This Delphi consensus study identified and categorised time-sensitive injuries and interventions relevant to the care of patients physically trapped following motor vehicle collisions. Through iterative survey rounds and a final consensus meeting, SMEs reached agreement on key principles guiding injury classification and intervention. Notably, there was strong agreement that certain clinical interventions—including administration of analgesia, tranexamic acid (TXA), and protection from environmental stressors—are essential and should be considered routine. These interventions were seen as both feasible and ethically necessary to be delivered as early as possible following road injury; including by trained non-clinical personnel such as police or fire and rescue services.
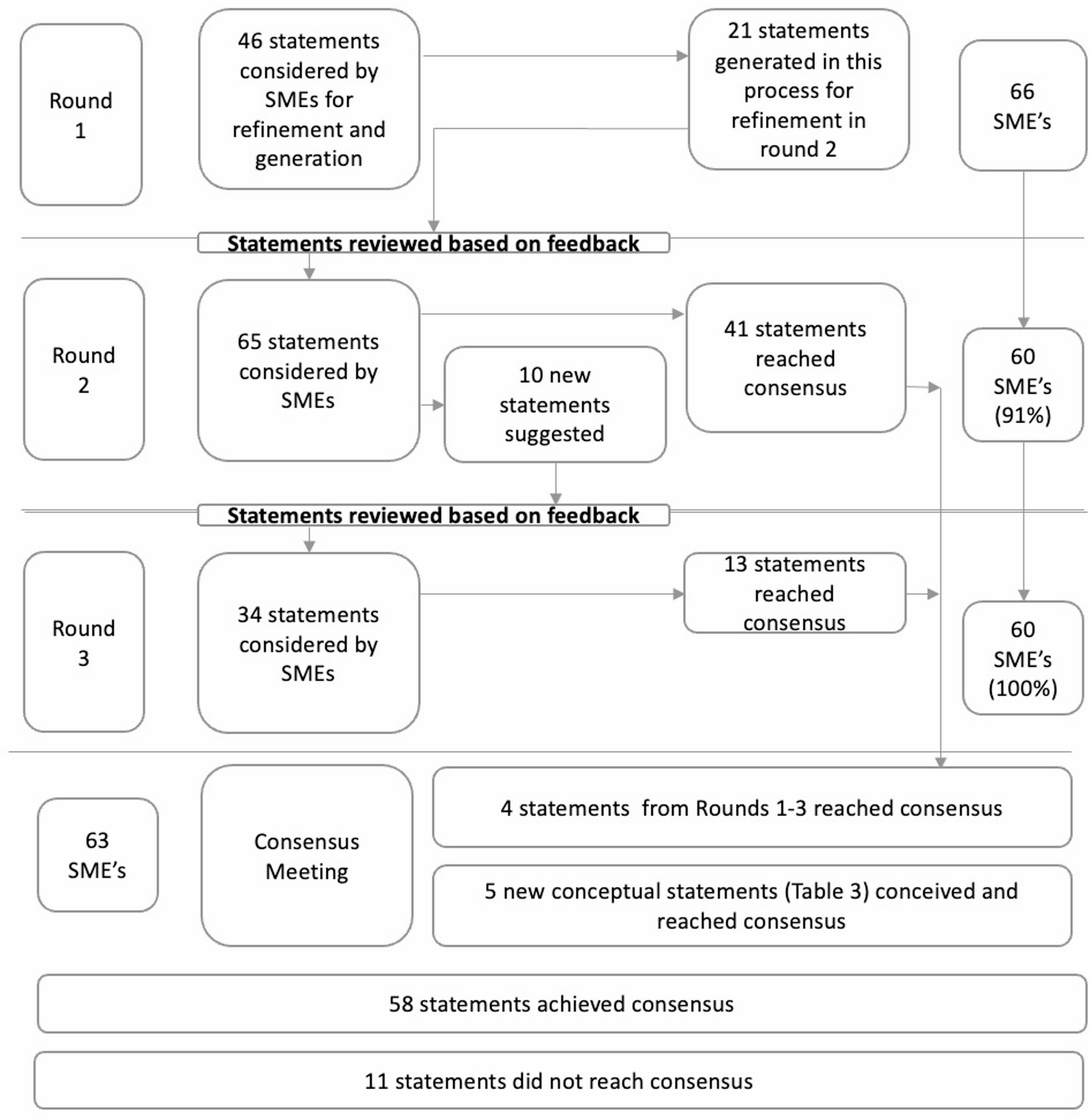
The study used a rigorous Delphi methodology, including diverse SME’s across emergency medicine, pre-hospital care, fire and rescue services, and paramedicine. Anonymised feedback, iterative voting, and a facilitated consensus meeting provides a robust framework to generate and refine statements, and to support convergence towards agreement.
However, there are limitations; some stakeholder groups were underrepresented, particularly patients and public contributors, who may have provided important insights into acceptability, ethics, and risk tolerance. Additionally, while Delphi processes are well-suited for complex or poorly evidenced topics, they are inherently consensus-driven and may fail to resolve deeply held differences in perspective or practice [10]. Furthermore, consensus meetings may be more likely to attract individuals who are already supportive of change, potentially skewing the discussion towards more progressive or interventionist positions and limiting the diversity of viewpoints. Several statements did not reach consensus, reflecting ongoing uncertainty or variability in operational capacity and governance frameworks. For categorising statements, definitions such as ‘respiratory failure’ or ‘physiological deterioration’ are not strictly defined and may be open to subjective interpretation leading to a lack of reproducibility.
The defining of “time critical” or “time dependent” interventions based on a specific diagnosis of injury (e.g. tension pneumothorax) may be overly complicated. Accurate clinical assessment to allow the diagnosis of specific injuries is known to be challenging in rescue environments, especially where there is limited access to the patient’s anatomy, safety considerations, and distractions including noise from cutting equipment. Clinical examination performed by experienced prehospital providers only has a moderate ability to correctly identify injuries, and responders without extensive medical training or exposure to trauma patients are even less likely to accurately diagnose these conditions [12,13,14]. This reinforces the need for pragmatic approaches to decision-making and the development of simple, recognisable heuristics and associated interventions —such as decreased level of consciousness or inability to speak in full sentences —to help identify patients in need of urgent care.
There is a growing body of literature recognising the challenges of delivering early, equitable care to trapped patients. Research demonstrates that women are significantly less likely to receive tranexamic acid treatment across all injury severity levels and baseline bleeding risk categories, despite equivalent clinical benefit, highlighting systemic inequities in trauma care delivery [15]. Similarly, sex-disaggregated analysis reveals that female patients are more frequently trapped than males (15.8% vs. 9.4%) and sustain different injury patterns, yet receive less aggressive treatment approaches [16]. These studies collectively demonstrate that current trauma care systems fail to deliver equitable treatment to all patient groups, particularly highlighting disparities affecting women and older patients. This study adds to existing literature by providing a structured, multi-agency view of which interventions should be prioritised and who might be empowered to deliver them, directly addressing the care delivery inequities identified in previous research. Interventions classified as routine included airway manoeuvres and basic adjuncts, oxygen administration, control of haemorrhage, analgesia and TXA. The prioritisation of analgesia and TXA aligns with previous research demonstrating their mortality benefit across patient populations, and importantly, our consensus supports making these interventions available regardless of provider background [17]. This finding underscores a collective willingness to re-evaluate traditional role boundaries and expand treatment access—a critical step toward addressing the systemic inequities documented in trapped patient care. The consensus approach of empowering non-clinical responders to deliver time-critical interventions, offers a potential solution to the access disparities that disproportionately affect vulnerable patient populations identified in the literature.
This study provides foundational consensus on priorities for early intervention during entrapment, offering guiding principles on which future clinical frameworks and operational guidance may be built. These principles can support the development of standard operating procedures, inform multi-agency training, and guide future policy. Most significantly, the findings provide a cross-disciplinary mandate to explore the safe extension of specific clinical responsibilities—such as delivery of analgesia or TXA—to appropriately trained non-clinical personnel, under suitable governance.
There are clear implications for the design of future trauma systems. Interventions should not be limited by provider role or professional boundary, but by the feasibility, safety, and impact of delivery in the pre-hospital phase. This supports the development of interoperable trauma care models that empower all responders to contribute to early stabilisation and symptom relief. Importantly, this study also suggests that principles developed for physically trapped patients should be extended to all seriously injured road users, given the similarity in their clinical needs and the urgency of care.
To realise the translational potential of these findings, targeted dissemination across all involved sectors is essential. The involvement of multiple agencies—each with distinct training structures, regulatory frameworks, and operational mandates—requires tailored approaches to education, guideline development, and policy translation. These findings will support the creation of role-specific guidance and underpin updates to joint operational procedures. Additionally, plain-language materials are needed to ensure accessibility for non-clinical responders, including fire and rescue personnel, who may assume new responsibilities as a result of this work.
Several questions remain. First, there is a need for better data linking specific injury patterns to outcomes in trapped patients, to refine our understanding of which conditions are genuinely time-critical and what impact early intervention may have. Second, although this study identified priority interventions, it remains unclear how best to train, equip, fund and govern non-clinical personnel to deliver them safely and consistently. Legislative frameworks—such as the Human Medicines Regulations (UK)—would need to be reconsidered. The potential role of novel technologies, app-based resources, and Artificial Intelligence (AI) should also be explored to support the delivery of these treatments and new models of care.
Finally, further research is required to validate simple heuristics or triage tools that can be reliably used by both clinicians and non-clinicians to identify critical injuries and associated interventions in the context of entrapment. These should be evaluated not only for accuracy but also for usability in high-stress, resource-constrained environments. This will be essential to underpin future decision support tools, frameworks, and training programmes aimed at improving outcomes for entrapped and seriously injured road users alike.







Comments (0)