
Remember me
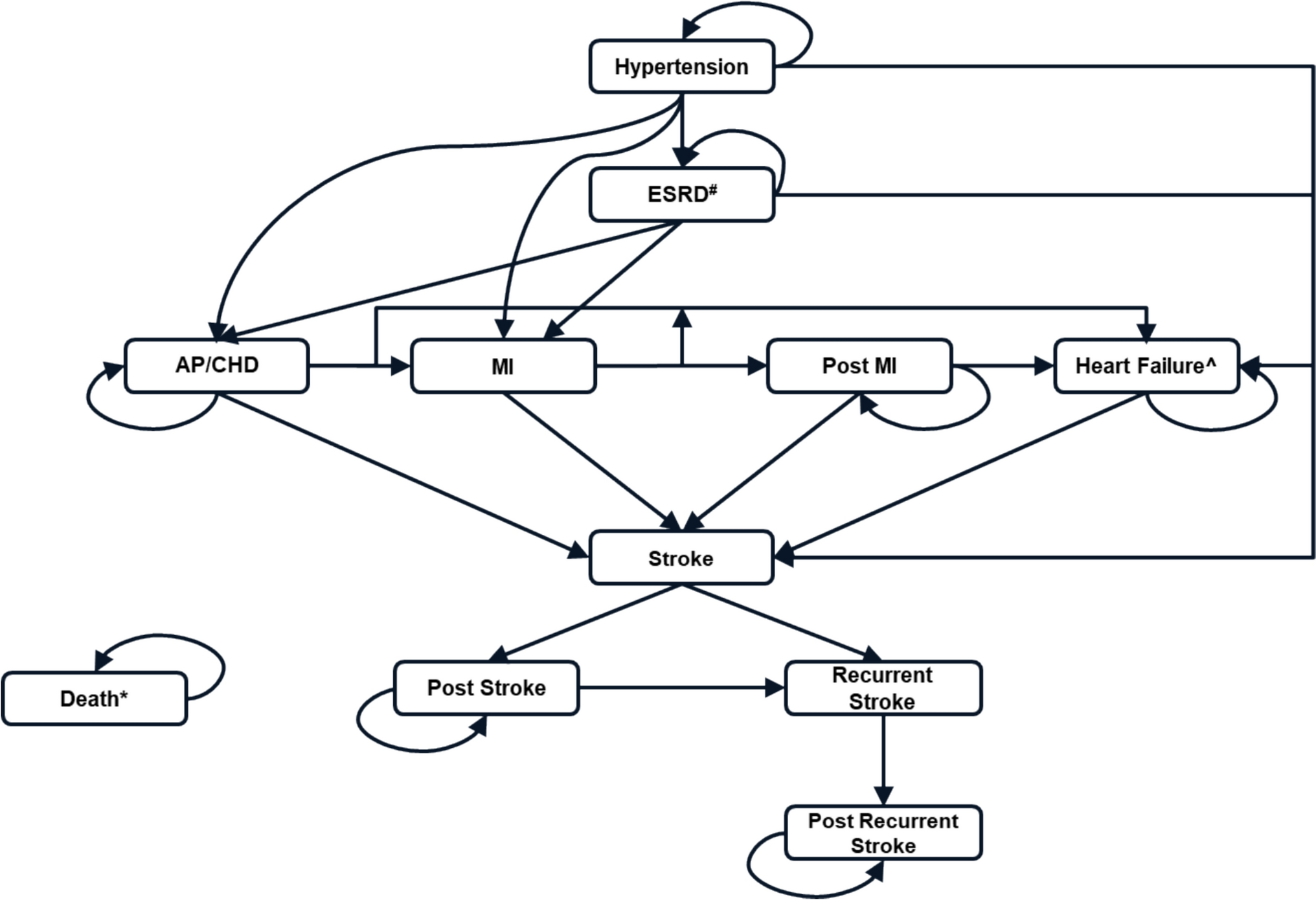
A cost-utility analysis was conducted using a partitioned survival model with three mutually exclusive health states: progression-free (initial state), progression, and death (end state) (Fig. 1). The model was developed using data from the DESTINY-BREAST04 clinical trial [3] and cost and resource use data were adapted to reflect the perspective of the Spanish National Health System (NHS). Cost data were sourced from official Ministry of Health databases and published literature. The analysis was conducted over a 75-month time horizon, incorporating monthly cycles. This period was selected to extend the evaluation beyond the 34-month follow-up period of the DESTINY-BREAST04 clinical trial, with the objective of more accurately capturing long-term variations in costs and outcomes between treatments. This report was created using the CHEERS 2022 checklist adapted into Spanish [8] (Table S1 in the electronic supplementary material [ESM]). The alternative therapies analysed were T-DXd versus standard of care (capecitabine, gemcitabine, eribulin, paclitaxel, nab-paclitaxel, sacituzumab govitecan, or vinorelbine). These two options were compared in two groups—the total sample enrolled in the DESTINY-BREAST04 clinical trial and a subgroup of hormone receptor-positive (RH+) patients. This trial was chosen because it provides robust and high-quality evidence on the efficacy of T-DXd in HER2-low metastatic breast cancer, making it the most relevant source for this analysis.
Fig. 1
Diagram of the partitioned survival model used in the cost-effectiveness analysis, including three mutually exclusive health states: progression-free, post-progression, and death
Health outcomes were measured as quality-adjusted life years (QALY), which is the length of survival weighted for quality of life (utility). Additionally, overall survival (OS) and progression-free survival (PFS), as reported in the clinical trial, were used to validate the model's outcomes and ensure consistency with the source data. Adverse events were included in the model if they occurred in at least 20% of patients and were grade ≥ 3. The only exception was nausea and vomiting, which, as T-DXd is considered a moderately emetogenic agent [9], was classified as a single adverse event type with all grades included due to the high number of patients experiencing this type of event.
OS and PFS curves were modelled to determine the average time spent by patients with these two health states. Data points obtained by digitizing survival curves and aggregated data from the DESTINY-BREAST04 publication were used to trace Kaplan-Meier curves, according to the algorithm described by Guyot et al. (2012) [10]. Cox regression hazard ratios (HRs) were calculated to compare the obtained data with the original data. Multiple parametric distributions (e.g., gamma, lognormal, Weibull, Gompertz) were analysed. The final curve selection was based on (1) Akaike information criterion (AIC) values, which reward the goodness of fit of the model to the data and penalize overfitting; (2) visual comparison of the modelled curves with the test curve; and (3) clinical validation conducted by health professionals [11] (Tables S2, S3, Fig. S1, see ESM). Based on these criteria, the Weibull distribution was selected for both OS and PFS curves, as it provided the best balance of goodness-of-fit, interpretability, and clinical relevance. The AIC values supporting this choice are detailed in Tables S2 and S3 of the ESM. The Kaplan-Meier curves and the selected parametric survival curves for both OS and PFS are shown in Figures 2a and 2b, respectively. All the above analyses were performed using the Flexsurv package of the statistical program ‘R’ v3.3.2.
Fig. 2
Projected health state distribution over 75 months for patients receiving trastuzumab deruxtecan
Utility values were obtained from the systematic review performed by Paracha et al. (2016) [12]. This review aimed to identify utility values related to health states in breast cancer. Data were preferably collected using direct methods developed for health technology assessment agencies. Utility values related to the presence of adverse events were neither applied nor estimated.
The study estimated the total healthcare costs within the Spanish National Health System (NHS) for different approaches. Given the complexity and difficulty of collecting data on all potential subsequent treatment rounds after disease progression, the most likely treatment options were agreed based on recommendations from the EMA, the Therapeutic Position Statements of the Spanish Agency for Medicine and Healthcare Products [4, 5], the Austrian Institute for Healthcare Technology Assessment (AIHTA) [13], and the Guide to the Integrated Breast Cancer Care Process of the Public Health System of Andalusia [14]. A panel of three experts, including one oncologist and two hospital pharmacists, reached consensus through structured discussions and iterative feedback sessions to estimate the frequency of use of each type of drug (capecitabine, gemcitabine, eribulin, paclitaxel, nab-paclitaxel, sacituzumab govitecan, and vinorelbine). These estimates also considered the frequencies described in the hallmark trials for each scenario. Table S4 shows the treatments used after relapse and the proportions used (see ESM). Bot-Plus was used to obtain the laboratory sales price of drugs in the primary care setting [15], while the official Ministry of Health database, Nomenclator [16] (March 2020), was used for the hospital setting, after deducting possible legal discounts. A standard weight of 70 kg and a body surface area of 1.65 m2 were considered for patients.
Defined activities, established standards, and identified resources were used to estimate the costs of adverse events. Cost data for diagnostic tests, clinic visits, and procedures were extracted from the 2005 Official Bulletin of the Council of Andalusia [17, 18] and subsequent updates. Medical costs post-progression were assumed to remain stable due to a lack of specific data on variations in resource use during this phase. This assumption has been tested through sensitivity analysis to explore its potential impact on the results. The costs of T-DXd and premedication (ondansetron and dexamethasone) were also included [6, 9]. Table 1 provides a comprehensive overview of the considerations used to estimate the direct healthcare costs, including the monthly costs of adverse events, follow-up care, pharmaceutical treatments, and medical appointments. These considerations represent the most relevant factors based on the availability and reliability of the data. Costs were updated to 2023 using the Consumer Price Index [19] as more recent data were not available at the time of analysis. A total of five healthcare professionals, including two hospital pharmacists, two pharmacoeconomists, and one medical oncologist, validated the data to ensure that the assumptions were consistent with clinical practice in the NHS. Consensus was reached through structured discussions and iterative feedback sessions.
Table 1 Direct healthcare costs used to estimate the monthly costs of adverse events, follow-up care, medications, and related visits in patients with HER2-low metastatic breast cancerTable 2 summarizes the main cost and utility inputs used in the base-case analysis. These include pharmaceutical acquisition costs, management costs of adverse events, follow-up costs, and health state utilities. All values were derived from published literature, official Spanish healthcare databases, or expert consensus, and reflect the perspective of the Spanish National Health System. These inputs served as the basis for both the cost-effectiveness and budget impact analyses.
Table 2 Cost and utility values employed in the budget impact evaluation and cost-effectiveness analysis of trastuzumab deruxtecan (T-DXd) versus standard treatmentIn order to ensure the accuracy of the cost estimates, it was necessary to make several assumptions regarding pharmaceutical treatments, adverse events, and follow-up care. The following considerations were critical to defining the costs included in the model and ensuring alignment with clinical practice and available data sources:
Pharmaceutical cost considerations: Follow-up costs incorporated the performance of computed axial tomography every 5 months and a blood count analysis every 30 days. With regards to specialist appointments, it was assumed that all patients receiving oral treatment had a monthly specialist appointment, whilst those treated intravenously had a specialist appointment for each administration. Finally, it was assumed that all patients who were going to die ceased treatment 1 month prior.
Considerations for the cost of adverse events: For each adverse event, in addition to pharmacological treatment, one specialist appointment was also counted. In the case of adverse events that led to treatment disruption, disruption was standardized in a cycle.
Considerations for appointments: Appointment costs extracted from the 2016 Official Bulletin of the Council of Andalusia (BOJA) was updated in 2023 using the Consumer Price Index (CPI).
Analyses were performed in Microsoft Excel 2016. The base-case analysis applied a 3% discount rate to all costs and health outcomes, in line with common practice in health economic evaluations. Cost parameters were informed by real-world pricing obtained from a panel of experts, including one oncologist and two hospital pharmacists, who shared insights based on structured discussions and clinical experience. These expert-informed estimates were incorporated into the base-case model, and the corresponding outcomes are presented in Table 3 and Table S5 (in the ESM).
Table 3 Incremental cost-effectiveness analysis of trastuzumab deruxtecan (T-DXd) compared with standard treatment, considering a 75-month time horizon, for all patients and the hormone receptor-positive subgroupTo facilitate interpretation of results in relation to acceptable cost-effectiveness thresholds, we also applied four willingness-to-pay thresholds (€21,000, €24,000, €25,000, and €60,000/QALY) derived from the Spanish context [21, 22], and calculated the price at which T-DXd would become cost effective in both the full and RH+ populations.
A univariate sensitivity analysis was conducted to explore parameter uncertainty. Where standard deviations or confidence intervals were unavailable, plausible variations were applied to key model inputs. These analyses were based on the inputs presented in Table 2.
We also explored the impact of alternative assumptions in scenario analyses:
Utility values from a US-based economic evaluation by Lang et al. (2023) [20] were applied to test the robustness of base-case results.
A 5% discount rate was used in place of the base-case 3% to evaluate the impact of higher discounting on cost-effectiveness outcomes.
With regards to budgetary impact, an estimated 35,001 new cases of breast cancer were diagnosed in Spain in 2023 [1], with approximately 50% characterized by low levels of the HER2 protein and 10% in a metastatic state [2]. Between 70% and 90% of patients could be considered for first-line treatment [23], and 10–15% of invasive cases lack hormone receptors and have low levels of HER2 [24]. Among the total cases, 1750 were identified as metastatic low HER2 breast cancer, including 1532 hormone receptor positive (RH+) cases and 175 hormone receptor negative (RH-) cases. Within this group, 1400 patients could be eligible for treatment, including 1225 RH+ patients.
The budget impact analysis was conducted using a decision-analytic model to estimate the financial consequences of adopting T-DXd in clinical practice from the perspective of the Spanish National Health System. The analysis was structured in two stages: a preliminary static analysis, estimating costs over a 5-year period assuming a fixed patient population, and a dynamic analysis, incorporating annual incidence rates to account for new eligible patients each year. This approach allowed us to assess both the immediate and cumulative financial impact of T-DXd treatment over time.
The cost projections for the 5-year period were based on treatment duration, drug acquisition costs, and healthcare resource utilization, with consideration given to disease progression and treatment discontinuation rates. Furthermore, sensitivity analyses were conducted to evaluate the impact of key parameters on budget estimates. One-way sensitivity analyses assessed variations in market penetration rates, drug costs (including potential discounts), and incidence rates, while a scenario analysis explored the effect of alternative time horizons.
In order to reflect potential adoption patterns, it was assumed that T-DXd would achieve a gradual increase in market penetration, reaching 100% among eligible patients by the end of the 5-year period. This scenario considers an initial lower market share, consistent with real-world adoption dynamics, followed by a progressive increase as clinical experience accumulates and prescribing practices evolve. While this assumption represents an upper-bound estimate, it allows for a more complete evaluation of the potential financial impact of T-DXd introduction.
Comments (0)