
Remember me
In this study, an endogenous behavior model was constructed to explore how individuals might adopt either protective (P) or nonprotective (NP) behavior. These behaviors are defined on the basis of the number of sexual partners and variations in condom use. Having determined this behavioral distribution endogenously, the derived information was integrated into a Markov health-state transition model. This model aids in evaluating the long-acting PrEP (cabotegravir) in contrast to the conventional daily oral pill PrEP (TDF/FTC).
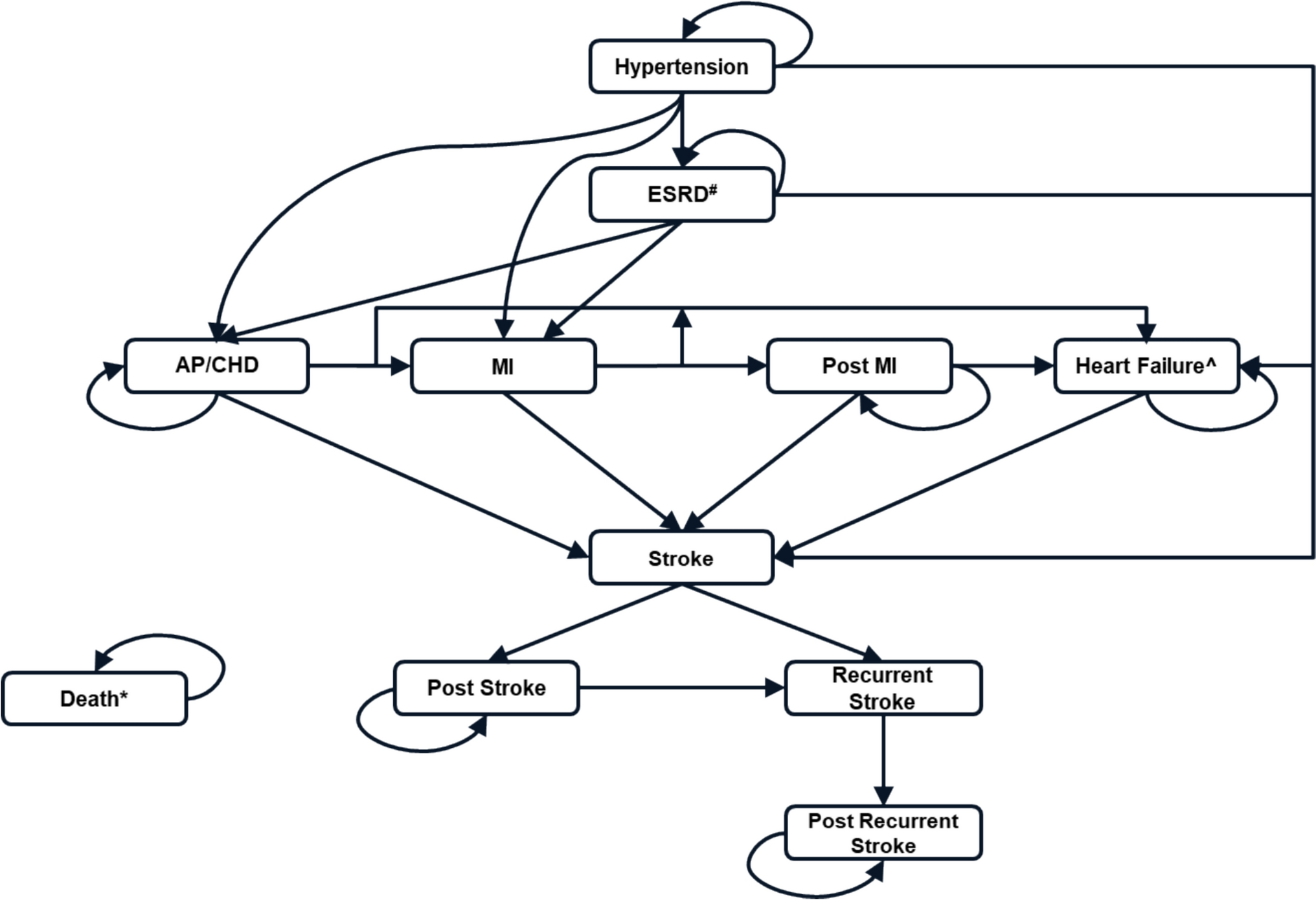
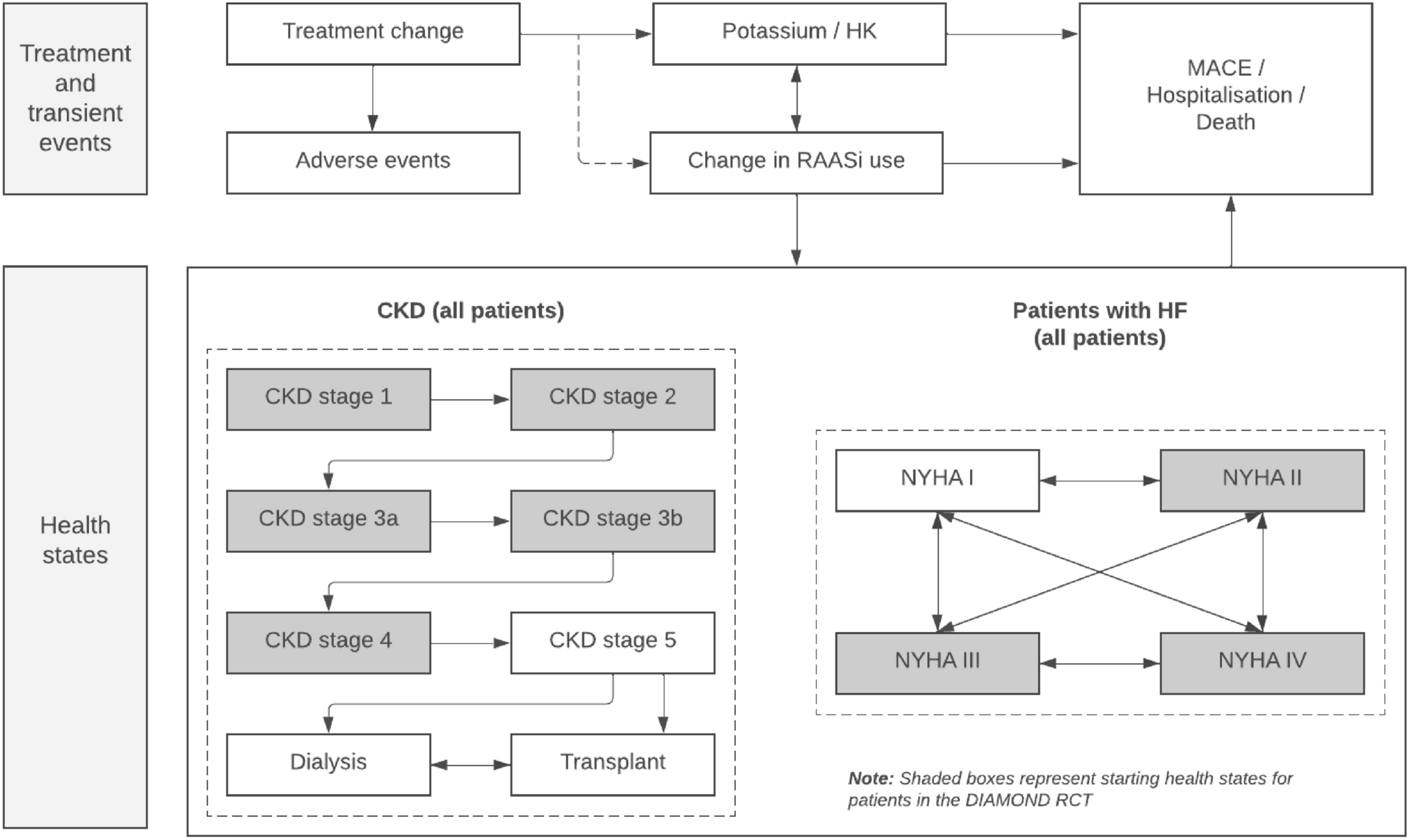
The underlying structure of the Markov health-state transition model remains consistent for both behavioral cohorts. However, certain parameters have been tailored for each group, ensuring a stylized representation of economic and health outcomes arising from their respective behaviors. It is important to note that once the behavioral distribution is determined by the endogenous behavior theoretic model, individuals are assigned to a fixed behavioral type—either P or NP—within the Markov framework. These types are not dynamically updated during the cohort simulation; rather, they represent stable classifications that reflect equilibrium behavior after the introduction of long-acting PrEP (cabotegravir). The schematic representation of our model is provided in Fig. 1.
Fig. 1
Conceptual diagram of the model
2.1 Individuals’ Endogenous Behavior ModelUtilizing evolutionary game theory, we examine how individuals endogenously respond to the availability of a long-acting PrEP treatment, which promises a significant reduction in the adherence challenges associated with traditional PrEP. The evolutionary perspective on game theory has garnered interest beyond its biological implications, extending into cultural considerations. While cultural and biological evolutions are intertwined, as cultural shifts can shape biological adaptations [6,7,8], their theoretical underpinnings differ. In a biological context, evolutionary game theory focuses on environments in which behavior is genetically ingrained, and strategy selection is driven by varying reproductive fitness among gene carriers. In contrast, our model delves into cultural evolution, emphasizing the role of learning processes. Within a community, individuals observe, learn from, and mimic behaviors they perceive as beneficial to their well-being. Such learning dynamics can reshape the distribution of beliefs and strategies within a population over time, mirroring the principles of biological evolution. Individuals typically harbor multiple ideas or potential behaviors, and the prominence of each is influenced by their experiences, learning trajectories, and the advantages reaped from specific actions. Thus, the evolution of ideas within an individual’s cognition can be analogized to biological evolution [9].
2.1.1 ModelIndividuals have two potential behavioral strategies: protective (denoted by P) and nonprotective (denoted by NP). These strategies manifest in real-world behaviors, such as number of sexual partners and condom use. Given the context of our study, it is essential to consider both historical behavior patterns (e.g., past number of sexual partners and drug use) and current interaction choices (e.g., condom use during a specific interaction). For instance, the payoff U (P,NP) is interpreted as the utility of an individual that has been taking the action (i.e., strategy) P when their partner has been taking the action NP. Similarly, U (P,P) is the utility when both individuals have been taking the action P. If both have historically chosen the same strategy, they continue with that strategy during the interaction. If one has previously chosen the NP strategy, the interaction defaults to the NP behavior.Footnote 1 It is assumed that an individual’s past behavior is transparent to their partner during an interaction. Partner HIV status, however, is assumed to be private information and not observable by the other individual.
In this model, we analyze the interaction between pairs of individuals. These interactions can be captured using specific strategy pairings, each with associated outcomes based on behavioral choices. Specifically, the potential strategy pairings are:
(P, P): Both players have historically exhibited protective behavior, and during the interaction, they persist with the protective approach (e.g., using condoms).
(NP, NP): Both players have a history of nonprotective behavior, which they continue during the interaction (e.g., forgoing condom use).
(P, NP): Player 1 has consistently been protective, whereas player 2 has been nonprotective. During their interaction, the prevailing behavior is nonprotective.
(NP, P): Here, player 1 has been nonprotective while player 2 has acted protectively. However, the interaction defaults to a nonprotective behavior.
The resulting payoffs, considering all potential interactions, are defined as:
$$_\left(P,P\right) = \overline$$
$$_\left(P,NP\right) = -\left(1 - \gamma \right)\lambda$$
$$_\left(NP,P\right) = \pi - \left(1 - \gamma \right)\lambda$$
$$_\left(NP,NP\right) = \pi - \left(1 - \frac\right)\lambda$$
Here, \(\overline\) represents the immediate utility derived when both players maintain their behavioral patterns, thereby not exposing each other to added risk. The parameter \(\pi\) quantifies the utility associated with a nonprotective behavior, which includes factors such as increased sexual partners and variance in condom use. The term γ denotes the efficacy of the PrEP treatment in preventing HIV acquisition, while \(\lambda\) indicates the disutility associated with contracting HIV.
In the context of this model, it is proposed that the overall utility derived from adopting a nonprotective behavior exceeds the expected disutility of acquiring HIV, as represented by the inequality:
$$\pi > \left(1 - \frac\right)\lambda$$
If this condition were not met, individuals would naturally avoid such behavior. In addition, when an opponent chooses the protective strategy, an individual is likely to also adopt the protective approach to minimize potential risks and the likelihood of acquiring HIV:
$$\overline> \pi - \left(1 - \gamma \right)\lambda$$
Long-acting injectable PrEP has emerged as a promising biomedical intervention, particularly for populations facing challenges with daily adherence. While it offers improved delivery and potential for greater effectiveness, its use may also influence individuals’ perceptions of risk and subsequent protective behavior. To explore these behavioral feedback effects, we developed a stylized model of endogenous behavior grounded in game theory, as presented in Table 1. The model seeks to understand these endogenous behavioral adjustments and estimate the distribution of individuals between the protective and nonprotective categories.
In a scenario where player 1 has historically adhered to a protective behavior while player 2 has been nonprotective, they both exhibit nonprotective behavior during their interaction. In this setting, player 1 incurs a negative expected payoff, equivalent to the expected disutility from the risk of acquiring HIV, represented as \(-\left(1 - \gamma \right)\lambda\). Conversely, player 2 realizes a positive expected payoff. This is computed as the net utility derived from prior nonprotective behavior, denoted as \(\pi\), subtracted by the expected disutility of potential HIV acquisition, represented as \(\left(1 - \gamma \right)\lambda\). In situations in which both players consistently adopt the nonprotective stance—both historically and during their interaction—the expected payoff for each is determined by the utility from nonprotective behavior, \(\pi\), reduced by the heightened expected disutility of HIV acquisition due to amplified risk. This heightened risk arises from their shared history of risky behavior and is mathematically represented as \(\left(1 - \frac\right)\lambda\).
In our analysis, two distinct pure strategy Nash equilibriums emerge: (P, P) and (NP, NP). On the basis of initial conditions, it seems reasonable to posit that individuals might inherently prefer the (P, P) equilibrium. This inclination can be attributed to the fact that the efficacy of the traditional oral pill PrEP treatment is largely contingent on consistent adherence to the daily pill—a task which presents considerable challenges. As underscored in reference [18], those at heightened risk of acquiring HIV often hail from socioeconomically disadvantaged backgrounds, characterized by lower income levels, limited education, and racial minority status. Such demographics may encounter increased barriers to maintaining consistent pill adherence over an extended duration. Moreover, even when infected, they might also confront significant obstacles in accessing and adhering to healthcare utilization, as indicated in reference [19]. Consequently, these high-risk individuals often resort to supplementary preventive measures, such as consistently using condoms and reducing their number of sexual partners.
Given the aforementioned factors, we can make a tentative assumption that individuals initially favored strategy P. This setup reflects the real-world context in which, prior to the introduction of long-acting PrEP, individuals were more likely to engage in protective behaviors owing to adherence challenges, lower perceived PrEP efficacy, and higher perceived risk. We model the availability of long-acting PrEP as a shift in these perceived conditions—primarily through increases in the behavioral utility of NP strategies (\(\pi\)) and efficacy (\(\gamma\)). These shifts influence the payoff structure and change the threshold, which determines whether the population converges toward NP or P behavior at equilibrium.
With this in mind, our objective is to identify the conditions under which strategy P can be successfully supplanted by the alternative, or “mutant,” strategy NP. Let us consider a scenario where a minute fraction, represented as \(_\), of the population consists of mutants adhering to strategy NP. Given the vastness of the population, the likelihood of an individual encountering a mutant (those employing strategy NP) is \(_\). Conversely, the probability of pairing with a nonmutant (those adhering to strategy P) stands at \(1-_\). Consequently, we can derive the expected payoff for a typical individual as follows:
$$U\left(P\right) = \left(1 - _\right)\overline-_\left(1 - \gamma \right)\lambda$$
$$U\left(P\right) =\overline-_(\overline+ \left(1 - \gamma \right)\lambda )$$
The expected payoff for a mutant individual that plays NP is
$$U\left(NP\right) = \left(1 - _\right)\left(\pi - \left(1 - \gamma \right)\lambda \right)- _ \left(\pi - \left(1 - \frac\right)\lambda \right)$$
$$U\left(NP\right) = \pi - \lambda \left[\left(1 - \gamma \right) + \frac_ \right]$$
If we compare the expected payoff of strategy NP with the expected payoff of strategy P, we get the following inequality:
$$U\left(NP\right) > U(P)$$
$$_> \frac-[\pi -\left(1-\gamma \right)\lambda ]}+\left(1-\frac\gamma \right)\lambda } =_^$$
(1)
The focal parameter for this study is \(_^\), denoting a pivotal threshold.Footnote 2 This parameter essentially dictates the conditions under which strategy NP can successfully supplant strategy P. From equation (1), one can deduce that when the proportion of mutants, \(_\), surpasses \(_^\), strategy P ceases to be an evolutionary stable strategy. This is attributable to the fact that strategy NP offers a more advantageous payoff, thereby enticing the entirety of the population toward its adoption, consistent with the replicator dynamic. Conversely, if the proportion of mutants, \(_\), is below the threshold \(_^\), the predominant strategy remains P. In situations where \(_\) equates to \(_^\), the population would exhibit a bifurcation in strategy adoption: a proportion \(_^\) would favor strategy NP, while the remaining \(1-_^\) would remain aligned to strategy P (for formal definitions of evolutionarily stable strategy and replicator dynamic, see Appendix 2).
In this study, the parameter \(_^\) is of primary interest, especially in relation to the exogenous parameters presented in Table 2. As anticipated, an increased utility derived from adopting the nonprotective behavior (\(\pi\)) reduces the critical threshold of mutants necessary for the successful invasion of strategy P. This translates to the idea that a minimal subset of individuals adopting strategy NP can sway the majority to adopt the same, especially as \(\pi\) elevates (\(\frac_^} < 0\)). The logic underpinning this is straightforward: the allure of the utility associated with strategy NP outweighs that of P, with everything else being equal.
Table 2 Net effect on the fraction of mutants \(_^\)Conversely, a heightened disutility from acquiring HIV makes the successful invasion of strategy P less probable since it demands a more substantial fraction of mutants (\(\frac_^} > 0\)). It stands to reason that individuals would be more reticent in adopting strategy NP if the repercussions of acquiring HIV are notably severe. Moreover, increasing the efficacy of the long-acting PrEP tilts the balance in favor of adopting strategy NP. This is attributed to the improved survival prospects even if HIV is acquired (\(\frac_^} < 0\)). Lastly, an elevated \(\overline\) necessitates a larger proportion of mutants for the invasion of the prevailing strategy (\(\frac_^} } > 0\)). A rise in the inherent utility derived from a consistent behavioral pattern (\(\overline\)) makes individuals more cautious, disinclining them from strategy NP and the associated risks. Consequently, it becomes more challenging for strategy NP to gain a foothold since many are content with the prevailing status quo. Comprehensive derivations of these findings are detailed in Appendix 3.
Building on the foundational game mechanics delineated earlier, it becomes pertinent to examine the implications of introducing the long-acting PrEP treatment on the game’s initial conditions. The enhanced reliability of this treatment—attributed primarily to the diminished dependency on consistent adherence—augments the overall effectiveness of the PrEP intervention. Furthermore, there is an associated psychological dimension to consider. Individuals are likely to perceive an elevated utility from engaging in nonprotective behavior. This stems from diminished concerns regarding consistent adherence to the daily pill regimen, both for themselves and their interaction partners. Within the construct of our model, this behavioral shift would manifest as increases in both \(\gamma\) and \(\pi\). The implication of this is profound: a larger segment of the population would gravitate toward the NP strategy, potentially making this strategy more adept at supplanting strategy P.
In essence, a rise in the values of \(\pi\) and \(\gamma\) will lead a larger segment of the population to gravitate toward strategy NP. This inclination can be ascribed to the enhanced probability of the mutant strategy securing a more favorable payoff in comparison with the prevailing one. For illustrative purposes, assuming \(_ = _^\) allows us to distinctly delineate the population’s composition: \(_^\) denotes the fraction adhering to strategy NP, while \(1 - _^\) encapsulates those committed to strategy P.
2.2 Markov Health-State Transition ModelOur model delineates four health states: not infected, HIV infection, AIDS, and death, tailored for each of the two populations encompassed within our analytical framework. The model draws inspiration from Adamson et al. [20]. In addition, our approach aligns with the methodological recommendations of the Second Panel on Cost-Effectiveness in Health and Medicine, satisfying standardized reporting prerequisites [21].
2.2.1 Study PopulationWe focus on a US-based population of individuals at an elevated risk for HIV, specifically cisgender men who have sex with men (MSM) and transgender women who have sex with men. This population reflects key demographics targeted in HIV prevention efforts and aligns with those studied in the HPTN 083 trial, which evaluated the efficacy and safety of long-acting injectable cabotegravir versus daily oral TDF/FTC [5]. Although the trial was conducted across multiple global regions, the majority of enrolled participants were based in the USA, making it a relevant source of clinical effectiveness data for our analysis.
2.2.2 Interventions, Perspective, and ComparatorsWe evaluate the efficacy of the long-acting PrEP cabotegravir in comparison with the conventional daily oral-pill PrEP TDF/FTC (branded formulationFootnote 3). Patients slated for the cabotegravir regimen commence with a 1-month, daily oral lead-in comprising FDA-approved cabotegravir in tablet form and oral rilpivirine to ascertain tolerance. This is followed by an initial dose of 600 mg cabotegravir combined with 900 mg rilpivirine. Thereafter, patients are administered monthly injections, each comprising 400 mg of cabotegravir and 600 mg of rilpivirine. In contrast, TDF/FTC is prescribed as a once-daily medication. For both treatment strategies, we assume full adherence throughout the model time horizon—that is, 100% adherence to both the long-acting injectable regimen and the conventional daily oral pill.
From an economic standpoint, our evaluation prioritizes the US healthcare sector perspective, emphasizing direct medical and pharmacy costs. The four-state Markov model tailored for each demographic group operates on a 1-month cycle length, with a primary time horizon set at 2 years (24 months). Results for alternative time horizons, both shorter (12 months) and longer (36 months), are also provided. Following standard practices in literature, we apply a 3% discount rate for both costs and health outcomes. All financial figures are presented in 2021 US dollarsFootnote 4. To measure the welfare impact of both treatments on the individuals, we compute the quality-adjusted life years (QALYs).
2.2.3 Model InputsTable 3 presents the key model inputs.
HIV Incidence: Input values for HIV/AIDS incidence (transition probabilities) were derived from the World Health Organization, a randomized, double-blind, double-dummy, noninferiority trial comparing the long-acting injectable PrEP with its daily oral pill counterpart, and a comprehensive review of relevant literature.
The transition probability from the not-infected state to the HIV state was modulated on the basis of an individual’s behavior (i.e., protective or nonprotective) and the respective treatment. Specifically:
For the traditional PrEP and long-acting PrEP, the primary distinction between a protective and a nonprotective individual lies in condom use. A protective individual consistently uses condoms, leading to an 80% enhanced reduction in transmission risk compared with their nonprotective counterparts that do not regularly use condoms [29, 30].
Clinical Inputs: Individuals with a new HIV diagnosis experience health progression characterized by CD4+ T-cell count categories. An individual is classified as not-infected upon testing negative, HIV-diagnosed upon testing positive, and in the AIDS stage when a positive diagnosis accompanies a CD4 count < 200 T-cells per mL.
Health State Utility: The health state utility values employed are rooted in established literature [25,26,27], which provide preference-based utility weights for HIV states determined by CD4+ T-cell counts. The utility values for the HIV-diagnosed and AIDS states remain consistent across both PrEP types and independent of protective or nonprotective behaviors. The utility value for uninfected, protective individuals is calculated as a weighted average of individual age distributions (gleaned from trial data) and the utilities of healthy male individuals from the general US population. In addition, potential side effects of cabotegravir and TDF/FTC treatments are factored into these utilities. Conversely, nonprotective, uninfected individuals are assigned higher utility values in both PrEP types, reflecting their predisposition for risk-taking behaviors and their preference for less restrictive prevention strategies (e.g., sex without barrier methods). This modest utility increment (e.g., 0.001) is informed by discussions with HIV clinicians and behavioral experts and is further supported by literature indicating that less restrictive sexual experiences are often associated with greater physical satisfaction and emotional closeness [31]. The utility increment is larger for long-acting PrEP owing to minimized adherence challenges. The specific increments in utility were assumed, and sensitivity analyses were performed around these parameters.
Costs: Costs are based on published literature, adjusted to 2021 US dollars using the consumer price index. From a healthcare sector perspective, the costs reflect both payer and patient medical expenses [21] and are determined at the microlevel. We further consulted a US-based study detailing healthcare expenditures for patients with HIV, segregated by CD4-count categories, to ascertain the cost values for HIV and AIDS care. It is notable that costs remain invariant across protective and nonprotective behavioral categories.
2.2.4 Model OutputsA hypothetical cohort was monitored from the intervention’s commencement for a period of 24 months, with additional results provided for extended and truncated time horizons. Outcomes are presented as per-person averages. These data are disaggregated for the two populations: protective and nonprotective.
2.2.5 Cost-Effectiveness AnalysisThe principal economic outcome generated by the model is the incremental cost-effectiveness ratio (ICER). To offer an interpretation of cost-effectiveness, we set a threshold based on the assumed willingness to pay for health improvements. Drawing from the existing literature, we classify ICER values < 80,000/QALY as highly cost-effective, those between 80,000 and 100,000/QALY as cost-effective, and values > 100,000/QALY as potentially not cost-effective. This categorization is based on a 24-month time horizon. It is worth highlighting that the model will produce two distinct ICER values: one for the protective (P) population and another for the nonprotective (NP) population. However, by defining the population proportions for each group, it becomes feasible to derive a singular, weighted ICER value as follows:
$$ICE_=_\times ICE_+_\times ICE_$$
2.2.6 Sensitivity AnalysisWe conducted two types of sensitivity analyses to assess the robustness of our results. First, we performed sensitivity analyses on key model inputs, including costs, utilities, and efficacy parameters. These were carried out separately for individuals classified as protective (P) and nonprotective (NP), reflecting the fact that each behavioral type is associated with distinct parameter values. For each sub-population, we estimated an ICER comparing long-acting PrEP (cabotegravir) with traditional daily oral PrEP (TDF/FTC). These subgroup-specific ICERs were then combined using behavioral weights PP and NP, representing the assumed proportions of the population adopting each behavior. This structure allowed us to capture how input uncertainty affects cost-effectiveness, conditional on a given behavioral distribution.
To operationalize this, we conducted a one-way sensitivity analysis, adjusting the values within the upper and lower bounds of select input parameters while keeping other variables constant. This analysis was performed to assess the sensitivity of our model in response to variations in key parameters. The parameters evaluated in this sensitivity analysis include: cost of HIV care, cost of AIDS care, utility of noninfection for traditional PrEP (TDF/FTC) in the nonprotective group, utility of noninfection for long-acting PrEP (cabotegravir) in the nonprotective group, efficacy of long-acting PrEP (cabotegravir) in the nonprotective group, efficacy of traditional PrEP (TDF/FTC) in the nonprotective group, cost of daily oral PrEP (TDF/FTC), and cost of long-acting PrEP (cabotegravir).
In addition, a probabilistic sensitivity analysis (PSA) was conducted to evaluate the uncertainty associated with the input parameters. The underlying principle of PSA is to incorporate diverse values for each parameter, derived from specific distributions, thereby appraising the uncertainty in parameters extracted from observational data. This methodology empowers us to ascertain the confidence level of the cost-effectiveness analysis results, particularly concerning the sensitivity of these results to plausible alterations in input parameters. Table 3 presents insights into each parameter’s input values, standard deviation, and the selected distribution (for extra details about the PSA, see Appendix 4).
The primary outcomes of this analysis will be represented on the incremental cost-effectiveness plane, showcasing each simulation alongside a benchmark line for a US$100,000/QALYs threshold, and the cost-effectiveness acceptability curve. While the former visualization aids in the interpretation of results given the simulated inputs, the latter illustrates the proportion of instances in which each treatment emerges as cost-effective for a defined threshold. This dual representation facilitates a deeper understanding of result uncertainty, offering more than a mere confidence interval around a deterministic value.
Second, we conducted a sensitivity analysis on the behavioral distribution itself. In this case, all input parameters were fixed, and we varied only the proportion of individuals adopting protective (PP) versus nonprotective (PNP) behavior. Using the ICERs previously estimated for each behavioral group for the input values in our model, we computed the overall ICER under a range of distributional scenarios (e.g., 100% NP, 80/20, and 50/50).
Separating these two analyses allowed us to isolate the effects of model input uncertainty from the effects of shifts in population behavior.
Details on model validation are provided in Appendix 5.
Comments (0)