
Remember me
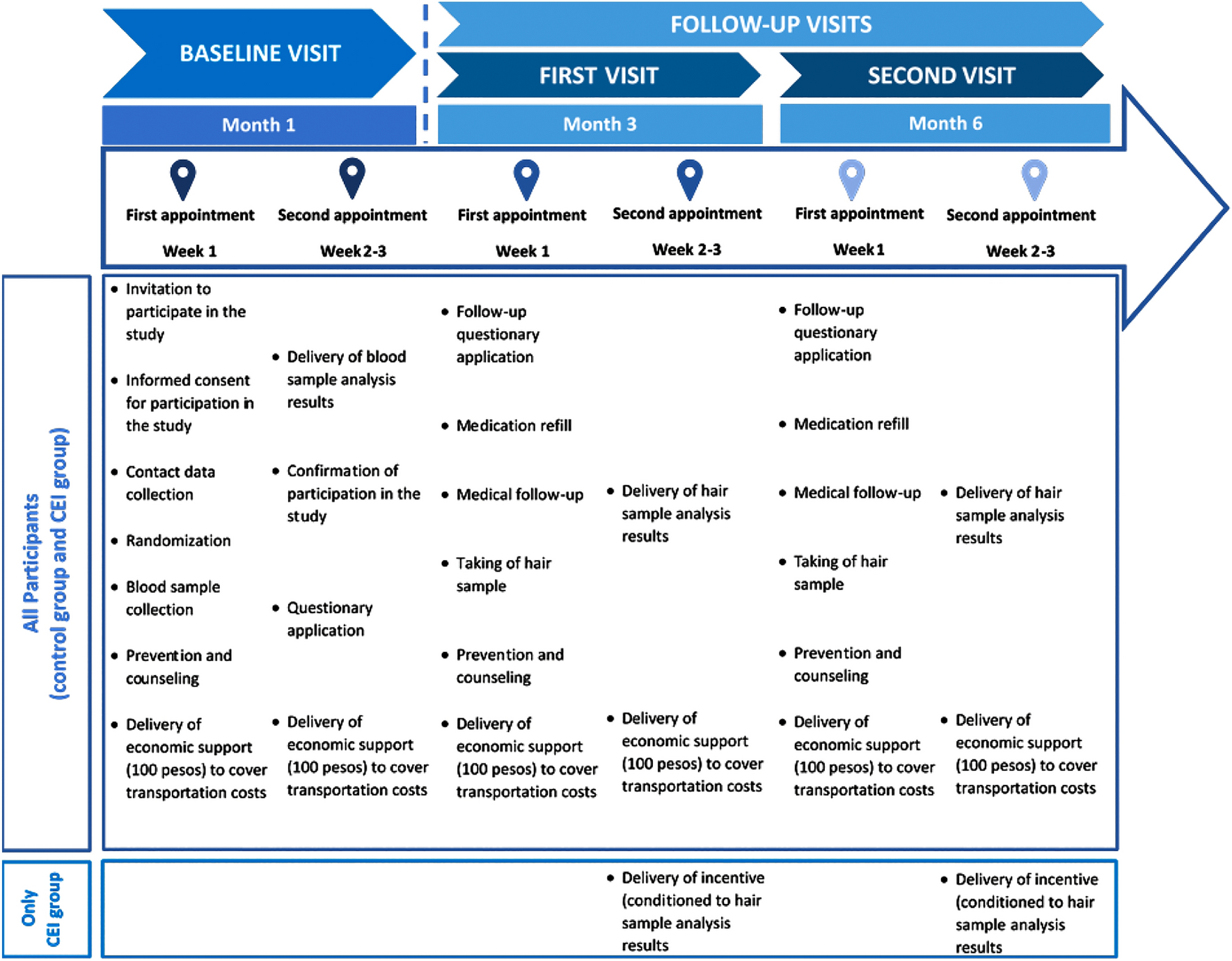
We conducted a randomized pilot study to evaluate the effectiveness of using conditional economic incentives (CEIs) to increase adherence to free PrEP among male sex workers (MSWs) in Mexico City (ClinicalTrials.gov identifier: NCT03674983). Detailed explanation of the trial design and findings are available elsewhere [19]. Eligible participants were male, aged 18 years or older, HIV-negative within the past month, and reported engaging in penetrative sex with at least four male partners and exchanging sex for money, drugs, or gifts on four or more occasions in the past month. They also needed to be part of the ImPrEP project (more details elsewhere [19]), able to provide contact information, willing to give blood and hair samples, and capable of providing informed consent. Participants were recruited by research and clinical staff at Clínica Condesa during scheduled care visits and through community outreach at known sex work locations in Mexico City such as La Alameda Central, Zona Rosa, and Metro Hidalgo. Male sex workers recruited in these venues were first enrolled in the ImPrEP program before being invited to join the PrEP Seguro study. Clínica Condesa is a primary, outpatient care center for people living with HIV and the largest provider of antiretroviral treatment in Mexico. The clinic also offers screening for sexually transmitted infections and general HIV prevention and care in Mexico City. The trial enrolled 110 male sex workers who were then randomly assigned to receive standard HIV prevention care alone or standard HIV prevention services with conditional incentives. PrEP adherence was assessed on the basis of tenofovir/emtricitabine (TDF/FTC) concentrations in scalp hair samples collected at the first study visit following randomization (baseline), as well as at the 3- and 6-month visits post randomization (Fig. 1). Hair samples were collected at each of the three primary study visits (baseline, 3-month, and 6-month visits). Owing to the coronavirus disease-2019 (COVID-19) pandemic, there were at times delays in processing and analyzing these samples, with the results taking approximately 3 months to become available. As a result, the incentives for participants in the intervention group were delivered at the subsequent visit after the test results were received. Despite these delays, all participants—both in the intervention and standard care groups—attended the same number of study visits.
Fig. 1
Study design of the PrEP Seguro randomized pilot trial
Individuals randomized to the intervention condition received economic incentives based on level of PrEP adherence measured at each of the three study visits. Participants with TDF/FTC concentrations of at least 0.043 (ng/mg), consistent with taking five to seven pills per week, received an incentive of ~ US $20. Those with concentrations between 0.011 (ng/mg) and 0.042 (ng/mg), indicating taking three to four pills per week, received an incentive of ~ US $10. Participants with concentration levels below 0.011 (ng/mg), consistent with taking two or fewer pills per week, received no incentive [15].
2.2 Collection of Cost DataWe used a direct-measure microcosting approach to estimate the costs associated with providing healthcare resources to study participants. Microcosting is a detailed and granular costing method that involves identifying and valuing all the individual components of a healthcare intervention. In this study, cost information was collected from May 2019 to August 2020 from the healthcare provider’s perspective (Clínica Especializada Condesa). This involved a thorough review of administrative records and interviews with key informants such as clinic managers and healthcare staff.
We identified all relevant resources used in delivering the intervention and standard care. Direct medical costs included the cost of the PrEP medication (tenofovir) and the resources associated with routine scheduled HIV care visits. For each scheduled visit, we recorded the cost of infectious disease tests, such as tests for gonorrhoea, chlamydia, syphilis, and other clinically indicated infections.
We also considered the cost of healthcare personnel time, including physician consultations and counseling services. This was estimated on the basis of the average salaries of providers and social workers at the clinic (Clínica Especializada Condesa). For each identified resource, we obtained the unit costs from the clinic’s financial records. For example, the cost of PrEP was based on the actual purchase price paid by the clinic, which could differ from market prices owing to bulk purchasing agreements or subsidies.
To facilitate comparison and ensure consistency, we adjusted all base unit costs to reflect a common year and currency. The costs were first standardized to 2020 values using Mexico’s 2020 consumer price index (CPI) to account for inflation. After adjusting for inflation, all costs were converted from Mexican pesos to US dollars (US $) using the 2020 World Bank official exchange rate (local currency units (LCU) per US $, period average) [21]. This process ensured that the cost estimates were presented in a standardized currency, making them comparable to international studies [21]. The mean cost of tenofovir was US $104. This cost estimate in our study reflects the procurement cost paid by the specific clinic participating in the trial, which may differ from retail prices owing to bulk purchasing agreements or subsidies. Online Table A2 shows the unit costs of the material and human resources involved in care and intervention delivery during the trial.
2.3 Quality-Adjusted Life YearsWe estimated the number of quality-adjusted life years (QALYs) for each enrolled participant at 6-months based on the number of HIV infections averted owing to being sufficiently highly adherent to PrEP. First, we defined sufficient adherence using a dichotomous variable derived from hair analysis results. A TDF/FTC hair sample concentration below 0.011 ng/mg (equivalent to taking three to four pills per week) was classified as nonadherent (0) and a concentration of at least 0.011 ng/mg (equivalent to taking at least three pills per week) was classified as adherent (1) [22]. Among participants randomized to receive standard care without incentives, 62% of male sex workers were categorized as adherent at the end of the 6-month follow up period. Among participants randomized to the incentive condition, 78% were adherent after 6 months. Next, for both trial arms, we calculated the number of prevented HIV infections owing to sufficient PrEP adherence over the 6-month trial. We assumed an incidence rate of five new HIV cases per 100 person-years [3] and a PrEP effectiveness of 96% [23]. At each measurement timepoint (baseline, 3-month visit, and 6-month visit), we calculated the infections avoided by each adherent patient as:
$$\text.\text=\text\times \, \text.$$
For the first visit, we estimated 0.3936 infections avoided = (0.41 new HIV cases per month) (0.96). Similarly, for the 3-month and 6-month visit, we estimated 1.2 infections avoided = (1.25 new HIV cases per 3-month) (0.96). Next, to estimate the total infections avoided over the whole 6-month period, we summed the infections avoided for each visit. Last, to calculate the QALYs gained per averted infection, we used a lower limit of 4.45 QALYs [24] and an upper limit of 6.43 QALYs [25]. We calculated the mean number of QALYs gained by each program based on these ranges. More details about QALY estimation are summarized in Online Table A2.
2.4 Incremental Cost-Effectiveness RatiosWe calculated the incremental cost-effectiveness ratio (ICER) as the additional cost needed to gain one additional QALY, comparing the CEI-based program to standard care. The ICER was calculated by dividing the difference in costs between the intervention and standard care arm (ΔC) by the difference in QALYs for the same comparators (ΔE) (ICER = ΔC/ΔE). We used Mexico’s per capita gross domestic product (GDP) in 2020 (US $8655) as a willingness-to-pay (WTP) threshold for determining cost-effectiveness [26]. Two WTP thresholds were used in this analysis. First, we employed a threshold of US $8500, representing Mexico’s per capita GDP in 2020, in line with a commonly used benchmark in health economic evaluations [27]. This threshold assumes that an intervention costing less than the per capita GDP per QALY gained is generally considered cost-effective. However, recognizing the limitations of this approach, particularly in low- and middle-income countries, we also used a more stringent threshold of US $3850, as suggested by Woods et al. [28]. This threshold is based on empirical estimates of the health opportunity costs specific to Mexico, offering a more realistic assessment of the intervention’s value given the country’s healthcare context.
2.5 Sensitivity AnalysisWe conducted a probabilistic sensitivity analysis (PSA), specifying appropriate probability distributions for each key parameter. Costs, including medication, clinical visits, and administrative overhead, were modeled using gamma distributions, reflecting their skewed nature and non-negativity. The effectiveness of the intervention, measured in quality-adjusted life years (QALYs) gained, was modeled using a beta distribution, which is suitable for variables bounded between 0 and 1. We then ran 10,000 Monte Carlo simulations, in which values for each parameter were randomly drawn from their respective distributions. Each simulation generated a potential scenario, allowing us to calculate a distribution of possible outcomes for costs and QALYs for both strategies: standard PrEP care and PrEP + CEI. From these outcomes, an ICER was calculated for each iteration, providing a distribution of ICERs rather than a single point estimate.
The results of these simulations were analyzed to estimate the probability that the PrEP + CEI intervention would be cost-effective at various willingness-to-pay (WTP) thresholds. We constructed cost-effectiveness acceptability curves (CEACs) to visualize the proportion of simulations where the ICER was below given WTP thresholds. This graphical representation helped illustrate the uncertainty around the intervention’s cost-effectiveness. The cost-effectiveness analysis and probabilistic sensitivity analysis (PSA) were conducted using R software (version 4.3.1) with the dampack package [29]. This software facilitated the calculation of the incremental cost-effectiveness ratio (ICER) and allowed us to rigorously address uncertainty in key parameters such as costs and health outcomes [29].
2.6 Ethical AspectsAll human subject protocols and materials implemented during the PrEP Seguro study were approved by ethics committees at Brown University (Institutional Review Board (IRB) Authorization Agreement no. 18–70) and Mexico’s Instituto Nacional de Salud Pública (National Institute of Public Health) (protocol no. P33-18, project CI: 1551). All trial participants provided written informed consent for study participation and for the use of their data for research purposes.
Comments (0)