Mpox virus (MPXV), a zoonotic orthopoxvirus historically endemic to Central and West Africa, was primarily associated with sporadic outbreaks linked to zoonotic transmission in countries such as the Democratic Republic of Congo, where thousands of suspected cases are reported annually, along with Nigeria, Cameroon, the Central African Republic, and the Republic of Congo. In these regions, human infections typically arose from contact with infected wildlife, such as rodents and non-human primates, with limited secondary transmission occurring within households and local communities. A marked shift in the epidemiological pattern of Mpox occurred in May 2022, when the first cases of a multi-country outbreak were identified in the United Kingdom, Portugal, and Spain. In contrast to prior outbreaks, these cases showed no epidemiological link to endemic regions or known zoonotic exposure, indicating sustained human-to-human transmission. Within a matter of weeks, the virus disseminated rapidly across Europe and North America and subsequently reached South America, Asia, Oceania, and the Middle East. By July 2023, over 108 countries had reported confirmed cases, many for the first time, signaling a global expansion of the virus far beyond its traditional geographic boundaries [1,2,3,4].
The virus is primarily transmitted through close contact with infected individuals, including sexual contact, and exposure to contaminated materials and respiratory fluids [1, 3, 5, 6]. Since May 2022, most cases have occurred among gay, bisexual, and people living with HIV (PLWH), and other men who have sex with men [1, 4, 7, 8], highlighting the significant role of sexual transmission in its spread.
In fact, previously, mpox infection was primarily diagnosed after contact with infected animals or travel to endemic regions. However, in the recent outbreaks, most cases are linked to sexual contact between individuals rather than animal exposure or travel history [6]. Furthermore, MPXV can silently circulate, as previously observed and confirmed by serological testing and retrospective polymerase chain reaction studies [7, 9]. Since 2022, reported mpox cases have persisted at a low but steady frequency, indicating the ongoing circulation of MPXV and the need to include it in sexually transmitted infection screening tests [10,11,12].
Common symptoms include fever, headache, muscle pain, swollen lymph nodes, and a characteristic rash that progresses through various stages [1, 8].
Virological and Epidemiological Brief Overview of MPXV
MPXV is a member of the Orthopoxvirus genus in the Poxviridae family. It is a large, double-stranded DNA virus measuring approximately 197 kb, which includes a conserved core region and a variable region [6, 13]. Like other orthopoxviruses, MPXV possesses a complex envelope structure and replicates entirely within the cytoplasm of host cells, bypassing the nuclear machinery.
There are two major genetic clades of MPXV; they differ by 0.5% in genomic sequence [13]. Clade I (formerly Central African or Congo Basin clade) is more virulent and associated with higher human-to-human transmission and mortality rates (10%) [13]. Clade II (formerly West African clade) is less virulent, with a lower fatality rate (< 1–3%) [13]. Phylogenetic analyses from 2022 to 2023 identified subtypes within clade 1 and clade 2. Clade 1a dominates Central Africa, while clade 1b, discovered in 2023, emerged in the eastern Democratic Republic of Congo. Clade 2a circulated in West Africa until Nigeria’s 2017 outbreak, where clade 2b became dominant. The 2022 global outbreak led to further divergence of clade 2b into two lineages, with clade 2b A, which had been prevalent in Nigeria in 2017, and clade 2b B.1, which became the dominant strain during the 2022 global outbreak and was mainly associated with sexual contact transmission [14]. More in-depth analyses revealed that the virus responsible for the 2022 outbreak is not a recent introduction but descends from strains that had already been circulating since 2017–2018 [15]. Notably, the virus has undergone significant genetic changes, with G > A mutations likely caused by the human APOBEC3 enzyme, which edits viral genomes, evolving for more efficient human transmission [15, 16]. These genetic changes were also observed for Clade 1b [16]. Whole-genome sequencing has revealed mutations associated with increased adaptation to human hosts [17].
By 2024, mpox cases had increased in some areas of the Democratic Republic of Congo, primarily due to the spread of clade 1b [14, 16]. Sexual contact was identified as a significant mode of transmission, and the virus expanded into previously non-endemic areas, including Rwanda, Uganda, Kenya, and Burundi [14, 16]. A novel Clade III was proposed, identified following the 2022 European outbreak [18].
The nucleotide sequences encoding enzymes and structural proteins of the MPXV genome were 96.3% identical to those of the variola virus. Still, they differed in the terminal regions, where most virulence genes are located [13]. Genome analysis of MPXV revealed that genes responsible for DNA replication, recombination, repair, virion structure, and morphogenesis are typically located in the conserved regions. In contrast, genes related to host interactions are found in the variable regions [17]. Variable region mutations contribute to our understanding of the evolution and host adaptation of MPXV [17]. Tandem repeat sequences, usually located in the variable region, have reduced over the years, resulting in a lower length in the clade IIb [17]. The gene with the highest single-nucleotide polymorphism density was Kelch repeat and BTB domain-containing protein 2, located in the variable region. Only poxviruses contain Kelch-like protein genes. These proteins can inhibit NF-κB signaling pathway [17].
Replication, Host Interaction, and Immune Evasion
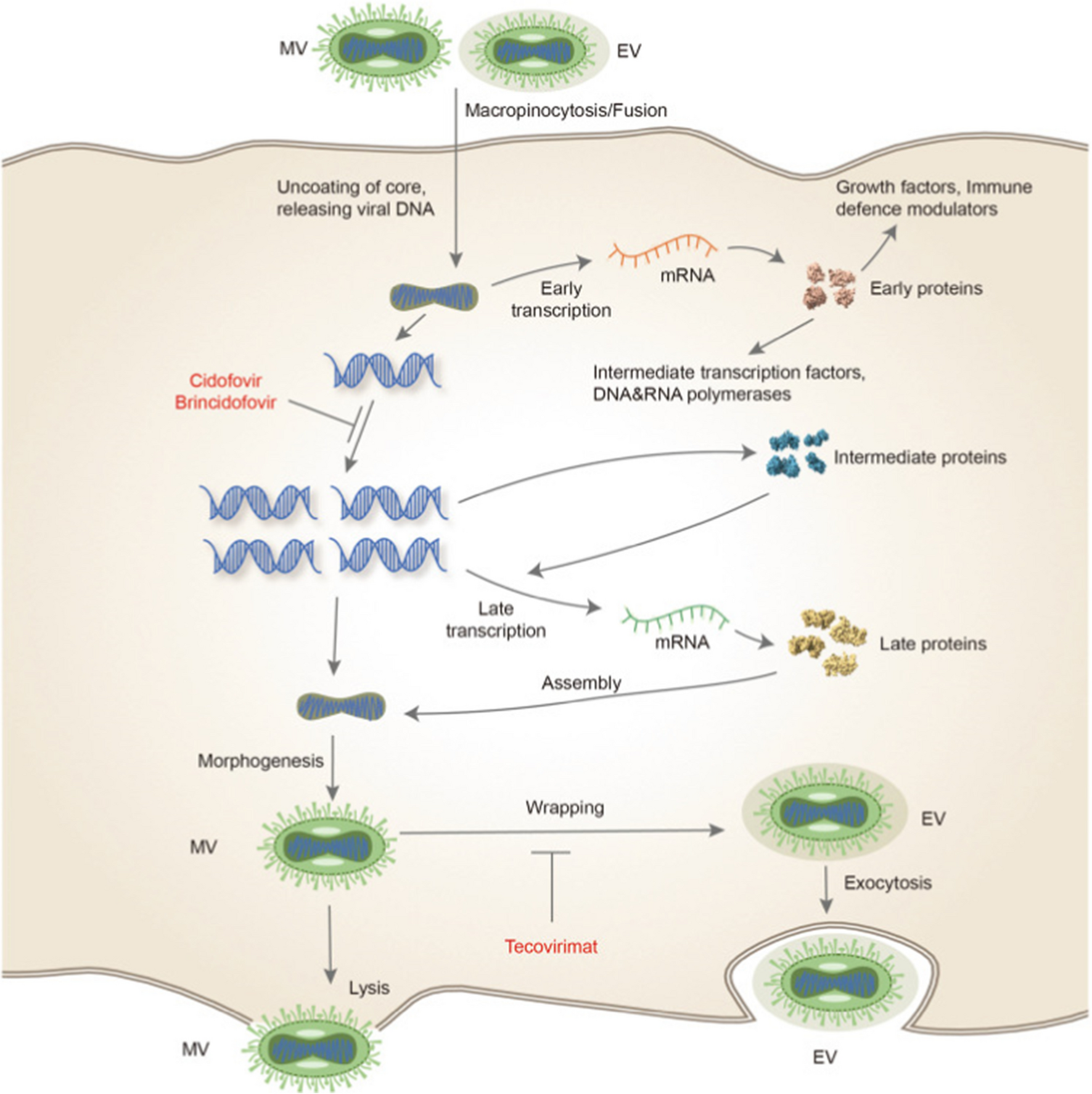
The MPXV infection and replication process occurs in multiple, well-defined stages: virus entry, uncoating, replication, gene expression, assembly, maturation, and release [6].
Unlike many DNA viruses, MPXV completes its entire replication cycle in the cytoplasm of the host cell, independent of the nuclear machinery [6].
The process begins when MPXV binds to unidentified surface receptors on host cells and is internalized via endocytosis or direct membrane fusion. Entry is facilitated by lipid rafts, cholesterol-rich microdomains in the plasma membrane. Cholesterol plays a central role in maintaining the structural integrity of these rafts. Consequently, drugs such as amphotericin B, statins, and PCSK9 inhibitors may exhibit antiviral effects by disrupting lipid raft function and depleting membrane cholesterol, thereby impairing viral entry [6]. Once inside the cell, the virus is transported along microtubules toward the perinuclear region. During this journey, it undergoes uncoating, releasing its large, linear, double-stranded DNA genome into the cytoplasm. MPXV brings with it a complete transcriptional machinery, including a DNA-dependent RNA polymerase, which allows immediate transcription of early genes. This independence from the host nucleus is a hallmark of poxviruses [6]. Central to the viral replication machinery is the DNA polymerase holoenzyme, composed of the F8 polymerase and two associated processivity factors, A22 and E4. These proteins form a stable complex that ensures efficient and continuous DNA synthesis by maintaining the polymerase’s attachment to the DNA strand, functioning analogously to a “forward sliding clamp” [19].
Following genome replication and viral gene expression, structural proteins are synthesized and assembled in cytoplasmic viral factories. Newly formed virions initially acquire a single membrane from the endoplasmic reticulum, forming the Intracellular Mature Virus (IMV). IMVs can remain intracellular or be released through cell lysis. Some IMVs undergo an additional wrapping process in the Golgi apparatus or endosomal membranes, leading to the formation of the Extracellular Enveloped Virus (EEV), which possesses two or more membrane layers [6].
The EEV form is transported in vesicles to the plasma membrane and released via exocytosis, enabling the virus to spread cell-to-cell without triggering host cell lysis. This form is more efficient at immune evasion and dissemination due to its additional membrane layers, which shield key viral antigens from neutralizing antibodies. In contrast, IMVs, which are more environmentally stable and released upon cell lysis, are more susceptible to complement activation and antibody neutralization due to their exposed surface proteins [6].
MPXV employs multiple immunomodulatory strategies to evade host defenses. It inhibits interferon signaling, cytokine production, and apoptosis by targeting key pathways like NF-κB, MAPK, and JAK/STAT, impairing T cell activation. It also modulates EGFR signaling to promote cell proliferation and viral dissemination. Proteomic analyses show post-transcriptional downregulation of pro-apoptotic proteins and altered phosphorylation patterns affecting RNA processing and cell survival. Notably, MPXV suppresses AKT signaling, unlike other poxviruses, indicating a distinct replication strategy. These mechanisms support immune evasion, replication, and differences in virulence among MPXV clades [18, 20,21,22].
Pathogenesis
Unlike variola virus, MPXV is not limited to humans and can infect a wide range of hosts, including rodents and primates. After exposure to respiratory secretions or bodily fluids of mpox patients, the virus enters through mucous membranes (ocular, respiratory, oral, urethral, and rectal) or broken skin, spreading via tissue-resident immune cells and lymph nodes during the latent period [6, 23]. In the respiratory tract, MPXV primarily infects airway epithelial cells, while in the skin, it targets keratinocytes, fibroblasts, and endothelial cells, leading to productive and cytopathic infection. Additionally, antigen-presenting cells such as macrophages, dendritic cells, and Langerhans cells undergo abortive infection, allowing them to survive long enough to transport viral antigens to draining lymph nodes, potentially contributing to immune activation and systemic spread [23]. After initial replication in the lymph nodes, which leads to a low-grade primary viremia, the MPXV can spread to larger organs, including the spleen and liver, where it undergoes amplification. This results in a second major viremia wave, which enables the virus to disseminate further to distant organs such as the lungs, kidneys, intestines, and skin [23]. Finally, the virus is detected in the blood on day 8, with viral concentrations increasing until day 10, accompanied by widespread skin lesions and involvement of mucous membranes. Ulcerating lesions in the mouth and pharynx release large quantities of virus particles, which are then disseminated through respiratory droplets, facilitating further transmission [23]. Infected individuals initially develop prodromal symptoms such as fever, chills, headache, myalgia, and lymphadenopathy, typically lasting three days. This is followed by the onset of rash, which in the current outbreak often begins in the genital or anal region before spreading more widely [6].
New Mpox Disease: Clinical Features
Nowadays, mpox is primarily observed in men who have sex with men. High-risk sexual behaviors, such as having multiple sexual partners, have been identified as potential risk factors for transmission [24, 25]. Most of the confirmed mpox cases have been found in PLWH [8, 24]. The incubation period of mpox is approximately 7–14 days, with symptoms typically lasting 14–21 days [6]. Instead, in PLWH Eser-Karlidag et al. showed that the duration between exposure and onset of symptoms was 6.5 (2–21) days in those with CD4 > 200, and 3 (2–6) days in those with CD4 < 200 [8].
Mpox usually causes systemic symptoms followed by skin lesions. Skin lesions are well-circumscribed and present a central umbilication, typically resting on an erythematous base. In some cases, the lesions may appear greyish [12, 26,27,28]. The lesions are deep-seated, rigid, and range in size from 2 to 10 mm [16]. The skin lesions can persist for weeks and progress through several stages, beginning as small macules that evolve into papules, vesicles, and eventually pseudo-pustules [12, 24]26– [28]. They persist in the pustular stage for 1 week before crust development occurs and resolve 3–4 weeks following the commencement of symptoms [16]. The main differential diagnoses include lymphogranuloma venereum, syphilis, genital herpes recurrence, molluscum contagiosum, and pustules associated with scabies [29, 30].
Unlike the endemic African variant, which is characterized by widespread lesions across the body, the non-endemic variant generally presents with fewer lesions, typically localized to sexually exposed areas, such as the external genitalia, perianal, and labial region [12, 25,26,27,28]. These lesions are often painful [12, 26,27,28] and bacterial superinfection of the skin is a common complication [28]. Lesion-free cases have also been reported [31]. Other common manifestations include proctitis [31], presenting with severe pain and pharyngitis, including white ulcerative and other lesions [32, 33]. Penile edema is another possible clinical feature [25].
Significant inguinal lymphadenopathy is often observed in mpox cases. This clinical feature can help differentiate mpox infection from other orthopoxvirus infections [6].
In rare cases, systemic forms with multiorgan involvement, including brain, bone marrow, and esophagus, have been described, which can result in fatal outcomes [34]. Severe manifestations of mpox include ocular infections, neurologic complications, myopericarditis, and complications associated with mucosal lesions in areas such as the oral, rectal, genital, and urethral regions [35]. A meta-analysis reported a pooled prevalence of ophthalmic manifestations of 9%, although Studies from Europe reported a very low prevalence of ocular manifestations (0.98%), compared to studies from Africa with a higher prevalence (27.22%) [36].
However, most MPXV infections are self-limiting, with 1–13% of patients requiring hospitalization for either treatment or isolation. The case-fatality rate remains low, at less than 0.1% [23]. In a multicenter Italian cohort, a multivariable analysis showed that severe mpox was more likely in Caucasians and patients with the onset of fever, lymphadenopathy, sore throat, and perianal lesions [37].
Diagnosis
Diagnosis of Mpox relies primarily on nucleic acid amplification techniques, particularly PCR and real-time PCR, conducted on lesion samples [38, 39]. For improved sensitivity, simultaneous sampling from multiple anatomical sites, including skin, oropharyngeal, anal, rectal swabs, urine, semen, and blood, is recommended [38, 40]. Blood testing is especially useful in early infection stages due to transient viremia [38]. However, standard PCR assays may not differentiate MPXV from other orthopoxviruses, necessitating the use of specific genetic targets such as the A-type inclusion body protein gene [38,




Comments (0)