
Remember me
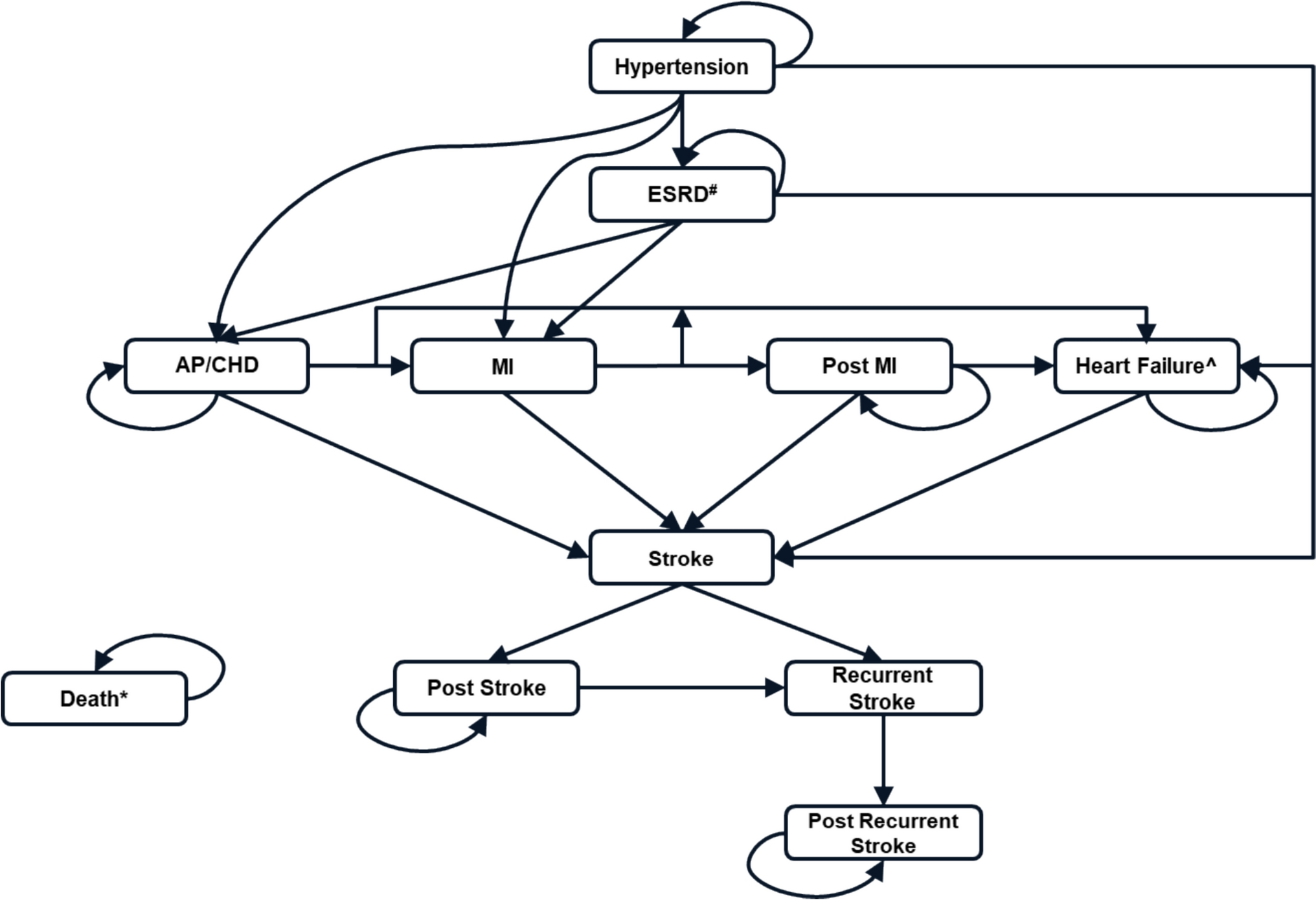
The systematic search yielded 13,228 records. Post-deduplication and title and abstract screening, 1431 records were identified, and further full texts were evaluated against the inclusion criteria. Of the 1431 screened articles, 152 were included in this study for data extraction and analysis after full-text screening (Fig. 1). After screening, only studies published in English were found to be eligible for inclusion.
Fig. 1 3.2 Summary of Included Studies
3.2 Summary of Included StudiesOf the 152 studies, 54 were published in 2023 (35.5%), 50 were published in 2022 (32.9%) and 48 were published in 2021 (31.6%). A total of 73 of 152 studies were conducted in Europe (48%), 40 studies were conducted in Asia (26.3%), 22 (14.5%) in North America, 3 (2%) in Latin American countries and 14 (9.2%) were conducted in other regions. Of the 152 studies, 35 were funded by respective governments, while 24 were funded by academic institutions. The remaining studies were either non-funded, self-funded or non-academic (funded by the pharma industries, research centres and private foundations or trusts). Cost-of-illness (COI) analysis, cost-effectiveness analysis (CEA) and cost–utility analysis (CUA) were reported in 67 (44.1%), 66 (43.4%) and 22 (14.5%) studies, respectively. More than one method for economic evaluation was utilised in 11 (7.2%) studies. A societal perspective was adopted in 68 (44.7%) of all the studies, while a healthcare and societal perspective was adopted in 31 (20.4%) studies. Of the 152 evaluated studies, 118 (77.6%) reported productivity loss measures for patients only, 14 (9.2%) included measures for caregivers and 20 (13.2%) included measures for both patients and caregivers. Productivity measures were assessed mostly in patients with mental, behavioural or neurodevelopmental disorders (16.4%), followed by cancer (11.2%), diseases of the musculoskeletal system or connective tissue (9.9%), diseases of the nervous system (8.6%) and certain infectious or parasitic diseases (7.2%). Across all therapeutic areas, most of the studies covered both genders and adult patients (Electronic Supplementary Material Table S5).
Of the 152 studies analysed, 97 studies utilised instruments reporting absenteeism as a productivity component, whereas presenteeism was utilised in 70 studies. While most of the studies considered absenteeism and presenteeism of the patients, only the Zarit Burden Interview considered unpaid care given by the caregiver [26]. Various forms of hourly wages were utilised as a labour measure in 29 studies, while daily wages were used in 19 studies. Weekly, monthly and annual wages were also considered as labour measures.
Table 1 provides an overview of the included studies with details about year of publication, region, funding source, therapeutic area, economic analysis type, population type and study perspective.
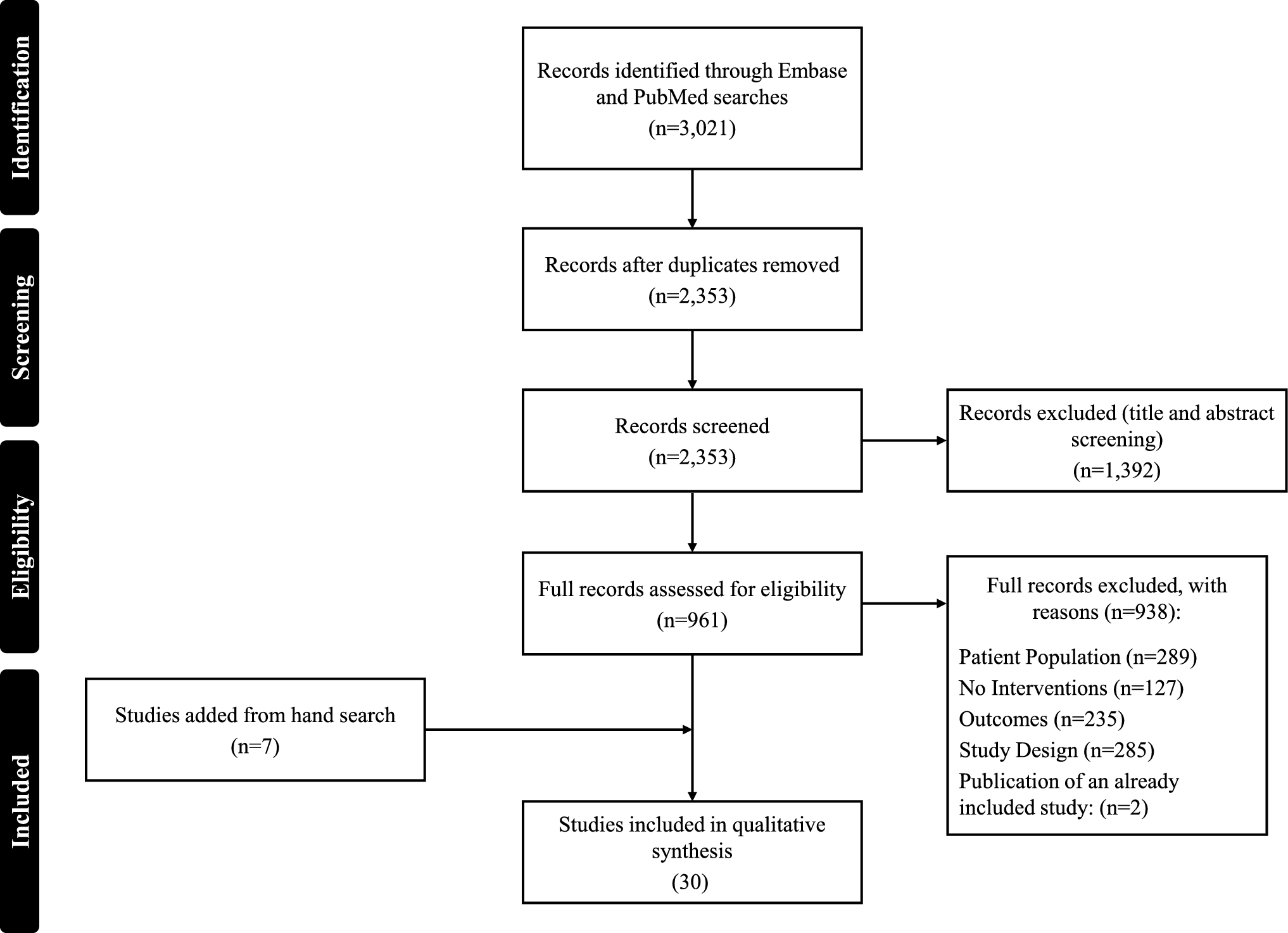
Table 1 Distribution of included studies by year of publication, region, funding source, therapeutic area, economic analysis type, population type and study perspective3.3 Selection of InstrumentsIn the 152 studies, 88 instruments or questionnaires were identified to assess productivity measures (Electronic Supplementary Material Table S6). Of the 88 instruments, 20 were included in the analysis of this study, while 68 were excluded. Of the included instruments, 12 were included as these were utilised in more than one study, while eight were included despite being used only in one study each owing to their practical relevance.
Of the excluded instruments, 44 were categorised as ‘research-specific questionnaires’, which were developed by researchers for specific studies, and 20 instruments, which were not named instruments and reported in only one study, were excluded. The remaining four instruments were used in literature/database analysis.
Figure 2 provides the selection of instruments for analysis.
Fig. 2
Distribution of instruments identified in the selected studies
3.4 Summary of Included InstrumentsOf the included instruments, the Work Productivity and Activity Impairment Questionnaires (WPAI) (23 studies; 15.1%) [WPAI—no version specified (8; 11.8%); WPAI General Health (WPAI-GH) (6; 3.9%); WPAI Specific Health Problem (WPAI-SHP) (6, 3.9%); WPAI: chronic obstructive pulmonary disease (COPD)-specific, asthma-specific and Crohn’s disease (CD)-specific (each 1; 0.7%)] were the most utilised. For this analysis, all WPAI instruments were considered and analysed as a single instrument, irrespective of generic or disease-specific ones. Institute for Medical Technology Assessment (iMTA) Productivity Cost Questionnaire (iPCQ) was another of the most commonly used instruments (23; 15.1%), followed by the Trimbos/iMTA Questionnaire for Costs Associated with Psychiatric Illness (TIC-P) (8; 5.3%). In total, 13 out of 20 are generic instruments, while the rest (7) are disease-specific instruments. The mode of administration was self-reported by ‘patient’ for 16 instruments and by both ‘patient and caregiver’ for two instruments [Client Service Receipt Inventory (CSRI) and Health Diary]. Patient market (absenteeism and presenteeism) and non-market productivity loss and informal caregiver time were the productivity components utilised for WPAI, iPCQ, TIC-P and Health and Labour Questionnaire (HLQ). Most instruments (WPAI, iPCQ and TIC-P) utilised hourly wages as the labour measure for evaluating the productivity loss. Additionally, iPCQ and TIC-P also use daily wages as a labour measure. The human capital approach is the most utilised method for valuation for the instruments. The recall period of all included instruments in the study ranged between 7 days and 6 months.
Detailed characteristics of all included instruments are summarised in Table 2, and the distribution of use of the productivity component and valuation method are in Electronic Supplementary Material Figs. S1 and S2, respectively.
Table 2 Characteristics of instruments identified3.5 Characteristics of the Most Frequently Used InstrumentsDetailed characteristics of the most frequently used instruments (WPAI, iPCQ and TIC-P) are summarised below.
3.5.1 Work and Productivity, Activity, Impairment QuestionnaireThe WPAI was created in 1993 by Reilly Associates as a patient-reported quantitative assessment of the amount of absenteeism, presenteeism and daily activity impairment attributable to general health (WPAI-GH) or a specific health problem. This instrument has been validated to quantify work impairments multiple times and in numerous therapeutic areas. The main questionnaire was validated in 1993, the WPAI-CD was validated in 2008 and the WPAI-GH was validated in 2010 [27,28,29,30]. Additionally, the instrument has been translated and validated in multiple languages; as many as 113 translations of the generic version are available [27, 28]. The recall period for WPAI is 7 days and can be used by either patients or caregivers. WPAI utilises both the human capital approach and the friction cost method for the valuation of lost productivity. The underlying theory and concepts of work productivity loss (absenteeism and presenteeism) apply to people with health problems (i.e., patients) and caregivers when measuring their work productivity loss.
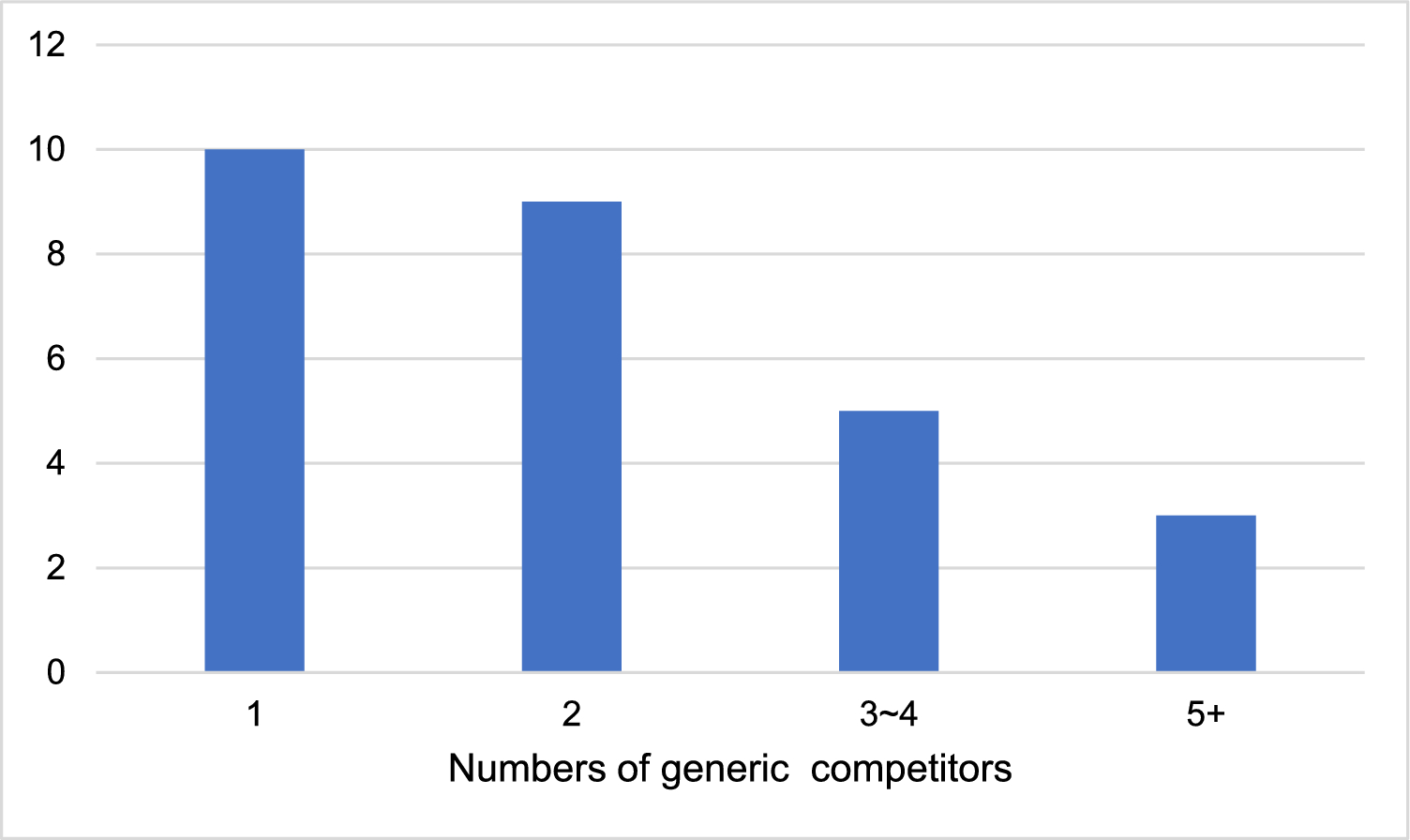
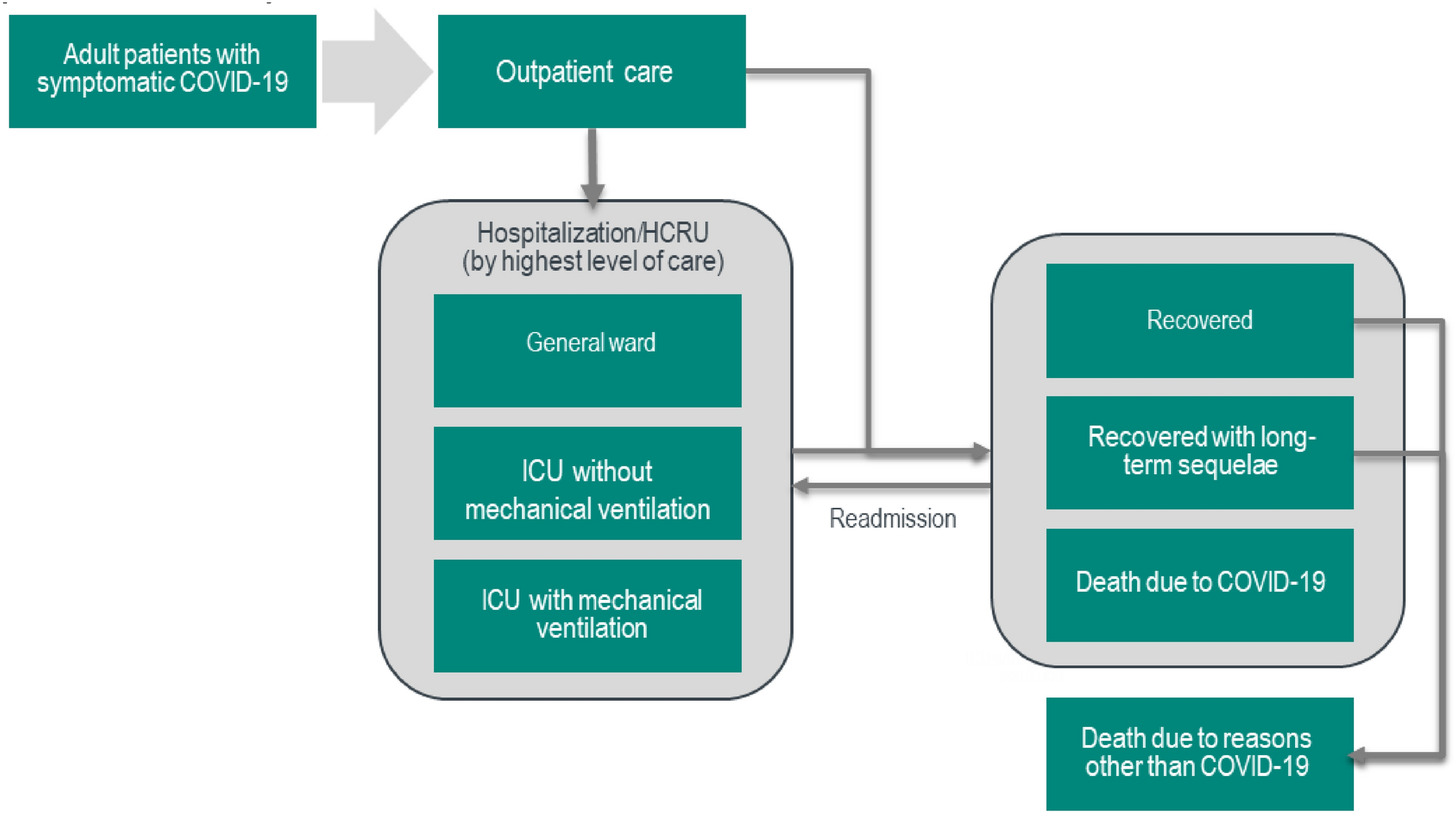
Of the 23 studies where this instrument was used, 10 were published in 2023, while 9 and 4 were published in 2022 and 2021, respectively. In total, eight studies were from Europe, while seven and five were from North America and Asia, respectively (Fig. 3). A total of 4 studies utilised CEA, 16 utilised COI and 2 utilised CUA. WPAI is adopted in all age groups.
Fig. 3
Distribution of instruments by number of studies and region of study. CD Crohn’s disease, COPD chronic obstructive pulmonary disease, iMTA institute for Medical Technology Assessment, TB tuberculosis, WHO World Health Organisation
3.5.2 iMTA Productivity Cost Questionnaire (iPCQ)iPCQ is a generic questionnaire developed by the Institute for Medical Technology Assessment, Netherlands, and published in 2014. The instrument has been translated into 18 languages. It comprises 18 components and utilises eight core items to calculate productivity costs [29]. Questions from preexisting validated questionnaires were optimised in the iPCQ for measuring presenteeism and absenteeism [30]. The questionnaire has also been validated [31]. The questionnaire comprises 18 questions. Of these, nine are general questions to collect demographic information, and the remaining questions measure productivity losses such as patient market and non-market productivity loss and/or informal caregiver time [30]. The recall period of iPCQ is 4 weeks, and it utilises both the human capital approach and the friction cost method for the valuation of lost productivity. iPCQ is a primarily patient-reported instrument. However, in this review, the questionnaire was utilised by caregivers in one study, though the same questionnaire was used [32].
Similar to the WPAI, iPCQ was another most utilised instrument to measure productivity in the 3-year span. Of the 23 studies where this instrument was used, 7 were published in 2023, while 6 and 10 were published in 2022 and 2021, respectively. A total of 21 studies were from Europe, whereas 2 were from North America (Fig. 3). In total, 14 studies utilised CEA, 5 studies utilised COI and 9 utilised CUA. iPCQ is adopted in both adult and elderly participants.
3.5.3 Trimbos/iMTA Questionnaire for Costs Associated with Psychiatric Illness (TIC-P)The TIC-P, also called Treatment Inventory of Costs in Patients with Psychiatric Disorders, was also developed by the Institute for Medical Technology Assessment, Netherlands, in 2013 and is a mental illness-specific questionnaire and patient-reported instrument. The iPCQ is an integral part of this questionnaire. This instrument is available in 11 languages, and a special parent version is also available to assess costs related to mental illnesses in children [33, 34]. TIC-P has been found to be a feasible, reliable and valid instrument for collecting productivity-related data in patients with mild-to-moderate mental health problems [35]. This questionnaire comprises a total of 36 components, and productivity components represent losses from patient market and non-market productivity loss and/or informal caregiver time. The recall period of TIC-P is 3 months, and it utilises both the human capital approach and the friction cost method for the valuation of lost productivity.
TIC-P reported its usage in eight studies, of which three were published in 2023 and 2021, while two were published in 2022. Of the eight studies, seven were from Europe, while the remaining study was from North America (Fig. 3). A total of five of the eight studies utilised CEA, while one and two studies utilised COI and CUA, respectively. TIC-P is widely used in adults.
Components and methods of calculation of these instruments are included in Electronic Supplementary Material Table S7.
Of the 12 remaining instruments, 7 utilised absenteeism as a productivity component, whereas presenteeism was utilised by 6 instruments. Work time loss was considered by six, while patient non-market productivity loss and/or informal caregiver time was considered by three instruments. Of these 12 instruments, 4 utilised the human capital approach for valuation, and the friction cost and opportunity cost approaches were utilised by 3 instruments each.
Comments (0)