
Remember me
A partitioned survival model was created to compare the costs and benefits of daily remote arrhythmia monitoring using an ICM combined with SoC compared with SoC alone for high-risk NSTEMI patients. The analysis was conducted over a lifetime horizon, and health benefits and costs were discounted at an annual rate of 3.5% [17]. The model used 6-monthly cycles in alignment with the primary care follow-up intervals within the BIO|GUARD-MI study.
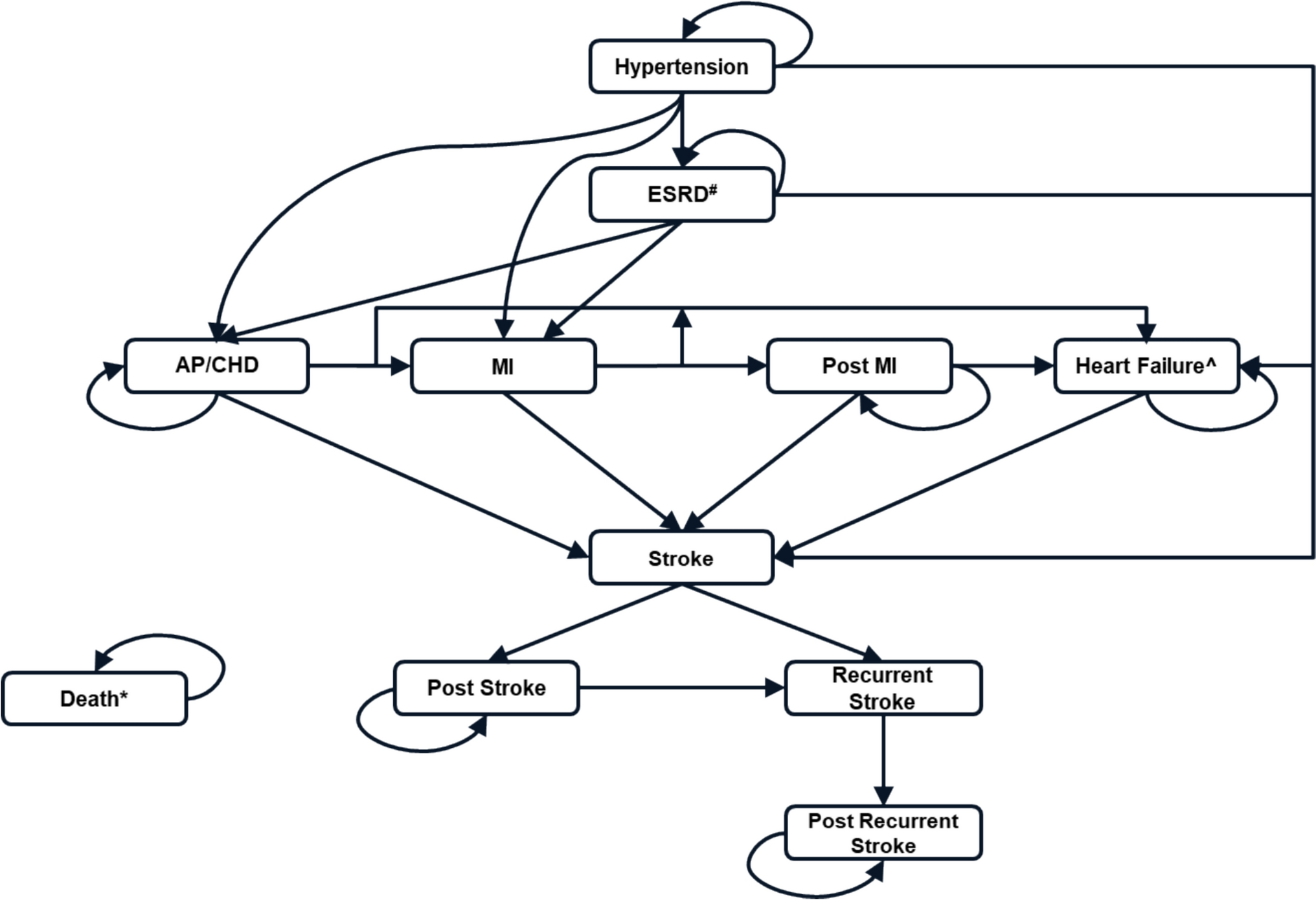
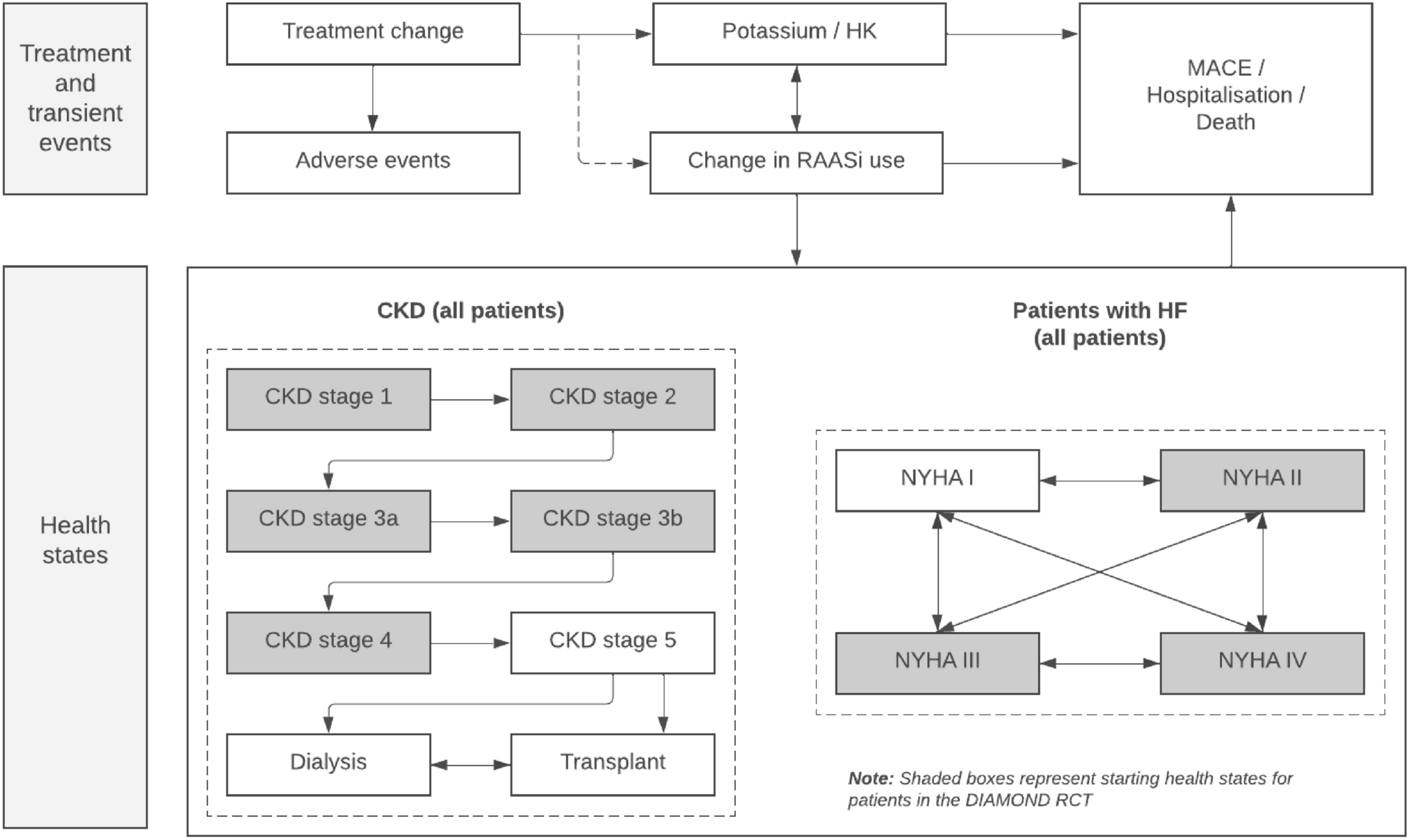
A hypothetical cohort of 1000 NSTEMI patients entered the model after the index event (MI) in the pre-MACE health state, where they were at risk of progressing to one of four MACE health states: worsening heart failure, acute coronary syndrome (ACS), stroke (ischaemic or haemorrhagic), or cardiovascular death (Fig. 1). The 6-monthly risk of a patient experiencing one of these long-term MACE was determined from survival analysis using individual patient-level data from the BIO|GUARD-MI study. The survival analysis was based upon a composite endpoint, and time-to-first MACE survival curves were not stratified by event type. Patients were separated into specific health states at the point of MACE occurrence based on distributions recorded during the BIO|GUARD-MI study to estimate the cost, mortality, and health-related quality-of-life (HRQoL) implications associated with each event. Patients residing in the pre-MACE health state were also at risk of the following short-term events: arrhythmia (requiring hospitalisation), major bleeding, and systemic embolism. A one-off cost and utility decrement was applied to patients whenever these pre-MACE events occurred.
Fig. 1
Model schematic. MACE major adverse cardiovascular events
All patients who experienced a long-term MACE (except those experiencing cardiovascular death) transitioned through a tunnel state, where they remained for one cycle only. This was to capture higher acute costs, higher mortality rates, and lower HRQoL directly after each event. Patients then transitioned to a permanent long-term post-MACE health state, where they remained until they died. It was assumed that patients could not experience more than one long-term MACE because of a lack of sufficient data available to model additional downstream events. Such assumptions have also been employed within other cardiovascular models [18, 19].
In alignment with previous modelling approaches, it was assumed that patients could not experience a short-term MACE once they had transitioned into a long-term MACE health state [19]. This conservative assumption was made because patients incur substantial costs and disutility following a long-term MACE, and any additional costs and disutilities due to the short-term MACE may double-count the consequences of such events. However, patients in the pre-MACE state could experience multiple short-term events before progression to one of the long-term MACE states.
The model conceptualisation, key assumptions, clinical extrapolations, and results were validated by a practising UK-based clinician during an individual interview. The model also underwent a rigorous internal validation process to check for calculation errors.
2.2 Model Input ParametersThe key model input parameters are provided in Table 1. This includes the aggregated costs that were applied in the model, with a detailed breakdown of these costs provided in Tables S1–S7 of Online Resource 1 (see the Electronic Supplementary Material). Data from the BIO|GUARD trial were used to inform the baseline characteristics of the modelled population, the 6-monthly probability of a short-term MACE, and the coefficients used to inform parametric survival modelling to estimate the time to first long-term MACE. Data from the BIO|GUARD-MI study were also used to inform resource use and utility inputs in a scenario analysis. A pragmatic literature search was conducted to obtain UK-specific standardised mortality ratios and utility, resource use, and cost inputs. The search was highly targeted and focused on the application of key search terms (for example, “MACE”, “utilities”, “mortality”, and “myocardial infarction”) to recognised bibliographical databases such as PubMed. Data sources were chosen based on the robustness of the underlying study (for example, study design and population size) and generalisability to the UK population. A description of the model inputs used in the base-case and scenario analysis is provided throughout the following section.
Table 1 Summary of key model input parameters2.2.1 Patient PopulationThe model cohort was set up to have the same baseline characteristics as the BIO|GUARD-MI study but was limited to NSTEMI patients. The exclusion criteria outlined that patients must not have had an indication for a CIED, permanent anticoagulation treatment, or a rare condition such as chronic renal dialysis, thrombocytopenia, or haemorrhagic diathesis. SoC within the BIO|GUARD-MI study aligned with the NICE guidelines for post-MI patients (patients would receive cardiac monitoring in hospital for approximately 24 h) [19].
2.2.2 Time to First Long-Term MACEParametric survival models were used to estimate the time to first long-term MACE within both arms of the BIO|GUARD-MI study. Altogether, six parametric functions (exponential, Weibull, Gompertz, log-normal, log-logistic, and generalised gamma) were fitted to extrapolate the observed data beyond the trial period. Statistical tests displayed that the proportional hazard assumption was not violated for any covariable included in the analysis. Therefore, one statistical model was run for the standard care arm, and an HR was applied to determine the survival curve for the ICM arm.
The Akaike information criterion, Bayesian information criterion values and graphical checks were used to determine the best fitting function to the data (as presented within Online Resource 1; see the Electronic Supplementary Material). Whilst this criterion indicated that the Weibull distribution was best fitting to the data, the long-term extrapolations were presented to a practising UK-based clinician, who confirmed that the Gompertz curve was most reflective of the average patient trajectory (i.e. a flatter curve is the most plausible option because the majority of MACE are expected to occur within 2 years of the initial MI). Figures for all extrapolations are presented within Online Resource 1, and the choice of curve was varied within scenario analyses.
The following distribution of patients after a MACE was based on data from the BIO|GUARD-MI study: 56.0% ACS (n = 65), 12.1% stroke (n = 14), 19.0% worsening heart failure (n = 22), and 12.9% cardiovascular death (n = 115). The ACS group included patients experiencing both unstable angina and MI. The distribution was assumed to be equivalent for both treatment arms because it was anticipated that the choice of intervention should not actively impact the distribution of events. However, a scenario analysis with treatment-dependent distributions was also run. These proportions were varied in the probabilistic sensitivity analysis using a Dirichlet distribution.
2.2.3 Short-Term MACEThe probabilities of experiencing an arrhythmia requiring hospitalisation, a major bleed, or systemic embolism were estimated from the BIO|GUARD-MI study. Constant probabilities were applied to all patients whilst they remained in the pre-MACE health state (i.e. before death or transition to the MACE/post-MACE health states), and distinct probabilities were applied in the two treatment arms (Table 1).
2.2.4 Arrhythmia DetectionAs observed in the BIO|GUARD-MI trial, it was assumed that the use of an ICM would increase the detection of arrhythmia. Treatment received following this detection would subsequently increase the time to first long-term MACE or prevent the occurrence of long-term MACE completely. As long-term outcomes were determined by the parametric survival models described previously, the sensitivity and specificity of the ICM were not used directly to determine the movement of patients through the model. However, the sensitivity and specificity of the device did have an indirect impact on these outcomes.
Based on data from BIO|GUARD-MI, 43.9% and 12.7% of patients in the ICM and SoC arms, respectively, experienced a change in treatment plan due to arrhythmia detection. These values were dependent on the sensitivity and specificity of each treatment arm during the duration of the study. It was necessary to make certain assumptions to incorporate these data into the model. Firstly, the distribution of patients with or without arrhythmia at baseline did not change throughout the time horizon and no further cases of arrhythmia could develop over time. Secondly, the prevalence of arrhythmia was equivalent across the two treatment arms (based on the randomisation within the BIO|GUARD-MI study). Finally, all detected cases of arrhythmia were true positives (as all episodes were adjudicated in the study).
2.2.5 MortalityThe cardiovascular deaths following MACE captured a proportion of the overall deaths in the model. Therefore, general population mortality data, based on data from the Office of National Statistics, were also incorporated [28]. Additionally, standardised mortality ratios/HRs were applied to the general population mortality rates to estimate the additional risk of death associated with each health state (see Table 1).
2.2.6 UtilitiesThe utility values used in the base-case analysis were identified through a targeted literature review, and data were obtained from two sources: the NICE guideline on ACS and an economic evaluation focusing on person-centred care for people with ACS. HRQoL data were also collected in the BIO|GUARD-MI study through the administration of the EQ-5D-5L. However, as this instrument was added to the study via a protocol amendment after commencement, only a small number of patients were available to provide utility estimates, thereby reducing the robustness of the data. Therefore, the utility data from the BIO|GUARD-MI study were used in a scenario analysis only (Online Resource 2; see the Electronic Supplementary Material).
Disutilities were applied to patients experiencing short-term MACE, as presented in Table 1. It was not possible to derive these short-term utility decrements using the BIO|GUARD-MI study data as the frequency of EQ-5D measurements was prohibitive. Therefore, these data were also identified from the targeted literature review. The disutilities for arrhythmia and systemic embolism were assumed to be incurred for 3 months, and major bleeds were assumed to impact HRQoL for 45 days [20, 23, 24].
2.2.7 CostsAll unit costs were based on the 2022/2023 cost year, and the costs were inflated to match this price year using the Hospital and Community Health Service index if the available source was pre-2022 [25].
A one-time cost was applied to patients who received the BIOMONITOR ICM device upon entry to the model. This incorporated both the cost of the device and the insertion of the device. A device removal cost was applied to patients who were still alive after the end of the BIOMONITOR battery life. It was also assumed that all patients receiving an ICM would attend a follow-up cardiologist clinic visit within the first 6 months. These costs are presented in Table 1, with more details provided in Table S1 of Online Resource 2 (see the Electronic Supplementary Material).
In alignment with NICE guidelines, patients within the pre-MACE health state were treated with aspirin (300 mg daily) combined with ticagrelor (60 mg twice daily) upon entry to the model. In alignment with clinical advice, it was assumed that patients could not receive ticagrelor for longer than 1 year. Therefore, patients received aspirin combined with ticagrelor for the first year in the model, until they experienced a long-term MACE or arrhythmia was detected. After 1 year, patients who had not experienced such events were assumed to receive aspirin only, until they experienced a long-term MACE or arrhythmia was detected. These costs are presented in Table S2 of Online Resource 2.
Patients were assumed to receive upfront procedural costs and ongoing medication changes (until long-term MACE or death) following arrhythmia detection. The proportion of arrhythmia types detected was obtained from the BIO|GUARD-MI study. Data were also available to inform the treatments received by patients following arrhythmia detection within the BIO|GUARD-MI study. However, these data were not generalisable to the UK (patients were treated across multiple countries with different treatment pathways) and, therefore, were not used in the base-case evaluation. Instead, NICE guidelines were reviewed to determine the resource use required to treat each type of arrhythmia in the UK. The resource use data were then multiplied by unit costs, identified from UK-specific sources, to determine the overall arrhythmia treatment costs (as displayed in Tables S3–S6 in Online Resource 1).
It was possible to determine the resource use incurred with short-term and long-term MACE from the BIO|GUARD-MI study. However, as with the arrhythmia treatment costs, these resource use data were not considered generalisable to the UK, and therefore, resource use and resulting event costs were obtained from UK-specific sources (as presented in Table 1).
Online Resource 2 presents a scenario in which healthcare resource utilisation for arrhythmia treatment costs, and each short-term and long-term MACE, were estimated using data from the BIO|GUARD-MI study (as presented in Tables S1–S3). The utility data from the BIO|GUARD-MI study was also used in this scenario (Table S4).
2.3 Sensitivity AnalysesDeterministic and probabilistic sensitivity analyses were undertaken to investigate first-order and second-order uncertainty, respectively. All parameters were tested in the deterministic sensitivity analysis by varying each input individually within a pre-specified range to explore the impact on the overall cost-effectiveness estimates (in terms of net monetary benefit). During the probabilistic sensitivity analysis, all parameters were varied simultaneously. The rate of short-term MACE per year and health state utility values were varied using a beta distribution. The time to first long-term MACE and health state-specific standardised mortality ratios were varied using a normal distribution. The disutility values associated with short-term MACE were varied using the gamma distribution. Parameters were varied using the 95% CI where possible. In all other cases, parameters were varied by ± 20% of the mean. In the probabilistic sensitivity analysis, a sample of 1000 iterations was used—this was enough to reach stabilisation. Scenario analyses were also performed, as described in more detail in Sects. 3.2, 3.3, and 3.4.
Comments (0)