This retrospective analysis was conducted using the electronic medical record system of our institution. Patients diagnosed with sarcoma who initiated PAZ treatment at our hospital between November 1, 2012 and January 31, 2020, were included in this study. Medical records were reviewed up to March 30, 2023, as the final date of data collection.
Patient background factors such as height, weight, age, sex, body mass index (BMI), diagnosis, disease stage, recurrence status, treatment history, PAZ dosage and timing of administration, concomitant use of PPIs or H2RA, use of cytochrome P450 (CYP) 3A4 inhibitors (ketoconazole, itraconazole, clarithromycin, ritonavir, voriconazole) or inducers (rifampin, carbamazepine, phenytoin), presence of gastrointestinal disorders, Eastern Cooperative Oncology Group performance status (PS), and histological classification were collected from the electronic medical records.
Information on the concomitant use of PPIs or H2RAs was obtained from prescriptions recorded in the hospital’s electronic medical records, which include all inpatient and outpatient medications prescribed within the institution. Medications brought in by patients at the time of hospital admission (i.e., self-medicated or prescribed at another institution but confirmed during medication reconciliation) were also reviewed and included when available. However, over-the-counter (OTC) medications that were not recorded in the medical records were not captured in this analysis.
Although height, weight, and BMI are interrelated variables, they were analyzed individually to identify any potential differences in baseline characteristics between groups.
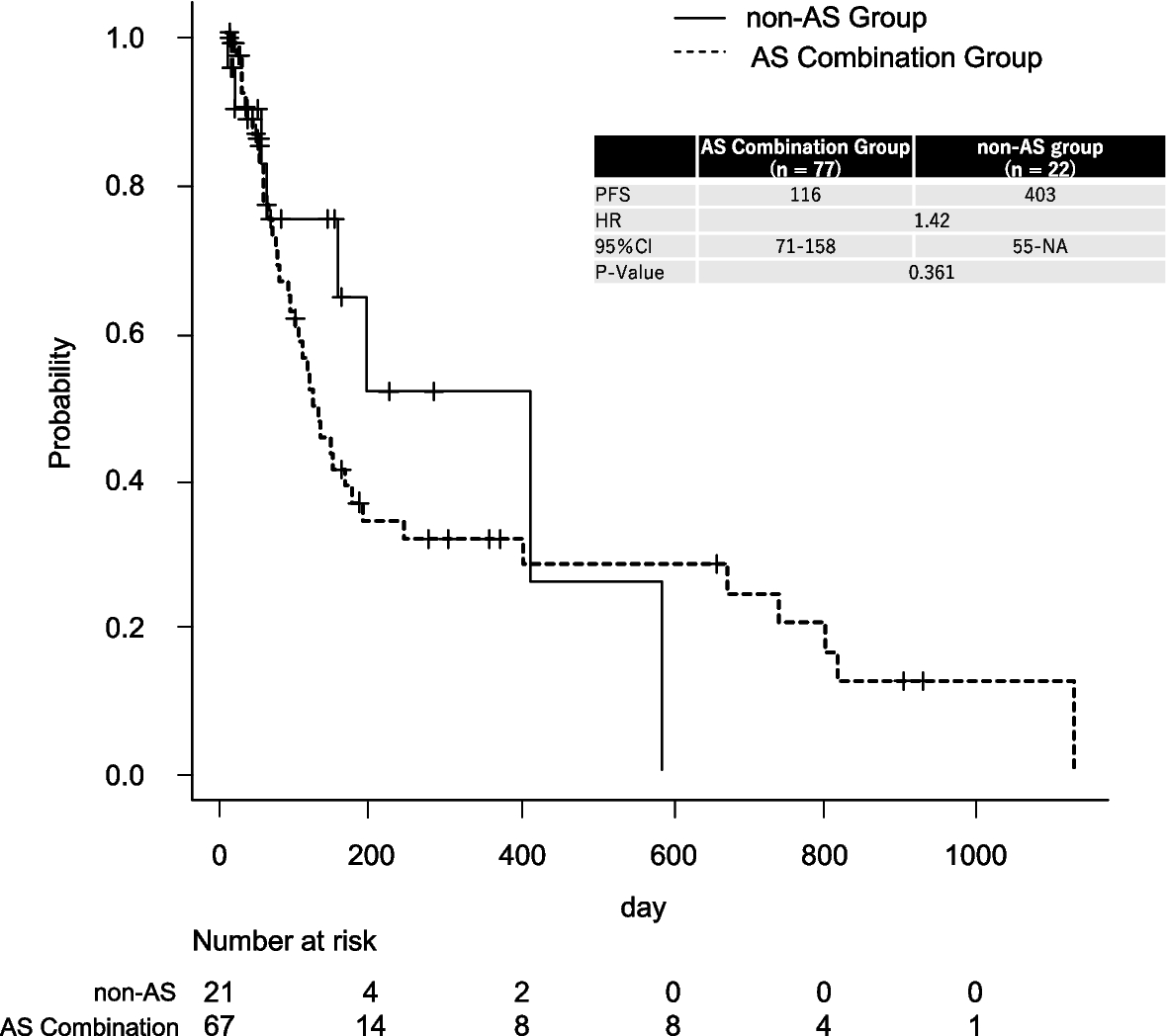
The primary endpoint was PFS of patients whose treatment comprised PAZ and AS (AS combination group) and that of patients whose treatment comprised PAZ alone (non-AS group).
The secondary endpoint was treatment safety, which was evaluated by analyzing AEs related to PAZ. For this purpose, AEs were classified into two categories based on clinical relevance and the PAZ drug label: serious AEs potentially associated with PAZ, and gastrointestinal toxicities. The following events were designated as serious AEs associated with PAZ, based on known safety concerns described in the Japanese package insert and prior literature: Liver failure, Aspartate Aminotransferase (AST) increased, Alanine Aminotransferase (ALT) increased, blood bilirubin increased, Gamma-Glutamyl Transferase (GGT) increased, hypertension and hypertensive crisis, left ventricular systolic dysfunction, QT corrected interval prolonged, ventricular arrhythmia, cardiac troponin I increased, angina pectoris, ischemic stroke, transient ischemic attacks, myocardial ischemia, venous thrombosis, pulmonary embolism, cerebral hemorrhage, hemoptysis, gastrointestinal bleeding, hematuria, bronchopulmonary hemorrhage, epistaxis, gastrointestinal perforation, gastrointestinal fistula, thyroid dysfunction, nephrotic syndrome, proteinuria, infectious diseases, delayed wound healing, interstitial pneumonia, thrombophilia, reversible posterior leukoencephalopathy syndrome, pancreatitis, retinal detachment, hair color changes, palmar-plantar erythrodysesthesia syndrome, gastric ulcer, duodenal ulcer, reflux esophagitis, acute and chronic gastritis. In addition, gastrointestinal toxicities were examined separately as clinically relevant endpoints because of their frequency and potential impact on treatment continuity. The following symptoms were included: Reflux esophagitis, acute and chronic gastritis, nausea, vomiting, diarrhea, and stomach pain. Each adverse event included in the analysis was mapped to its corresponding Preferred Term in the Common Terminology Criteria for Adverse Events (CTCAE), version 5.0, to ensure standardized and reproducible classification. The following events were identified and evaluated using their CTCAE-defined terms: Liver failure, aspartate aminotransferase increased, alanine aminotransferase increased, blood bilirubin increased, hypertension, ejection fraction decreased, electrocardiogram QT corrected interval prolonged, ventricular arrhythmia, cardiac troponin I increased, stroke, transient ischemic attacks, arterial thromboembolism, laryngeal hemorrhage, upper gastrointestinal hemorrhage, lower gastrointestinal hemorrhage, hematuria, bronchopulmonary hemorrhage, epistaxis, esophageal perforation, gastric perforation, duodenal perforation, ileal perforation, small intestinal perforation, colonic perforation, hyperthyroidism, hypothyroidism, nephrotic syndrome, proteinuria, bacteremia, sepsis, pneumonitis, thrombotic thrombocytopenic purpura, hemolytic uremic syndrome, reversible posterior leukoencephalopathy syndrome, pancreatitis, retinal detachment, hair color changes, palmar-plantar erythrodysesthesia syndrome, gastric ulcer, duodenal ulcer, esophagitis, gastritis, nausea, vomiting, diarrhea, and stomach pain. In contrast, the following events were listed in the PAZ package insert but were excluded from evaluation in this study because corresponding CTCAE preferred terms could not be identified: GGT increased, angina pectoris, myocardial ischemia, cerebral hemorrhage, gastrointestinal fistula, and delayed wound healing.
Patients who discontinued hospital visits or transferred to other institutions during the follow-up period were considered censored at the date of last confirmed clinical contact and were included in analysis.
Statistical analysis
Categorical variables were compared using Fisher’s exact test. Continuous variables were analyzed using the Mann–Whitney U test.
PFS was evaluated as the sole survival endpoint. PFS was defined as the time from the initiation of PAZ treatment to either documented disease progression or death from any cause, whichever occurred first.
In addition to the primary comparison between the AS combination group and the non-AS group, a subgroup analysis was also performed to evaluate PFS separately in patients receiving PPIs and those receiving H2RAs. Patients who received both PPIs and H2RAs during the observation period were excluded from the subgroup analysis.
Survival analysis was conducted using the Kaplan–Meier method, and differences in PFS between the AS combination group and the non-AS group were assessed using the log-rank test. A p-value < 0.05 was considered statistically significant.
To adjust for confounding, a Cox proportional hazards model was used, incorporating variables with known relevance to PFS in soft tissue sarcoma—PS, recurrence status, line of therapy, sex, and AS combination. PS, recurrence, and line of therapy were selected based on findings by Nassif et al. [13], while sex was included based on population-based data from Müller et al. suggesting sex-related prognostic heterogeneity [14].
All statistical analyses were performed using EZR version 1.61 [15].



Comments (0)