Since acetabular column fracture fixation with lag screws was first described by Judet and Letournel in the 1960s, it has been increasingly preferred due to its advantages such as requiring less surgical exposure [30, 31]. The gold standard treatment for displaced acetabular fractures is open reduction and internal fixation (ORIF) [16]. However, percutaneous lag screw fixation is a minimally invasive option that can be applied in the treatment of non-displaced or minimally displaced acetabular column fractures [11, 14, 31, 32]. Furthermore, in acetabular fractures involving both columns, it is a common practice to first perform open reduction and internal fixation for one column, followed by reduction and lag screw fixation of the other column through the same surgical approach [14, 33, 34].
Numerous biomechanical studies have demonstrated that lag screw fixation of acetabular column fractures can provide stability comparable to that of plate-and-screw constructs [35,36,37,38].
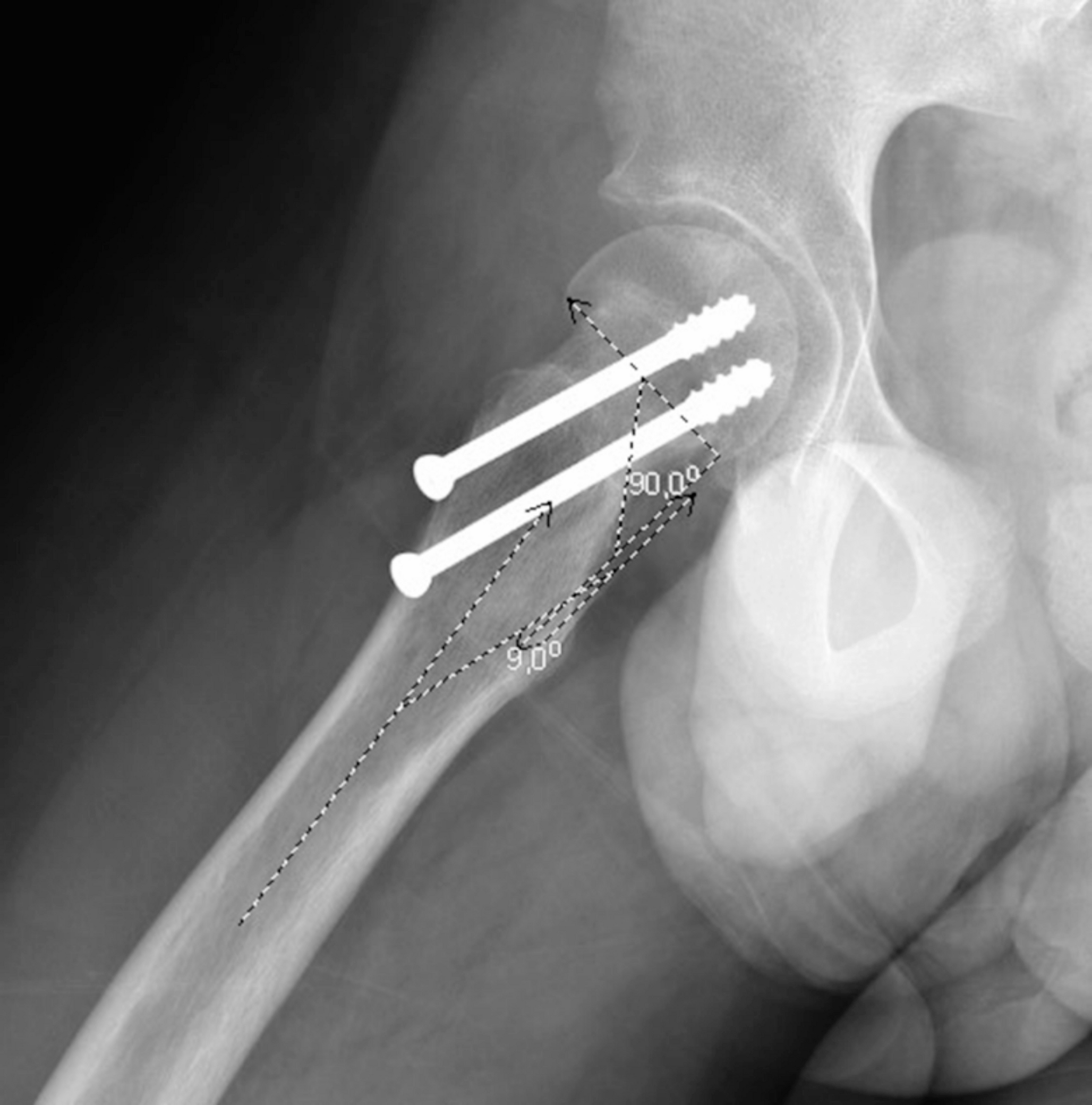
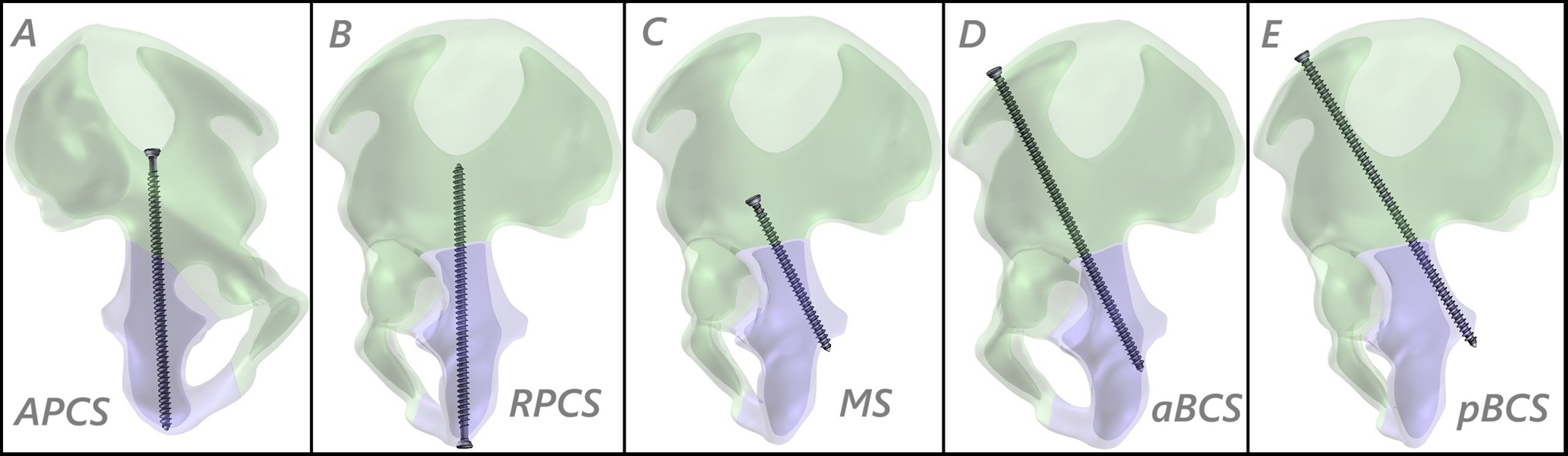
Various lag screw fixation techniques are available for the treatment of posterior column fractures of the acetabulum. The most commonly known is the antegrade posterior column screw, originally described by Judet and Letournel, which is inserted from the iliac fossa toward the posterior column [16]. Starr et al. later described a retrograde technique in which the screw is inserted percutaneously through the ischial tuberosity [32]. In 2001, Starr et al. also introduced another percutaneous technique involving the quadrilateral surface and posterior column, which they termed the “magic screw” [11]. More recently, Öztürk et al. described a new percutaneous fixation technique for posterior column fractures, termed the “Both Column Screw (BCS)” fixation technique [14, 15].
Numerous in vitro biomechanical studies and finite element analyses have compared the mechanical stability of different internal fixation models for various types of acetabular fractures. For instance, Şibar et al. conducted an in vitro biomechanical study comparing the stability of conventional cannulated screws, talon screws, and traditional plate-screw constructs for the fixation of acetabular posterior column fractures [36]. Wang et al. analyzed the efficacy of infra-acetabular screws (IS) in the fixation of posterior column fractures by comparing APCS, IS, traditional plate-screw techniques, and their combinations [38]. Similarly, Hinz et al. performed a biomechanical comparison of APCS and IS used as adjuncts to plate fixation in acetabular fractures involving the posterior column [39]. These examples reflect a growing body of literature evaluating and comparing the biomechanical performance of various implants and fixation techniques in acetabular fracture management [39,40,41].
However, there is no comprehensive study directly comparing lag screw techniques for the fixation of acetabular posterior column fractures. In our literature review, we found no studies other than the one by Zhang et al., which was published in Chinese, comparing lag screw fixation methods for acetabular posterior column fractures. Their study compared the Magic Screw, retrograde posterior column screw, single plate, and double plate fixation in the treatment of posterior column fractures [35].
To the best of our knowledge, this is the first biomechanical study to compare lag screw fixation techniques for acetabular posterior column fractures, encompassing both conventional methods such as APCS and RPCS, and innovative approaches such as the Magic Screw (MS) and Both Column Screw (BCS) techniques.
In this study, five different screw fixation techniques were compared based on five distinct biomechanical parameters under three common loading scenarios encountered in daily life: level walking, stair ascent, and stair descent.
Among these parameters, maximum stress within the screw (von Mises stress) reflects the magnitude of mechanical load exerted on the implant. High intramedullary screw stress increases the risk of approaching the elastic limit, potentially leading to implant fatigue or failure over time. In this context, the findings of our study demonstrated that the pBCS configuration exhibited the lowest intramedullary screw stress values across all loading scenarios. Similarly, the aBCS and MS models also showed comparably low stress levels. In contrast, the APCS model consistently recorded the highest screw stress under all loading conditions. These results suggest that the BCS configurations (aBCS and pBCS), as well as the Magic Screw, may offer a biomechanical advantage over conventional APCS and RPCS techniques in terms of long-term screw integrity.
Considering that the APCS and RPCS models exhibited similar biomechanical characteristics in our study, our findings—consistent with those of Zhang et al.—indicate that the Magic Screw demonstrates superior biomechanical performance compared to conventional screw fixation techniques (APCS and RPCS) [35].
Maximum stress within the bone represents the strain occurring in the cortical and cancellous bone surrounding the implant. Elevated bone stress may lead to increased micromotion at the implant–bone interface, cortical damage, or bone resorption. In our study, the lowest bone stress was observed in the MS configuration during level walking, while the pBCS configuration showed the lowest values during stair ascent and descent. Conversely, the highest bone stress was recorded in the RPCS model, followed by the APCS. These findings suggest that reducing peri-implant bone stress is critical for long-term stability, particularly in patients with osteoporotic bone structure. In this regard, the pBCS, aBCS, and MS configurations may offer biomechanical advantages over APCS and RPCS by potentially lowering the risk of bone resorption and implant loosening.
Total deformation reflects the structural change of the system under load and provides an indication of overall rigidity. Lower deformation values suggest that the fixation construct maintains its integrity and exhibits greater biomechanical stiffness. In this study, the lowest deformation was observed in the pBCS configuration under stair ascent and descent conditions, and in the MS model during level walking. A low total deformation value may indicate a level of stability that permits early weight-bearing, which could be particularly advantageous in elderly patients or those with concomitant injuries where early mobilization is critical. In contrast, the highest deformation values were observed in the APCS and RPCS models, indicating comparatively inferior performance in terms of construct rigidity.
Fracture gap and sliding distance are two key parameters that reflect micromotion between fracture fragments and indicate the degree of stability provided by the implant under load. In this study, the MS configuration exhibited the lowest values for both parameters during level walking, while the pBCS configuration showed the lowest values during stair ascent and descent. Similarly, the aBCS model also demonstrated low gap and sliding values. These findings suggest that the MS and BCS (aBCS and pBCS) screw techniques may provide superior fracture stability by minimizing interfragmentary motion. In contrast, the highest gap and sliding distances were observed in the APCS model, followed by the RPCS model. These results indicate that the APCS and RPCS configurations may be more prone to micromotion and therefore represent biomechanically less favourable options for fragment stabilization.
When all parameters are considered together, the pBCS technique consistently demonstrated the most balanced and rigid construct in terms of overall stability. The MS and aBCS models also exhibited similarly high levels of biomechanical performance. In contrast, the conventional APCS and RPCS configurations showed higher stress levels, increased deformation, and greater fracture surface motion under all loading conditions, indicating lower stability and weaker biomechanical profiles.
Limitations
This study has several limitations. The results obtained from finite element analysis (FEA) may not fully reflect the biological responses following fracture fixation due to individual variability in fracture morphology, technical differences during screw placement, and patient-specific factors such as body mass index (BMI), bone quality, and soft tissue characteristics. Furthermore, the study does not include clinical outcomes. Therefore, the findings should be interpreted as biomechanical guidance for surgical decision-making rather than direct predictors of clinical results.
Additionally, from an axial projection perspective, the posterior column of the acetabulum can be conceptualized as an isosceles triangle with a crescent-shaped base—bounded anteriorly by the acetabular joint, posteriorly by the greater sciatic notch, and medially and laterally by the inner and outer cortices of the column [14]. Accordingly, the aBCS is placed near the base of this triangle (adjacent to the acetabular surface), while the pBCS is positioned toward the apex near the greater sciatic notch. As the triangle narrows toward the apex, anatomical variations—particularly in the female pelvis, where the posterior column tends to be narrower and thinner—may limit the feasibility of placing a 6.5 mm diameter pBCS screw [42].
Therefore, caution is warranted when generalizing these findings, particularly in individuals where the posterior column tends to be narrower—most notably in female patients. In such cases, meticulous preoperative planning, preferably using advanced planning tools or software, is recommended to ensure safe screw placement. This anatomical perspective further underscores the necessity for future feasibility studies aimed at evaluating the applicability of the pBCS technique across diverse pelvic morphologies.




Comments (0)