularly in trauma, spine, joint, sports medicine, and orthopaedic oncology surgeries [16].
Fracture reduction robots face significant challenges, as they must withstand substantial loads during procedures and require ample space to execute reduction tasks effectively [17]. As a result, many of these robotic systems remain in the prototype phase. For instance, the University of Regensburg in Germany developed a femoral shaft fracture reduction robot, RepoRobo, based on the Staubli RX130 industrial robot [18]. Similarly, Hannover Medical School, in collaboration with Braunschweig University of Technology, created a reduction robot system utilizing master-slave control with force and position feedback [19]. Additionally, the University of Tokyo and Osaka University in Japan developed FRAC-Robo, a traction robot that aids femoral fracture reduction by applying traction via a boot connected to the patient’s foot [20]. Another example is RAFS, an image-guided robotic system proposed by Aston University for the percutaneous treatment of intra-articular knee fractures [21].
In China, several institutions have made strides in robotic fracture reduction. For example, Tzu Chi Hospital in Taiwan, in collaboration with National Taipei University and Chang Gung University, developed a robotic system that controls knee flexion, applies separate traction to the thigh and calf, and rotates the foot [22]. Beihang University has created a vision-based, teleoperated system that uses preoperative CT scans for high-precision minimally invasive fracture reduction [23]. Additionally, Beijing Jishuitan Hospital, in partnership with Tianzhi Navigation Technology Co., Ltd., developed a six-degree-of-freedom fracture reduction robot based on master-slave control [24].
Our research team has also developed an intelligent fracture reduction robot system, which has completed successful clinical trials involving 92 pelvic fracture cases. Building on this success, we are continuing to enhance this system for the closed reduction of long bones. Crucially, the robotic strategy for pelvic fracture reduction leverages mirroring technology. In this approach, the intact hemipelvis serves as a virtual template, guiding the fractured side towards a predefined mirrored anatomical position. Within our system, this mirroring protocol essentially defines the anatomical endpoint for pelvic reduction [17]. Conversely, the robotic reduction protocol for long bone fractures, exemplified by the femur, employs a statistical shape model (SSM). This model, constructed from a database of normative anatomical variations, calculates the optimal reduction by comparing the current fracture configuration against statistical norms, thereby directing the reduction towards an idealized, statistically derived anatomical alignment. The endpoint for long bone reduction is determined by the convergence of fracture fragments towards the position defined by the SSM. Furthermore, the inherent biomechanical and anatomical challenges encountered in these two regions are markedly different [25]. Pelvic reduction frequently encounters difficulties with locking between fracture fragments [26]. In contrast, the primary challenge in long bone reduction lies in achieving and maintaining a stable reduction and purchase at the proximal and distal fracture fragments. This often necessitates meticulous control over the robotic arm’s force application and spatial manipulation within the typically constrained surgical workspace to effectively control and align the bone segments during the reduction maneuver. These fundamental distinctions are elaborated upon in greater detail within the Discussion section.
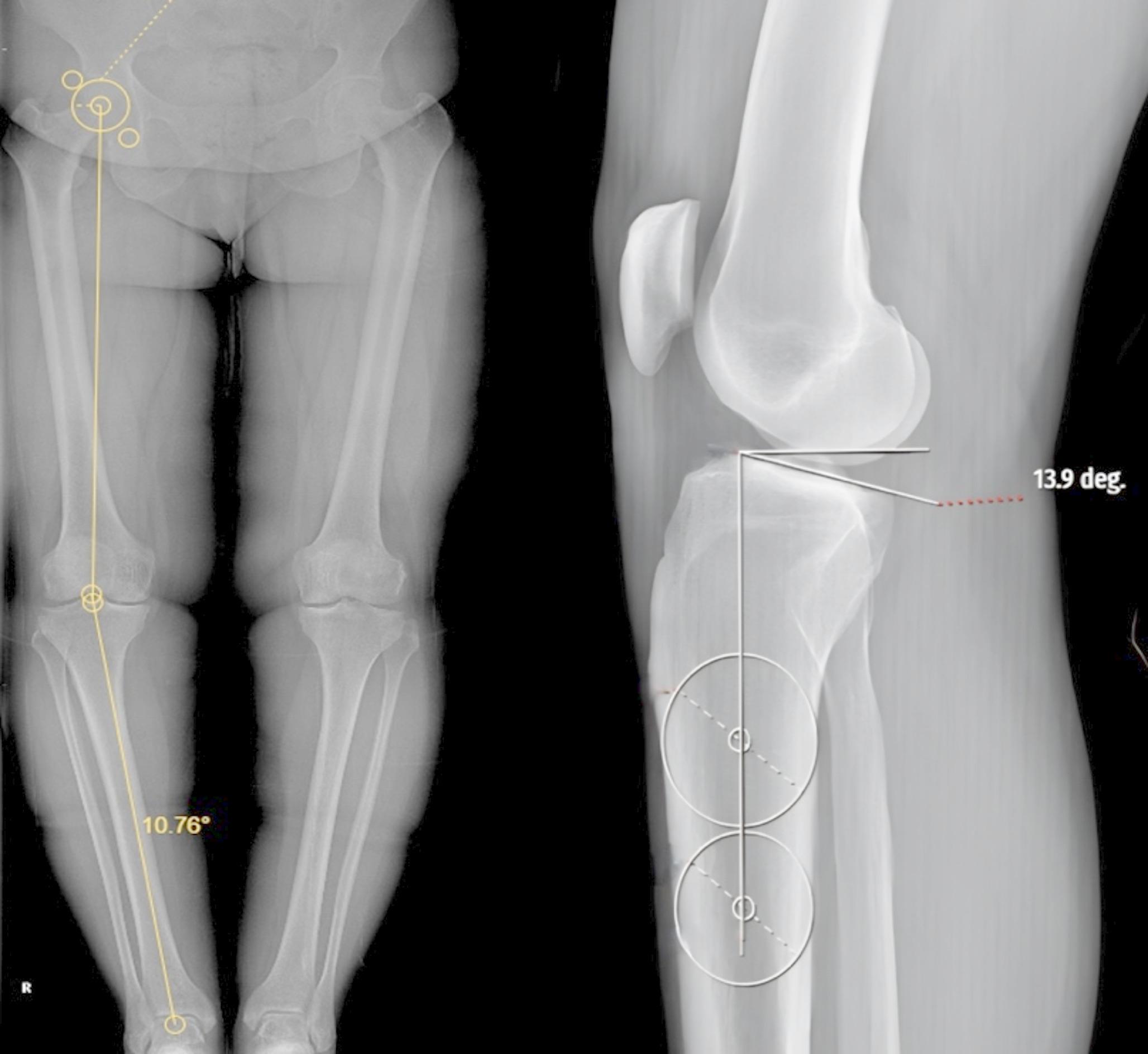
In our approach, we import CT data into the robotic software, where it undergoes 3D reconstruction to plan the reduction of the distal ends of the fracture using the mirror principle and the engagement relationships of the fracture surfaces. This ensures that no collisions or obstructions occur during the reduction process. Additionally, we have observed significant morphological differences in the bilateral femurs of the same patient, such as variations in the anteversion angle and femoral length. These findings align with those of Dimitris Dimitriou et al. [27].
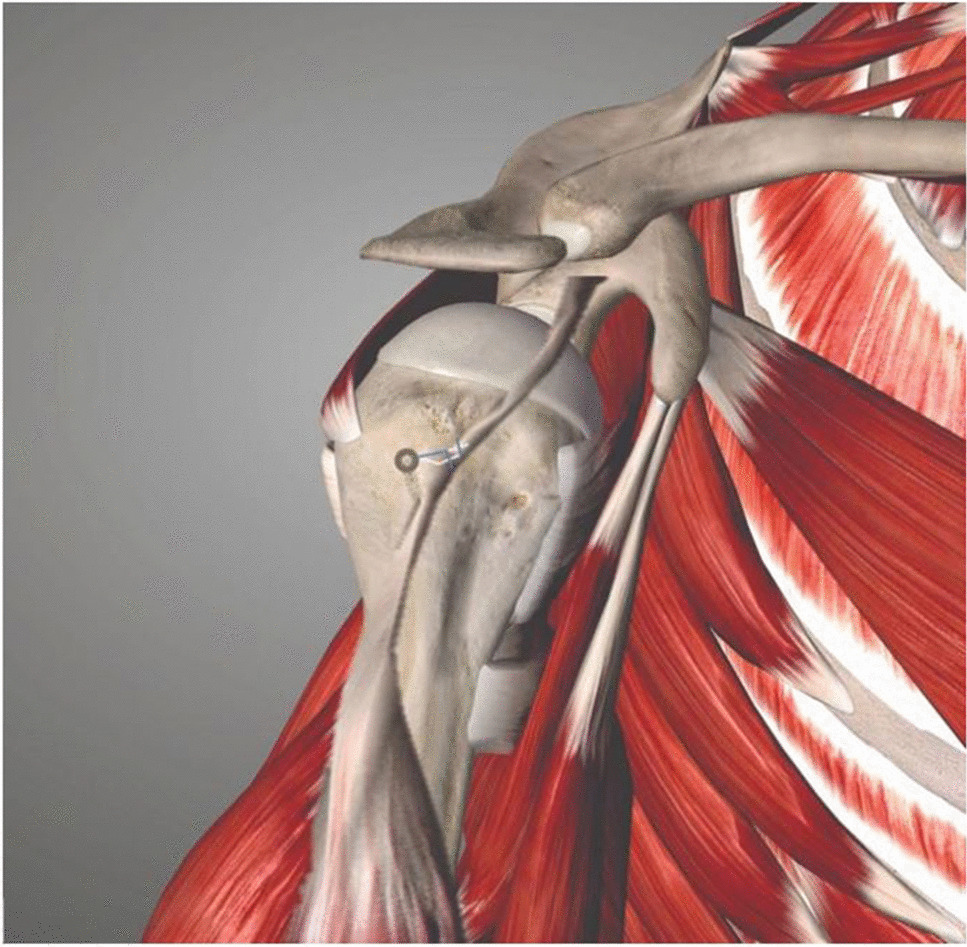
For the fracture reduction procedure, we employed a method where the fixation pin is inserted until it penetrates the cortex, ensuring it does not interfere with subsequent proximal reaming or the insertion of locking screws. This approach maintains stability for the tracker without affecting the planned surgical steps. The distal tracker is placed on the lateral femoral condyle, near the edge of the patella, to avoid entering the patellofemoral joint. This positioning minimizes the likelihood of interference during the insertion of the intramedullary nail. Following tracker placement, we conduct a cone-beam CT (CBCT) scan and integrate the scanned data into the robotic system for registration.
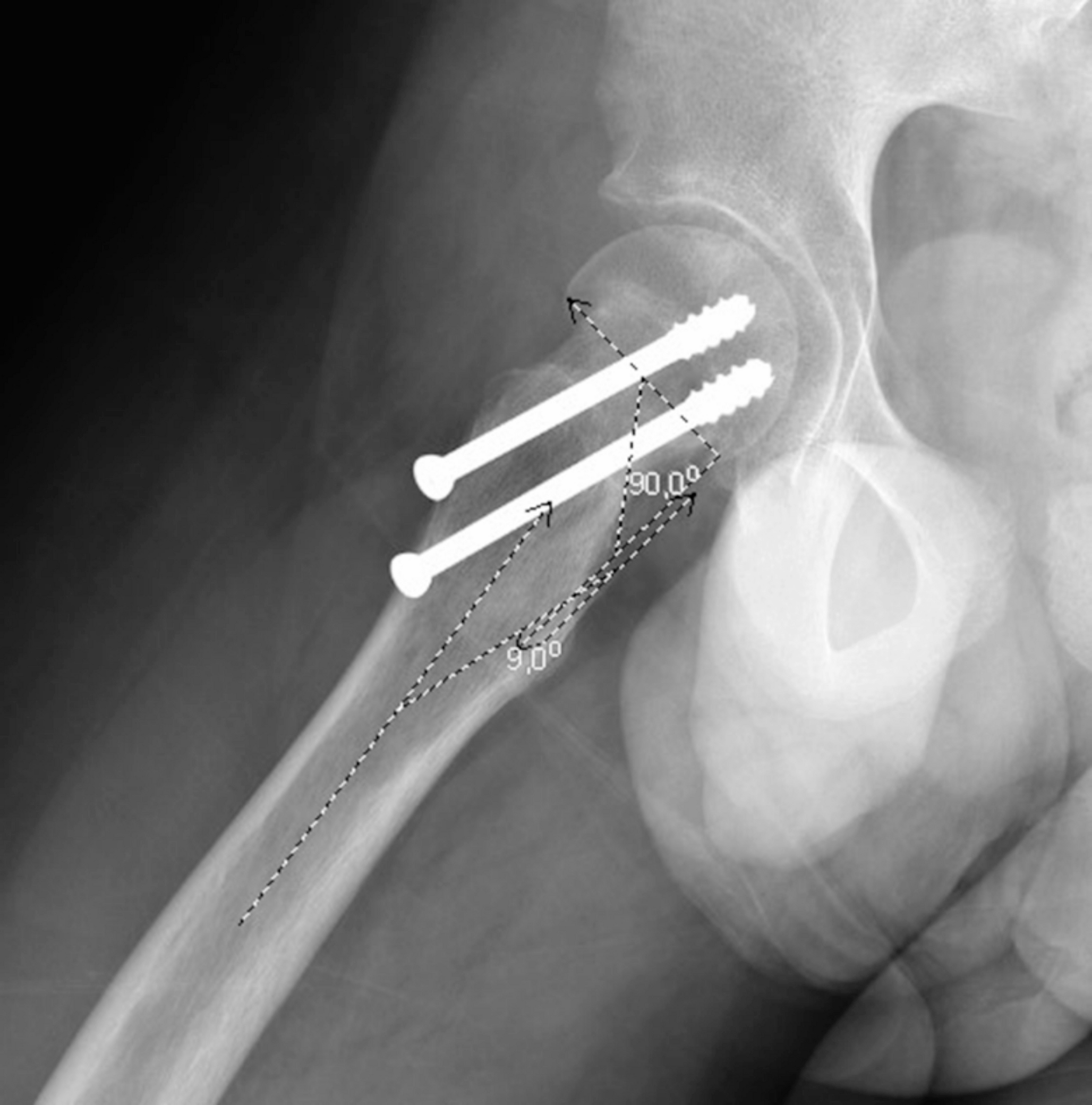
To ensure the alignment and orientation of the fracture reduction, we align the distal end with the proximal end, accounting for potential sagittal plane adjustments. The software calculates the position of the proximal end in advance, providing the surgeon with guidance to prevent collisions during the procedure. To hold the proximal end in place, a passive arm is attached near the patient’s head, locking the proximal femur in position. Once registration is complete, the holding pins are implanted at both ends of the fracture. For the proximal end, a holding pin is inserted from front to back, featuring a large threaded design to enhance stability. This pin is monitored in real-time to ensure it does not encroach upon the medullary cavity, ensuring that subsequent reaming and screw insertion proceed smoothly.
For the distal holding, two pins are connected to the robotic system via a three-pronged connector. One pin passes perpendicularly through the femoral condyles in the sagittal plane, positioned just above the femoral condyles to avoid interfering with the locking screws. The second pin is inserted similarly to the proximal holding pin. All pins are carefully monitored during insertion to avoid damage to intra-articular tissues, with the procedure being guided by the navigation drill.
Once both distal pins are connected, the robotic system performs the fracture reduction automatically, and fluoroscopy is used to verify the alignment. Unlike traditional methods, where an assistant must manually apply traction, our elastic traction device replaces this need. This device offers continuous, real-time adjustment of traction force during the reduction, providing more stable and efficient assistance throughout the procedure.
In summary, our intelligent fracture reduction robot system offers a highly precise, minimally invasive approach to femoral shaft fractures. The robotic arm, operating under real-time monitoring, effectively maintains the reduction position, providing advantages over traditional methods by reducing the need for intraoperative fluoroscopies.
Limitations
While this study demonstrates the feasibility of robot-assisted closed reduction for femoral shaft fractures, the small sample size limits the generalizability of the results. Larger trials are needed to confirm the effectiveness of this robotic system in clinical settings. Furthermore, while the system provides navigation and positioning for fracture reduction, its role in subsequent procedures, such as intramedullary nail placement, requires further investigation. Future studies should assess the accuracy and operability of these additional functions to validate their clinical utility.
Interpretation
This study explores the use of an intelligent surgical robotic system for femoral shaft fractures (Chinese Patent No.: 202110779036.4). The results show that the system can intelligently plan the reduction position, design the reduction path, and provide real-time 3D navigation during surgery. The robotic arm successfully completes the reduction as per the planned path, with the resulting reduction quality and accuracy surpassing conventional manual reduction techniques. Notably, the number of fluoroscopies required was significantly lower compared to traditional methods. As research progresses, we believe this intelligent fracture reduction system will offer a novel approach to the minimally invasive treatment of femoral shaft fractures and potentially other long bone fractures.




Comments (0)