
Remember me
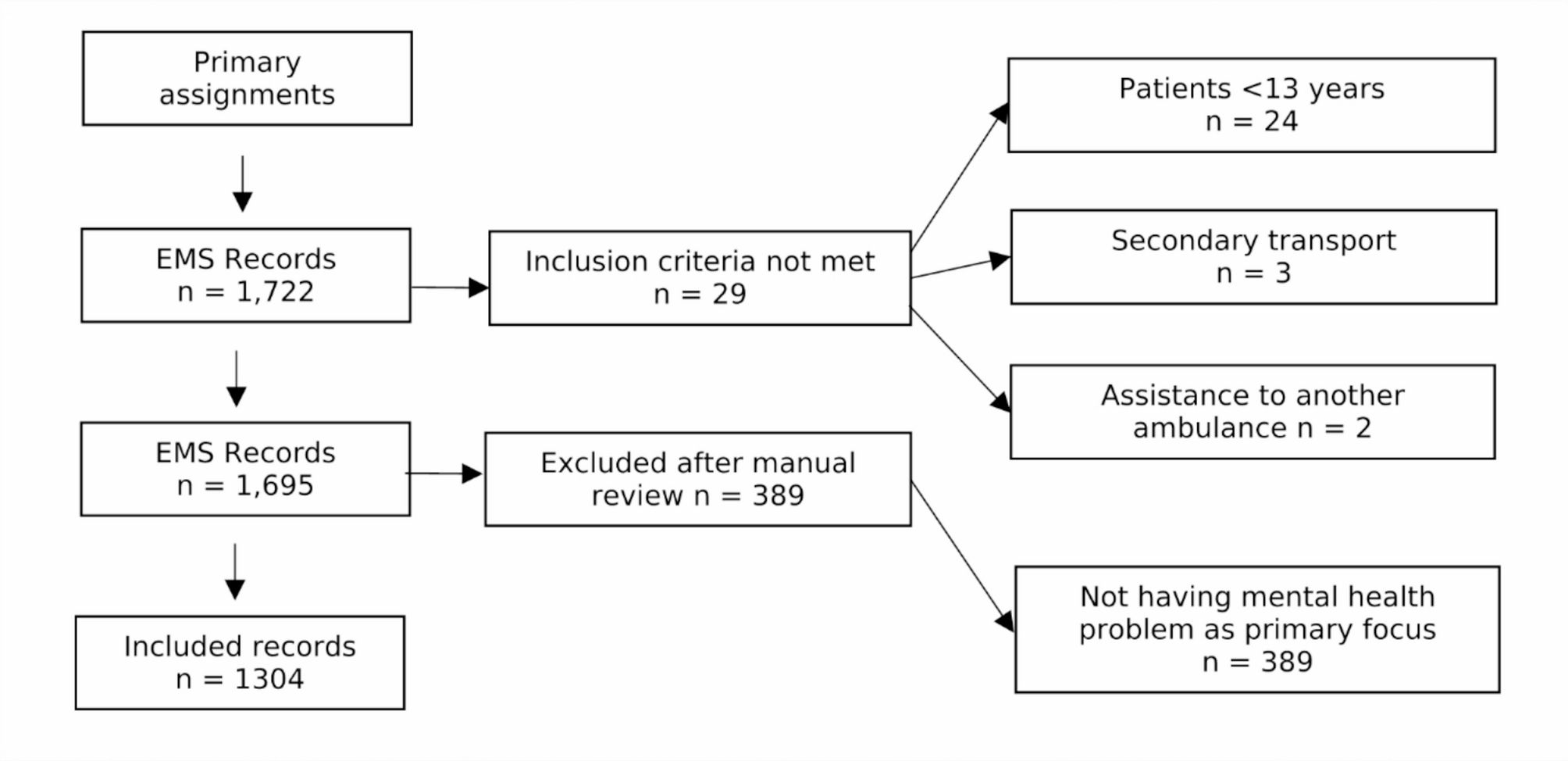






A total of 2110 unique articles were identified through database searches with a further 3 articles from hand searches, and 41 articles from reference list searches. After abstract screening, a total of 81 articles were retrieved for full text review. After application of inclusion and exclusion criteria, a total of 23 articles were included for review and evidence synthesis (Fig. 2). The geographic spread of evidence sources can be seen in Fig. 3.
Fig. 2
Flow diagram demonstrating evidence sources and screening process
Fig. 3
Global heatmap demonstrating geographic spread of included studies
To aid interpretation of these findings, results are presented across three key domains, aligned with our stated research aims. These domains are reflective of the predominant themes within the literature, and explore: the role of bystanders in triage; the accuracy of bystander triage; and the impact of training interventions on bystander triage capability.
Triage and the role of bystandersBystanders already have an established role within the road injury chain of survival, providing first contact with emergency care services thereby activating the emergency response. Here we explore ways to enhance this existing paradigm.
Identification of crash parametersCrash parameters such as seatbelt use, intrusion and deformity of passenger compartments are associated with injury severity and may form part of triage and resource allocation protocols [18, 19]. Despite the potential value of bystander-reported crash parameters, only one study was identified that specifically assessed this capability (Table 1).
Table 1 Triage & the role of bystanders - a summary of study characteristics and key findingsUntrained lay-persons, when asked to identify key crash parameters from traffic accident images, performed as well as health professionals and for many variables approached the accuracy of trained traffic accident researchers. There was a positive training effect across all participant groups. While this involved only 10 lay-participants, it is an interesting proof-of-concept that accurate crash-parameter recognition is possible even amongst untrained lay-bystanders [20].
Video streamingSmartphone ownership continues to grow globally, now accounting for 80% of the 5.8 billion unique mobile subscriptions [21]. The increasing prevalence of smartphones presents an opportunity to enhance current EMS response by using video streaming to provide real-time visual information to EMS dispatchers. There is emerging evidence for use of video streaming for CPR, but there are considerable gaps in the evidence base with regards to its use in other emergencies [22, 23].
Several studies explore the feasibility, effectiveness, and practical challenges of bystander-initiated video streaming in trauma scenarios (Table 1).
Video live streaming appears useful for call-handler assessment of trauma casualties, mechanism of injury and accident scene [24]. One cohort study showed call handler assessment of patient condition changed in around half of cases due to video live streaming and was particularly useful for assessing the unconscious patient [25]. In another study call handlers reported improvements in situational awareness and confidence in decision making [26]. Recognition of immediate first aid requirements by EMS dispatchers also appears to increase with the use of video [27]. Video may also be useful for EMS responders en route to the casualty. Paramedics reported video influenced decision making regarding role and equipment preparedness [28].
Studies demonstrate video streaming is feasible for use with both lay- and professional-bystanders [24], with one small RCT showing 86% of callers were agreeable to using video [26]. Cooperation with bystanders generally appears to be unchallenging, and video streaming is reviewed positively by bystanders [25]. Technical challenges exist such as establishing reliable connections, smartphone availability and language barriers; approximately 10–15% of video attempts appear to fail [25, 26].
Only one study explored psychological harm. No evidence of psychological harm to call handlers from increased exposure to incidents was identified, however due to low survey and interview response rates amongst bystanders, no conclusion regarding harm to bystanders could be made [26].
It should be noted these studies included cases of non-road injury trauma and medical illness. Furthermore all studies were conducted in high-income countries (HICs), and therefore the implications for low and middle income countries (LMICs), where smartphone prevalence is lower is unclear [21].
Accuracy of bystander triageExisting triage toolsMultiple studies sought to evaluate bystander triage accuracy using established triage tools developed for use by EMS in mass-casualty incidents (MCIs) [29,30,31,32,33] (Table 2). Only one study sought to evaluate accuracy of layperson triage and this was also the only study to specifically evaluate triage for road injuries [29]. All other studies evaluated professional bystanders. In all of the studies, participants were provided with written or verbal injury descriptions and physiological parameters; no study asked participants to assess a casualty and derive injury characteristics or vital signs.
Table 2 Accuracy of bystander triage - summary of study characteristics and key findingsCollectively, these studies demonstrate that both lay and professional bystanders are capable of applying simple triage tools with varying degrees of accuracy; there is a general tendency toward over-triage. Training appears to reduce triage errors. All of the assessed triage tools rely on measurable clinical variables such as heart rate or respiratory rate. It is unclear from the available evidence whether bystander-led triage can be consistently accurate enough to be clinically useful, particularly in real-world settings where injury identification and vital sign assessment may be challenging, particularly for lay and non-clinical bystanders.
Lay person triage toolsWe found only one example of a triage tool developed specifically for lay persons - the Keep it Simple and Safe (KISS) tool - which has been designed to use clearly observable signs such as talking, breathing and bleeding for casualty triage [34]. Unfortunately, this tool has yet to be validated.
Training for bystandersThere are numerous studies describing and evaluating trauma training courses for lay-persons [6]; here we have focussed on those which specifically refer to triage in their curricula (Table 3). Given the high incidence of road injury these courses frequently target commercial drivers [3, 4, 35,36,37]. Other target groups include government officials and police officers [4, 35, 38, 39]. All included studies occurred in LMICs where motor vehicle collisions are more common, and EMS remains in its nascent stage [40].
Table 3 Training for bystanders - summary of study characteristics and key findingsThe curricula for these courses appear to be derived from pre-existing trauma guidelines [4, 35], and while these courses are numerous and geographically diverse they frequently appear to be derivatives of each other therefore there is likely significant homogeneity amongst these courses [3, 36, 41]. The included studies do not share their exact curricula nor do they describe precisely how triage is taught, although frequently triage appears to be incorporated within scene management [3, 4, 36, 38, 41].
Two studies involving commercial drivers reported improvements in participant knowledge, including scene management, however this was assessed using only a 15-item questionnaire [3, 36]. A further study also reported a significant increase in triage competence scores, however this study included healthcare professionals as well as lay- and professional-bystanders; scores for individual occupational classes are not reported, and assessment methodology is unclear [35]. Several other studies included triage as a curriculum component, but evaluation was insufficient or not-reported and thus we are unable to evaluate these programmes in relation to triage teaching [4, 5, 37, 39, 42].
Two studies report the use of a Training of Trainers (ToT) approach with increased scene management scores. There were no significant differences in scores obtained between ToT groups suggesting high internal consistency of training. Knowledge regression at 9 months was reported [38, 41].
In interviews, lay responders reported using their triage skills to determine referral decisions based on health centre proximity and injury severity during subsequent casualty encounters [3]. Pre- and post-training surveys also showed increased participant confidence within the triage curriculum domain [43].
While it is evident from these studies that triage is recognised as an essential component of bystander education curricula, it is unclear how triage is being taught. There is some limited evidence to suggest bystanders are able to learn triage skills, and training increases confidence. There is also some evidence to suggest ToT models may be useful for knowledge dissemination to wider populations. Knowledge regression appears to occur, potentially necessitating repeat training. These findings should be interpreted cautiously given the lack of clarity regarding curricula and robustness of assessment methodology.
Comments (0)