
Remember me


Based on a report by Yoshiji et al. [13], we categorized the risk levels for each procedure and defined the platelet count required for each level. The degree of bleeding risk was defined based on mild risk, including transcatheter arterial chemoembolization (TACE), endoscopic variceal ligation (EVL), abdominocentesis, balloon-occluded retrograde transvenous obliteration (BRTO), and computed tomography (CT) during arterial portography (CTAP). Moderate risks included radiofrequency ablation (RFA), endoscopic injection sclerotherapy (EIS), endoscopic submucosal dissection (ESD), endoscopic mucosal resection (EMR), liver biopsy (BX), liver tumor biopsy (TmBX), microwave ablation (MWA) and percutaneous ethanol injection therapy (PEIT).
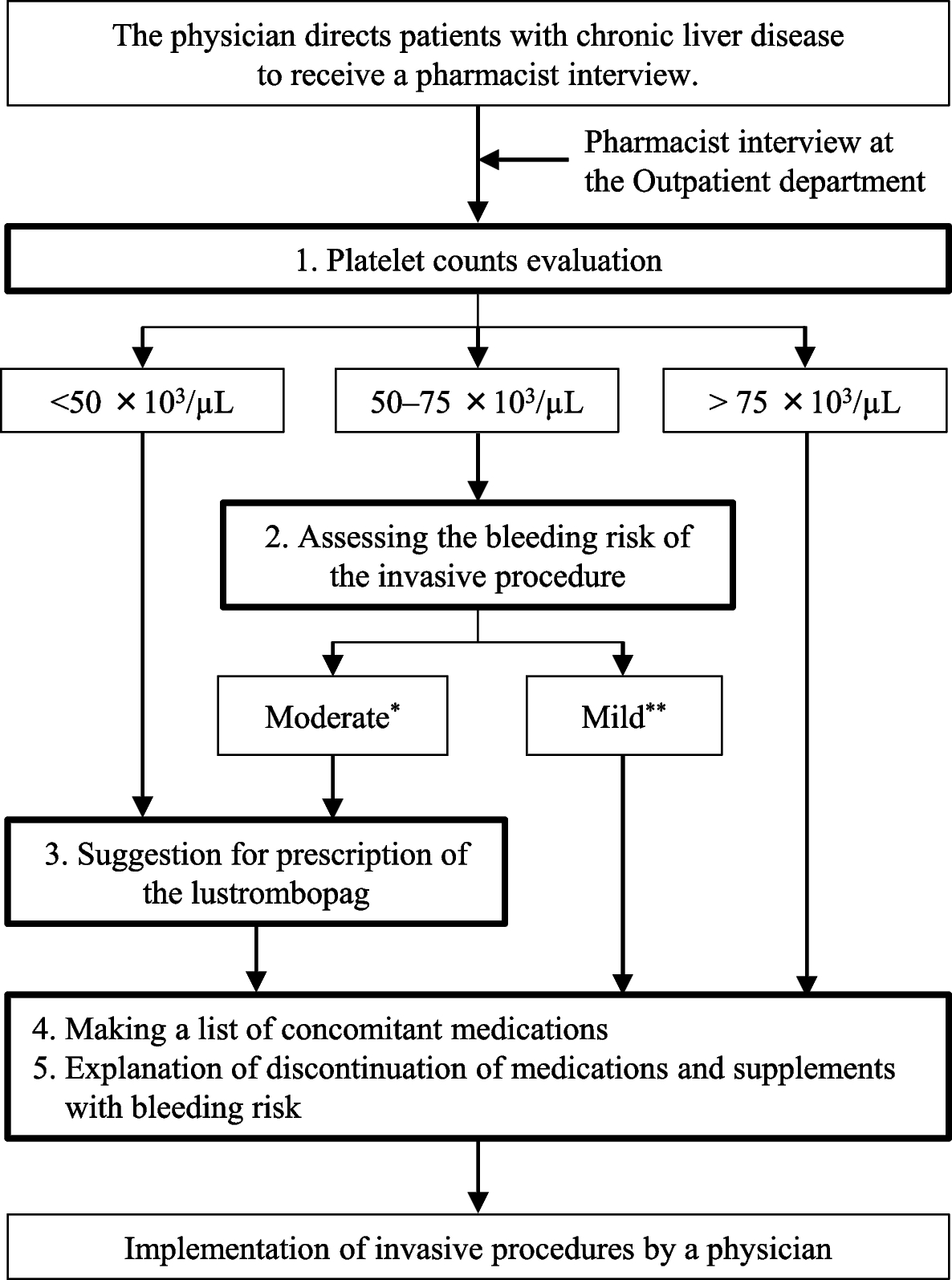
We developed a protocol to determine whether lusutrombopag administration should be recommended (Fig. 1). Briefly, pharmacists classified the patients by the platelet count into three categories: < 50 × 103/µL, 50–75 × 103/µL, and > 75 × 103/µL. Pharmacists suggested prescribing the lusutrombopag for all patients with platelet counts < 50 × 103/µL and for patients with platelet counts of 50–75 × 103/µL undergoing invasive procedures with the moderate bleeding risk as described above. These two suggestions were based on the package insert for lusutrombopag (Mulpleta® Tablets), the former based on clinical trial data, and the latter defined by the statement “This agent should be used when the patient is considered to be at high risk of bleeding based on platelet counts and other laboratory data, clinical symptoms, and the type of invasive procedure performed”. Yoshiji et al. reported that a platelet counts of at least 75 × 103/µL is desirable for patients undergoing moderate-risk procedures [13]. Therefore, we recommended lusutrombopag even if the platelet count was above 50 × 103/µL. This protocol-based pharmacist intervention was performed when the pharmacist interviewed patients with CLD in the outpatient department. The interviews included checking platelet counts, assessing procedural bleeding risk, suggesting the use of lusutrombopag based on the protocol, listing medications prescribed by other hospitals and clinics and supplements and/or over-the-counter medications in use, extracting medications and supplements with bleeding risks, such as antithrombotic agents, and explaining their discontinuation. The medication lists of patients who were not directed to be interviewed by a pharmacist in the outpatient department were prepared by a ward pharmacist through an interview after admission.
Fig. 1
Flowchart of a pharmacist interview to suggest a prescription for a TPO receptor agonist. *The moderate risk includes Radiofrequency ablation (RFA), Esophageal varices sclerotherapy (EIS), Submucosal dissection (ESD), Mucosal resection (EMR), Liver biopsy (BX), Liver tumor biopsy (TmBX), Microwave thermal coagulation (MWA) and Percutaneous ethanol injection therapy (PEIT). **The mild risk includes Chemical embolization of the hepatic artery (TACE), Esophageal vein ligation (EVL), Ascites puncture, Retrograde transverse vein thrombolysis under baroreflex occlusion (BRTO), Computed tomography under portal venography (CTAP)
PatientsPatients with CLD who were scheduled to undergo invasive procedures at the Department of Gastroenterology and Metabolism at Hiroshima University Hospital between August 2022 and February 2023 were enrolled. The exclusion criteria were as follows: patients who had participated in a clinical trial, patients who had undergone or are undergoing a liver transplant, patients with portal vein tumor thrombosis, adult-onset-type citrullinemia, aplastic anemia, myelodysplastic syndrome, myelofibrosis congenital thrombocytopenia, drug-induced thrombocytopenia, immune thrombocytopenia, generalized infection requiring treatment except for viral liver disease, and Child–Pugh class C. The physicians requested an interview with the pharmacist if the patient was taking medications at the time of their examination and the patient has sufficient time for the interview. Patients who were directed to be interviewed by a pharmacist were defined as the pharmacist's intervention (Ph-intervention) group, whereas others were defined as the non-intervention group.
Data collection and analysisThe data used in this study were obtained from clinical records. We extracted data on patient age, sex, type of chronic liver disease, Child–Pugh classification, degree of hepatic encephalopathy and ascites, bilirubin level, albumin level, prothrombin activity level, type of invasive procedure, baseline platelet count, use of medications, use of over-the-counter drugs, use of supplements with bleeding risk, occurrence of thrombosis and bleeding during hospitalization, lusutrombopag prescription, and administration of platelet products. As the primary endpoint in this study, effectiveness was compared between the rate of platelet administration prior to the procedure in the Ph-intervention and non-intervention groups. Safety was evaluated by comparing the numbers of adverse and thrombotic events. In a subgroup analysis, the rate of platelet product administration, platelet counts at the time of the invasive procedure and the incidence of thrombotic events in the patients who were required to receive lusutrombopag were compared between the two groups.
Statistical analysisCharacteristics were compared between the Ph-intervention and non-intervention groups and analyzed using the Mann–Whitney U test for continuous variables and Fisher's exact test for categorical variables. Differences in the rate of platelet product use and the incidence of thrombotic events were compared between the two groups using Fisher's exact test. Univariate logistic regression analysis was used to calculate the odds ratios (ORs) and 95% confidence interval (95% CI) of thrombosis cases in the Ph-intervention and non-intervention groups. Differences were considered statistically significant at P < 0.05. Data analyses were performed using the JMP pro version 17.0.0 (SAS Institute, Cary, NC, USA).
Ethics statementThis study was approved by the Ethics Committee of Hiroshima University (approval No. E2022-0220) in compliance with the Declaration of Helsinki and current legal regulations in Japan. Before collecting the data, we provided the participants with the opportunity to opt out. Information collected from medical records was entered into a case report form and de-identified by an information manager. Therefore, the researchers were unable to identify individuals from the analyzed data.
Comments (0)