
Remember me
A cost-effectiveness analysis was conducted to evaluate the economic impact of lecanemab combined with standard of care (SoC) compared to SoC alone for patients with early-stage AD. The SoC encompassed both non-pharmacological measures and symptom-targeted treatments, including donepezil, rivastigmine, galantamine, and memantine, as outlined in the Korean clinical practice guideline for dementia [14]. The study employed a Markov state transition cohort model to simulate AD progression and associated costs and outcomes over a lifetime horizon. The analysis was conducted from two perspectives – the healthcare payer perspective and the limited societal perspective—to comprehensively assess the economic impact of intervention [8]. One-way sensitivity analyses were performed to examine the robustness of the results. Scenario analyses were conducted by varying assumptions related to treatment initiation stage, patient demographics, and drug pricing. Our findings were reported following the guidelines of the Consolidated Health Economic Evaluation Reporting Standards (CHEERS), which are provided in Supplementary Table S1 (see the electronic supplementary material) [15].
2.2 Study CohortOur patient cohort consisted of 1000 individuals who were diagnosed with MCI or mild AD, which mirrored the characteristics of the patients who participated in CLARITY AD, a multicenter, global, randomized, placebo-controlled trial (ClinicalTrials.gov identifier, NCT03887455) [6]. The cohort, aged 71 and older, comprised 48% men and 52% women. We also assumed that 70% of the patients had MCI and 30% had mild AD, reflecting the distribution of Korean patients with AD (Table 1) [16].
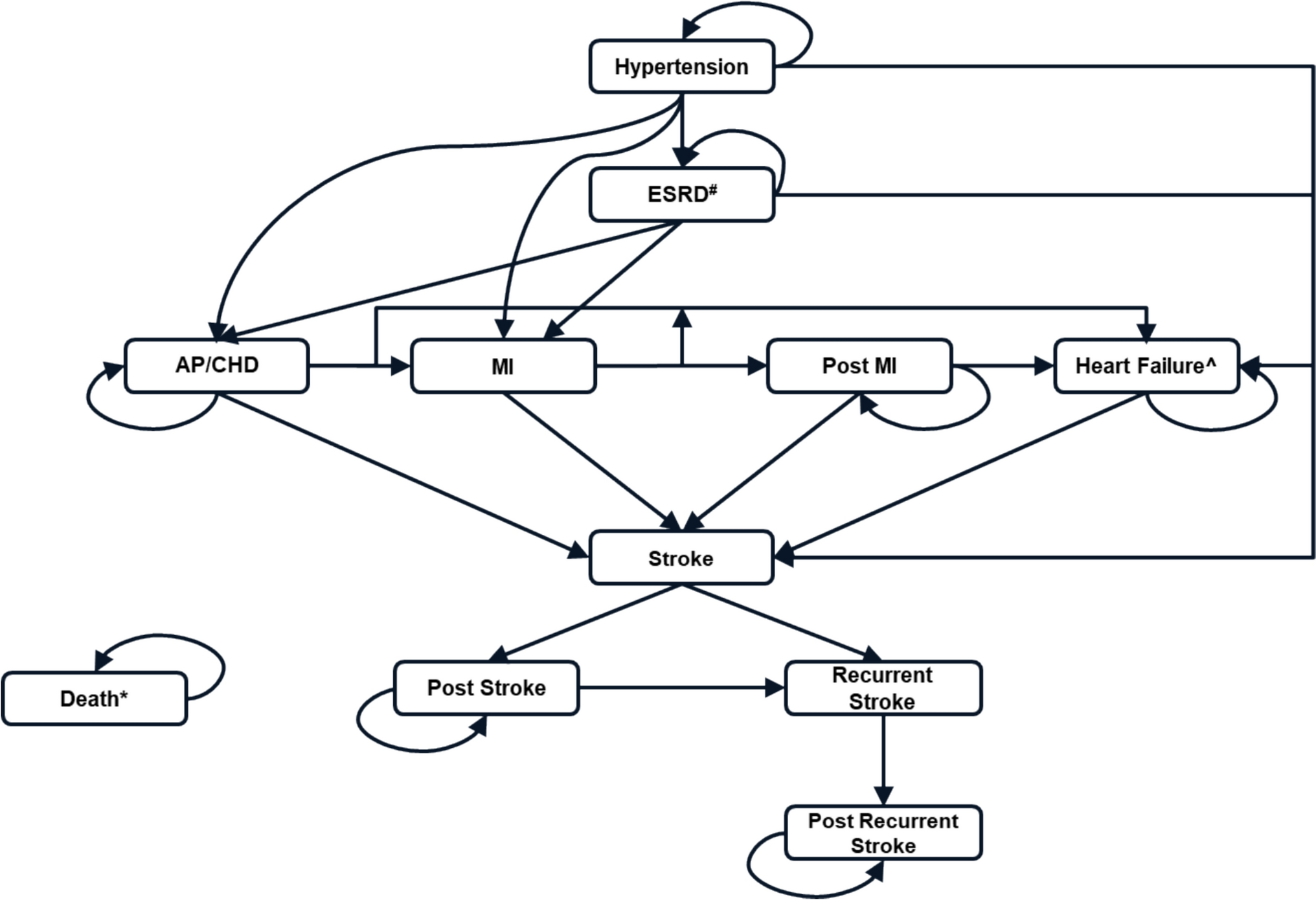
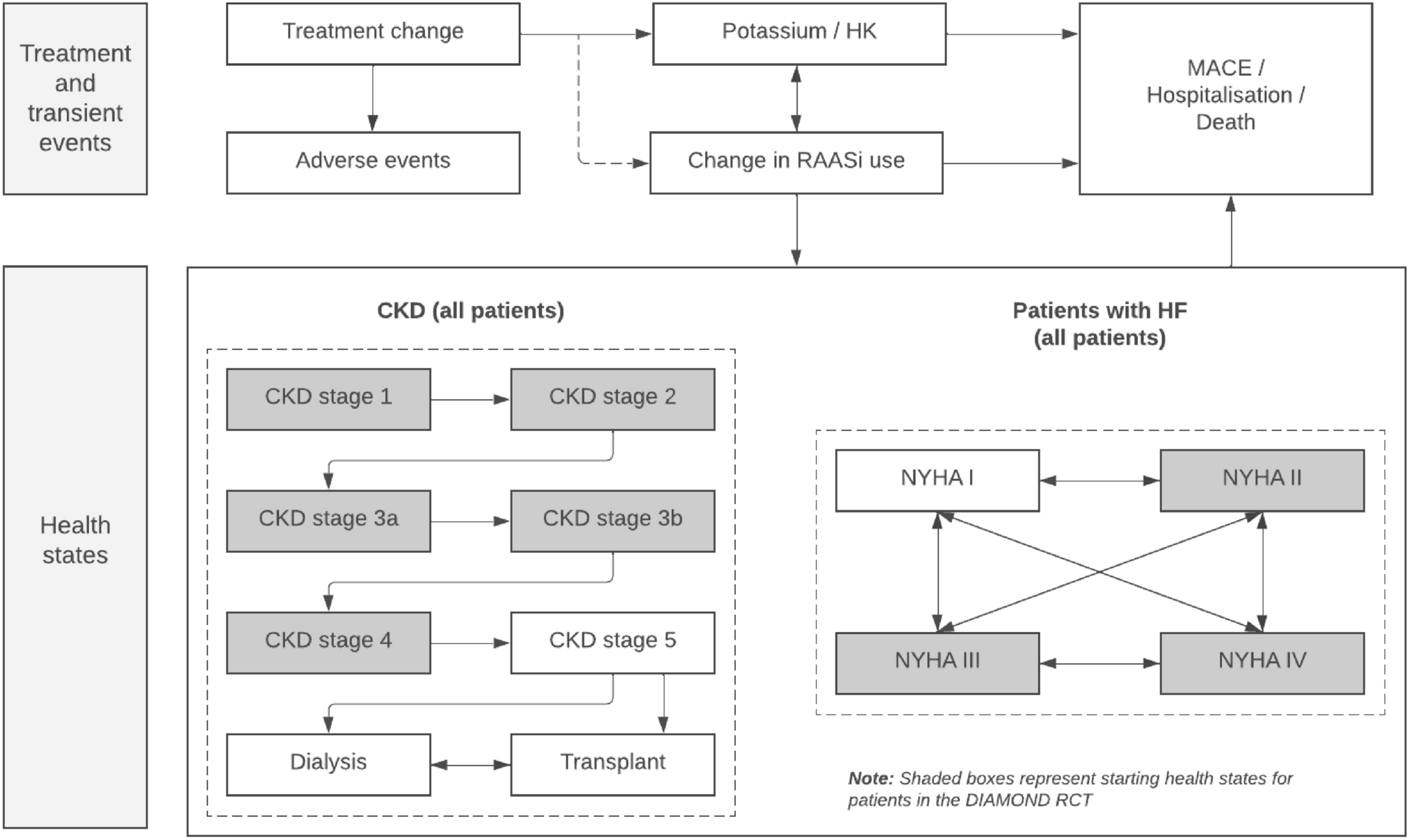
Table 1 Base-case patient characteristics and model inputs2.3 Model StructureA Markov state transition model was built for individuals diagnosed with MCI or mild AD over the patient's lifetime horizon on an annual cycle (Fig. 1). We adapted five stages of AD progression: MCI due to AD, mild AD, moderate AD, severe AD, and death, based on the previously published studies [8, 21, 22]. Each state was defined according to its Clinical Dementia Rating Sum of Boxes (CDR-SB) scoring ranges consistent with lecanemab efficacy analyses from the CLARITY AD trial: MCI (0.5–4.0), mild AD (4.5–9.0), moderate AD (9.5–15.5), and severe AD (16–18) [23]. To reflect the complexity of disease progression, our model allows transitions not only to the subsequent severity level but also to non-sequential or even less severe states under certain circumstances. Furthermore, each health state is subdivided into community and institutionalized settings. While progression from the community to an institutionalized setting is permitted, once a patient is institutionalized, transitions back to the community are not allowed. Finally, transitions to the death state are possible from any health state, in line with the natural course of AD and its associated comorbidities. We assumed that a significant portion of the patients with mild AD (95%) were initially cared for in a community care setting, while all the patients with MCI were cared for in a community setting [1]. These patients could also transition from community care to long-term care, where they remained until death. For each cycle, a half-cycle correction was used based on the Korean economic evaluation guideline [20].
Fig. 1
Markov transition model structure. Gray arrows indicate transitions between health states. AD Alzheimer’s disease, MCI mild cognitive impairment
2.4 Transition ProbabilitiesTransition probabilities between health states were derived from data provided by the National Alzheimer’s Coordinating Center (Table 2) [8]. The annual transition probabilities between health states were defined as the probability of moving from the current health state (row) to the subsequent health state (column) in each model cycle, and were conditional on patients surviving through each model cycle. The treatment effect of lecanemab, expressed as a hazard ratio (HR) for MCI or mild AD progressing to moderate AD, is set at 0.69 based on the CLARITY AD trial. The HR was reported in a prespecified, multiplicity-unadjusted time-to-event analysis evaluating progression to the next stage of AD. This indicates that lecanemab results in about a 30% reduction in the risk of progression from MCI or mild AD to moderate AD compared to SoC [8]. Regarding lecanemab’s potential to slow the progression from moderate AD to severe AD, we assumed, consistent with the Institute for Clinical and Economic Review report, that lecanemab would no longer be effective at this stage. State-specific transitions from community-based care to institutional care were obtained from a Japanese study [10]. Transitions from each health state to death were determined by state-specific HRs of mortality, which were multiplied by their respective age- and sex-adjusted mortality rates. The mortality rates were derived from life tables of the Korean population [24].
Table 2 Transition probabilities between health statesAccording to the CLARITY AD trial, patients receiving lecanemab experienced a treatment discontinuation rate of 18.8%, compared to 15.6% in patients receiving placebo during the 18-month duration [6]. Moreover, discontinuation due to side effects was higher in the lecanemab group than in the placebo group (6.9% vs. 2.9%). The 18-month discontinuation rates were converted to annual ones, e.g., a 13% discontinuation for lecanemab. Lastly, we assumed that progression to moderate AD necessitates treatment discontinuation.
2.5 Adverse EventsIn the CLARITY AD trial, lecanemab and placebo had no significant difference in resulting in death or serious adverse events (AEs) [6]. Common AEs resulting from lecanemab were infusion reactions, amyloid-related imaging abnormalities (ARIA) with cerebral microhemorrhages, cerebral macrohemorrhages, or superficial siderosis, headaches, and falls. Notably, most ARIA events were asymptomatic, emerged mainly in the first 3 months, and resolved within 4 months. Accordingly, we assumed all ARIA events occurred in the first cycle, with a 21.5% chance of any ARIA and a 3.5% chance of symptomatic ARIA.
2.6 UtilityPatient utilities, differentiated by states of AD progression and care settings (community versus institutional), were obtained from the published literature (Table 1). Utilities of patients in different care settings were derived from a cross-sectional study that collected EQ-5D-5L data from elderly patients receiving community or institutional care in South Korea [17]. Under the healthcare payer perspective, only quality-adjusted life years (QALYs) gained by the patient were considered. In contrast, the limited societal perspective accounted for QALYs gained by both the patient and informal caregivers, capturing the broader societal impact of the intervention. The limited societal perspective included disutilities of informal caregivers, which were assumed to be the same for community and institutional setting. Even after institutionalization of the patient, caregivers often continue to experience psychological distress—including guilt, anxiety, and grief— related to placing a loved one in care, concerns about disease progression, and the ongoing burden of care coordination. In countries like South Korea and Japan, cultural expectations frequently require family members to remain actively involved in caregiving tasks, such as providing meals, clothing, and personal care, as well as participating in routine care decisions. These sustained responsibilities suggest that caregiver disutility may persist even in institutional care settings [25, 26]. Assuming each patient has one caregiver, the QALYs lost due to the caregiver’s disutility were subtracted from the patient’s QALYs gained to estimate the net QALY gain [18]. All patients who experienced an ARIA event were assigned a disutility value of 0.09 for 12 weeks, which is the same disutility value associated with a mild migraine (the most common symptom of ARIA) [19].
2.7 CostsFor the healthcare payer perspective, we included drug cost, long-term care cost (formal caregiver costs), and other direct medical costs (Table 3). For patients receiving lecanemab, additional costs for drug administration and magnetic resonance imaging (MRI) monitoring were also included. The limited societal perspective included three additional cost components beyond those considered in the healthcare payer’s perspective: (1) informal care costs, reflecting the opportunity cost of caregiver time; (2) informal medical costs, such as out-of-pocket expenses for medical supplies and over-the-counter medications; and (3) direct non-medical costs, including travel time and transportation expenses for hospital visits. For patients in institutional care settings, informal care and travel-related costs were excluded under the assumption that such services are encompassed within the long-term care costs.
Table 3 Annual costs by AD stage and evaluation perspectiveAnnual treatment costs for lecanemab were estimated as 26,870,785 KRW (2022 constant KRW) based on US wholesale acquisition cost (WAC) per vial [27], considering the recommended dosage of 10 mg/kg and the average body weight of 60 kg of the Korean elderly population [20, 28]. The treatment costs included fees for drug administration and prognosis monitoring, which involved four MRI scans during the initial year [29]. In addition, patients experiencing an ARIA event were assumed to undergo a brain MRI every 4 weeks for 12 weeks, corresponding to the average duration of an ARIA event.
To estimate the direct medical costs, the study utilized the Korean NHIS claims data, which electronically document all payments made for covered healthcare services [30]. To estimate the medical costs of three AD states, each state was defined operationally based on time since diagnosis, drug usage, and long-term care levels. Direct medical costs associated with AD-induced MCI were estimated using severity-based weights from the National Dementia Annual Report, since a specific disease code was unavailable in the NHIS database [1]. Caregiving costs in an institutional setting were also identified and obtained from NHIS claims data.
We assumed that the healthcare costs of each state do not vary between community and institutional settings. Costs incurred informally in a community setting were estimated based on a recent survey in Korea that evaluated caregiver time spent caring for an AD patient [17]. Also, the costs used for the limited societal perspective were estimated from surveys reported in previous literature [17]. All costs from previous years were adjusted to 2022 KRW using the annual healthcare consumer price index published by the Korean Statistical Information Service (KOSIS). An exchange rate of 1 USD = 1320 KRW was used for reference [31].
2.8 AnalysisWe calculated the incremental cost-effectiveness ratios (ICERs) as the additional cost per QALY gained. An annual discount rate of 4.5% was applied for both costs and outcomes, following the Korean economic evaluation guideline [20]. To identify the main factors impacting cost-effectiveness, we implemented one-way sensitivity analyses. This involved changing input parameters within their uncertainty ranges to observe how these changes affected the ICERs when just one parameter was altered. We also conducted probabilistic sensitivity analyses (PSA) to account for joint uncertainty across all input parameters. The model was run for 1000 iterations, with input values randomly drawn from their respective probability distributions, in each iteration. As shown in Table 1, probability distributions were specified for all input variables with uncertainty, while constants were used for those with no variability; for cost variables (Table 3), a gamma distribution was applied to reflect their right-skewed nature. This approach enabled us to evaluate and assess the overall uncertainty in the model outcomes attributable to input parameter variability.
In addition, we conducted scenario analyses to examine the effects of different population subsets, by varying underlying assumptions on our model. Since the cost of lecanemab is not yet established in Korea, we also performed an evaluation of various price reductions. This was done to ascertain the impact that potential price adjustments might have on the ICERs relative to the base-case assumption, providing insights into how different pricing strategies could influence cost-effectiveness outcomes. We used Microsoft Office Excel (by Microsoft Corporation, Redmond, WA, USA) and SAS 9.4 for analyzing the study.
Comments (0)