This single-center, prospective pilot trial was approved by the Ethics Committee of Heidelberg University (S-004/2023) and registered prior to trial enrollment in the German Clinical Trials Registry (DRKS00031867, Registration Date 22.05.2023). The reporting of this trial follows the Strengthening the Reporting of Observational Studies in Epidemiology statement (Supplement STROBE Checklist) [12]. Due to the exploratory character, no formal sample size calculation was performed. We planned to enroll patients over one year.
Setting
The emergency medical services (EMS) in the Rhine-Neckar region have a two-tier system, with ambulances staffed by one paramedic and one emergency medical technician, and physician response cars staffed by one emergency medicine physician and one paramedic. The rescue control center is responsible for registering every medical emergency call within the region and deciding whether an ambulance is sufficient for the emergency or if a physician response car is required immediately. Moreover, the paramedics can determine whether an emergency physician is needed. To every suspected OHCA or unconscious patient, severe trauma, suspected myocardial infarction, or acute dyspnea, both ambulance and physician response cars are dispatched. Therefore, it captures the subset of patients with circulatory impairment.
Both units have the Corpuls C3 or Corpuls C3T (GS Elektromedizinische Geräte G. Stemple GmbH, Kaufering, Germany) as monitors and defibrillation systems. Some physician response cars have the possibility for IABP monitoring. Standard care involved iNIBP measurements (using the Corpuls device) at intervals determined by the treating team or as clinically needed.
Enrollment
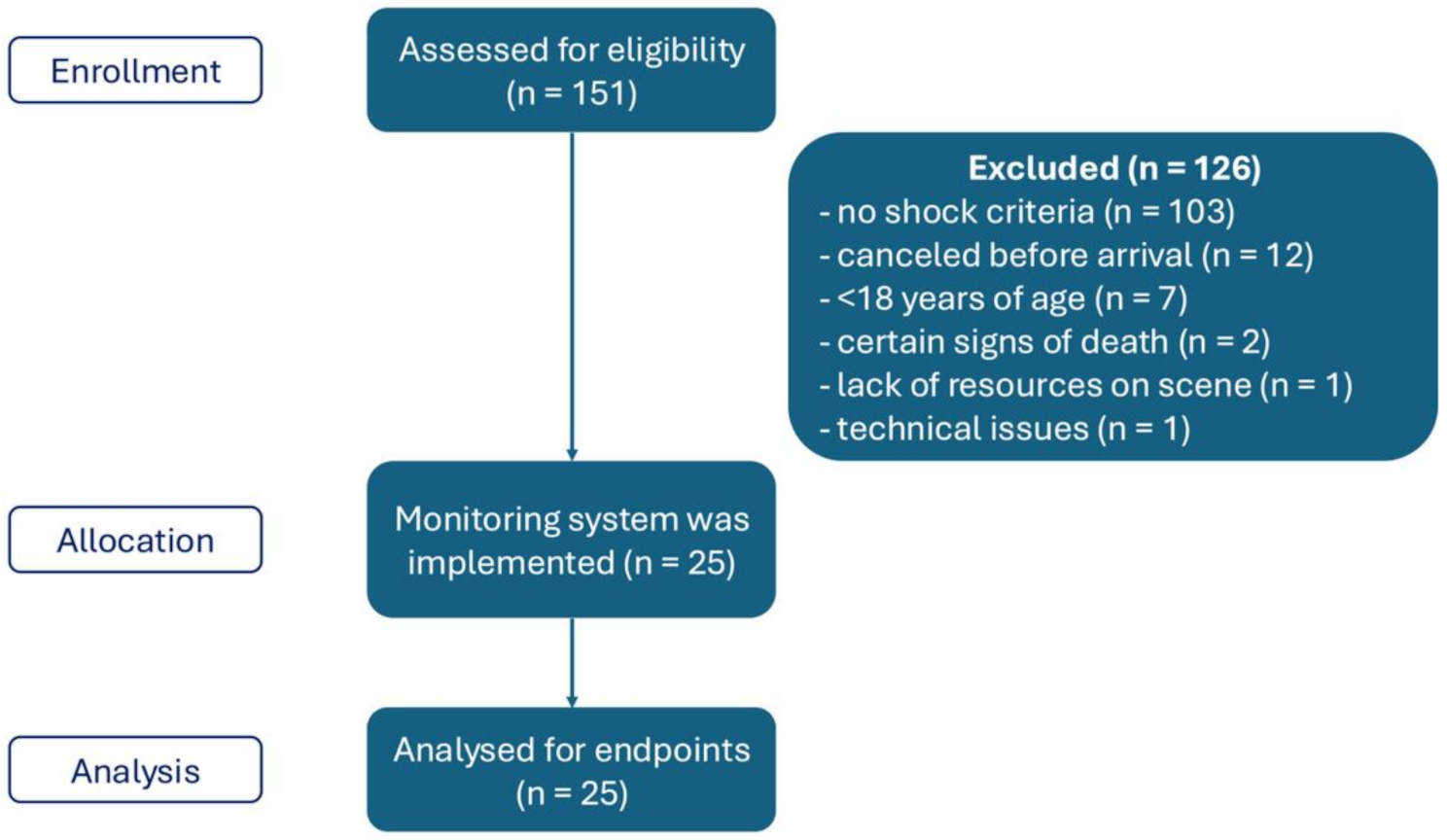
A study team member randomly accompanied different physician response cars in the Rhine-Neckar EMS system. At the time of data acquisition, the study team member was a medical student and paramedic. Patients over 18 years with shock were eligible for enrollment. Shock could be due to suspected acute coronary syndrome (ACS), trauma, undifferentiated shock, or OHCA. Patients were included if they met the inclusion criteria, and no exclusion criteria were applicable (Table 1).
For the definition of “undifferentiated shock” on the scene, the capillary refill time on the patient’s palm had to be over two seconds or the shock index > 1. “Undifferentiated” referred to shock of any other cause except acute myocardial infarction or trauma.
A suspected ACS was determined by an indicative clinical presentation of patients, with or without specific electrocardiogram findings.
Patients with OHCA were enrolled during ongoing cardiac arrest or return of spontaneous circulation (ROSC), depending on the arrival of the physician response car. After ROSC, measurements were performed until the patient arrived at the hospital.
This patient population was chosen because it reflects the most common and clinically relevant prehospital scenarios associated with hemodynamic instability and the risk of hypotension.
A physician not involved in the study had to determine if the patient’s condition was potentially life-threatening. After positive screening, patients were enrolled without explicit consent under an initial emergency exemption. All patients or their legal representatives were visited or contacted by phone by a study physician after hospital admission to obtain informed consent.
Table 1 Inclusion and exclusion criteriaStudy interventions
During the study period, an additional Edwards HemoSphere monitoring system was carried, equipped with the ClearSight module for cNIBP and ForeSight for StO2 measurement via near-infrared spectroscopy (NIRS). If the patient met the inclusion criteria, the study personnel applied the HemoSphere system while the EMS crew established standard monitoring. The ForeSight StO2 sensor was placed on the contralateral forearm to the iNIBP cuff. The treating EMS teams were not blinded to the study interventions. The treating teams were allowed to use the cNIBP and StO2 values for clinical decision making at their own discretion. After the mission, all monitoring data were extracted.
A detailed description of the HemoSphere system is presented in the supplements (Supplement Text 1, Supplement Figs. 1 and 2).
Endpoints, data synthesis, and statistical analysis
The primary endpoint was to assess agreement between paired cNIBP and iNIBP measurements. Secondary endpoints included the relationship between StO2 and cNIBP and iNIBP measurements. Further, we evaluated the duration of unrecognized hypotension phases. A hypotensive phase was defined as a MAP of 60 mmHg or lower.
Descriptive statistics were performed for continuous parameters using mean and standard deviation (SD) or median and interquartile range (IQR). For categorical parameters, counts and percentages were used.
Continuous parameters were assessed for homogeneity and analyzed using a paired Student’s t-test with a 95% confidence interval (CI) and Pearson correlation with a predefined interpretation (Supplement Table 1) [13]. Agreement between cNIBP and iNIBP measurements was assessed using Bland-Altman analysis [14]. For each parameter, the bias (mean difference) and the 95% limits of agreement (LoA) were calculated. In addition, 95% confidence intervals were computed for the bias and the LoA to quantify the precision of the estimates [15, 16]. Results were visualized as Bland-Altman plots indicating the bias and LoA. Analyses were performed using only complete measurement pairs.
Differences in StO2 between the MAP groups of < 60 mmHg and ≥ 60 mmHg were compared using analysis of variance (ANOVA). A two-sided significance level was defined at p < 0.05. Only cases with a complete dataset were included. For all analyses, the latest version of SPSS was used.







Comments (0)