
Remember me








Of 477 newly diagnosed patients with GBM treated at Tokyo Women’s Medical University between 2006 and 2021, 416 patients who received the Stupp regimen and had sufficient follow-up data were included in this analysis. After excluding 41 biopsy cases, 375 patients who underwent maximal resection remained for evaluation.
The study comprised 164 patients in the AFTV group and 211 in the non-AFTV group. The median age was significantly lower in the AFTV group (51.2 ± 14.4 years) than in the non-AFTV group (56.1 ± 15.1 years; p < 0.01). Although the AFTV group had a significantly lower median age, the therapeutic effects of AFTV therapy in elderly patients were analyzed as part of our study design to assess its efficacy across different age groups and account for potential age-related biases. No statistically significant differences were observed between the two groups in terms of sex ratio, Karnofsky Performance Status (KPS), laterality, or tumor location. The baseline characteristics of the patients are summarized in Table 1.
Table 1 Baseline characteristics of the study populationOverall efficacy of AFTV therapyComparison between the AFTV (n = 164) and non-AFTV (n = 211) groups demonstrated significantly prolonged PFS and OS in the AFTV group. The median PFS was 14.0 months in the AFTV group versus 8.7 months in the non-AFTV group (p = 0.03; Fig. 1a). Similarly, the median OS was 32.0 months in the AFTV group compared with 21.9 months in the non-AFTV group, demonstrating a statistically significant improvement (p < 0.01; Fig. 1a). These results suggest the potential of AFTV therapy to improve the prognosis of patients with GBM.
Fig. 1
Kaplan–Meier survival curves illustrating the efficacy of AFTV therapy across various subgroups. a All Patients with GBM: AFTV therapy significantly improved survival outcomes compared to the non-AFTV group. The median progression-free survival (PFS) was 14.0 months in the AFTV group and 8.7 months in the non-AFTV group (p = 0.03). The median overall survival (OS) was 32.0 months in the AFTV group and 21.9 months in the non-AFTV group (p = 0.002). b Elderly GBM Cases: Among patients aged 65 years or older, AFTV therapy significantly extended survival. The median PFS was 14.2 months in the AFTV group and 8.1 months in the non-AFTV group (p = 0.02), while the median OS was 27.3 months in the AFTV group and 17.0 months in the non-AFTV group (p = 0.005). c Early Recurrent Cases: In cases of recurrence within six months of initial treatment, AFTV therapy led to significantly prolonged survival. The median OS was 15.1 months in the AFTV group and 9.5 months in the non-AFTV group (p = 0.001)
Illustrative case 1A 62-year-old woman presented with progressive aphasia and right hemiparesis. MRI revealed multiple contrast-enhancing lesions in the left frontal and parietal lobes. The patient underwent tumor removal and photodynamic therapy (PDT) to achieve gross total resection (GTR) of the enhancing lesions. Postoperatively, AFTV therapy was administered. Despite moderate aphasia and mild hemiparesis, the patient has maintained a Karnofsky Performance Status (KPS) of 60 and has remained recurrence-free for 9 years postoperatively. This case highlights the potential of AFTV therapy in achieving exceptional long-term disease control (Fig. 2).
Fig. 2
Illustrative Case 1, a 62-year-old female with glioblastoma (GBM) who achieved long-term disease control with AFTV therapy. Preoperative MRI revealed multiple contrast-enhancing lesions in the left frontal and parietal lobes. The patient underwent gross total resection (GTR) combined with photodynamic therapy (PDT), followed by AFTV therapy. Postoperative MRI confirmed successful lesion removal, and at nine years post-surgery, no recurrence has been observed. Despite moderate aphasia and mild hemiparesis, the patient continues to maintain disease control, highlighting the potential of AFTV therapy in achieving durable remission
Efficacy of AFTV in older patientsWe evaluated the efficacy of AFTV therapy in 113 older patients (aged ≥ 65 years), including 29 in the AFTV group and 82 in the non-AFTV group. The median PFS was 14.2 months in the AFTV group compared with 8.1 months in the non-AFTV group (p = 0.02; Fig. 1b). Similarly, the median OS was 27.3 months in the AFTV group compared with 17.0 months in the non-AFTV group, demonstrating a statistically significant improvement (p < 0.01; Fig. 1b). These results demonstrated that AFTV therapy is a viable treatment option for older patients with GBM, who typically have poor prognoses.
Efficacy of AFTV in early recurrence casesAmong 114 early recurrence cases (defined as recurrence within 6 months of initial treatment), 32 patients were in the AFTV group and 82 were in the non-AFTV group. The median OS was 15.1 months in the AFTV group compared with 9.5 months in the non-AFTV group (p < 0.01; Fig. 1c). These findings indicated that AFTV remains effective even in cases of aggressive disease progression.
Illustrative case 2A 59-year-old woman presented with right hemianopia; MRI revealed a contrast-enhancing lesion in the left occipital lobe. Following gross total resection at another institution, the patient was referred to our hospital, where radiotherapy, chemotherapy, and AFTV therapy were initiated. Six months after treatment, recurrence was observed along the resection cavity wall. The patient underwent a second tumor resection with PDT, and pathological analysis confirmed recurrent GBM. Six months later, a second recurrence occurred, and another resection was performed. Pathological examination of the specimen revealed predominantly necrotic tissue with minimal tumor cells. The patient has remained recurrence-free for seven years, achieving a total survival of eight years from initial surgery, with a maintained KPS of 80. This case suggested a potentially delayed efficacy of AFTV therapy, even in cases of early recurrence (Fig. 3).
Fig. 3
Illustrative Case 2, a 59-year-old female with early recurrent glioblastoma (GBM) who achieved long-term survival. Preoperative MRI revealed a contrast-enhancing lesion in the left occipital lobe. After gross total resection, she received radiotherapy, chemotherapy, and AFTV therapy. Tumor recurrence occurred twice within six months of the previous surgery, requiring two additional resections with photodynamic therapy (PDT). The final pathology showed predominantly necrotic tissue with minimal tumor cells. The patient has remained recurrence-free for seven years following the third surgery, achieving a total survival of eight years with a Karnofsky Performance Status (KPS) of 80. This case suggests a potential delayed effect of AFTV therapy, even in early recurrent GBM
Association between molecular pathological factors and AFTV therapyIDH mutation and AFTV efficacyWe evaluated the association between IDH status and AFTV efficacy in 115 patients, consisting of 22 patients with IDH-mutant and 93 with wild-type IDH tumors. Among the 22 patients with IDH-mutant tumors (14 in the AFTV group and 8 in the non-AFTV group), we did not detect any significant differences in PFS (p = 0.8) or OS (p = 0.3) between the groups. These findings suggested that AFTV therapy has limited efficacy in altering the outcomes of IDH-mutant GBM, which is associated with a favorable prognosis (Fig. 4a).
Fig. 4
Kaplan–Meier survival curves illustrating the association between molecular pathological markers and AFTV therapy. a IDH-mutant GBM cases: No significant differences in progression-free survival (PFS, p = 0.8) or overall survival (OS, p = 0.3) were observed between the AFTV and non-AFTV groups, suggesting limited efficacy of AFTV therapy in IDH-mutant GBM. b IDH wild-type GBM cases: AFTV therapy significantly improved survival outcomes. The median PFS was 16.2 months in the AFTV group versus 6.3 months in the non-AFTV group (p = 0.003), and the median OS was 34.2 months versus 22.9 months, respectively (p = 0.002). c p53 expression in IDH wild-type GBM: Patients with p53-negative tumors showed significantly longer OS compared with those with p53-positive tumors (35.3 vs 24.8 months, p = 0.03). PFS also tended to be longer in the p53-negative group (17.2 vs 11.6 months, p = 0.07). d PD-L1 expression and survival outcomes: AFTV therapy was more effective in PD-L1-negative cases, with a median PFS of 19.1 months versus 9.8 months in PD-L1-positive cases (p = 0.04), and a median OS of 36.1 months versus 28.3 months, respectively (p = 0.03). e Combined p53 and PD-L1 status in IDH wild-type GBM: Patients with tumors negative for both p53 and PD-L1 (double-negative) had the most favorable prognosis, while those with tumors positive for both markers (double-positive) had the poorest. Median PFS was 20.9 months in the double-negative group versus 9.8 months in the double-positive group (p = 0.04), and median OS was 35.3 months versus 24.5 months, respectively (p = 0.03). A log-rank test for overall comparison among the four subgroups revealed a borderline difference in PFS (p = 0.06) and a similar trend in OS (p = 0.1)
Among the 93 patients with wild-type IDH (44 in the AFTV group and 49 in the non-AFTV group), we identified significant improvements in the survival outcomes of those treated with AFTV. The median PFS was 16.2 months in the AFTV group, which was substantially longer than the 6.3 months observed in the non-AFTV group (p < 0.01). Similarly, the median OS was 34.2 months in the AFTV group compared with 22.9 months in the non-AFTV group, showing a statistically significant improvement (p < 0.01; Fig. 4b). These findings indicated the efficacy of AFTV therapy in improving the survival outcomes of patients with wild-type IDH GBM.
Association between p53 expression and AFTV therapy in wild-type IDH GBMWe evaluated the prognostic effect of p53 expression on AFTV therapy efficacy in 91 patients with wild-type IDH GBM, including 59 in the AFTV group and 32 in the non-AFTV group. In the p53-negative subgroup, patients exhibited longer PFS and OS compared to those in the p53-positive subgroup. The median PFS was 17.2 months in the p53-negative subgroup and 11.6 months in the p53-positive subgroup (p = 0.07). The median OS was 35.3 months in the p53-negative subgroup and 24.8 months in the p53-positive subgroup, showing a statistically significant improvement (p = 0.03) (Fig. 4c).
PD-L1 expression and AFTV efficacyWe conducted PD-L1 expression analysis in 97 patients, 63 of whom were classified as PD-L1-negative, whereas 34 were classified as PD-L1-positive.
In PD-L1-negative patients, the median PFS was 19.1 months, which was significantly longer than the 9.8 months observed in PD-L1-positive patients (p = 0.04). Similarly, the median OS was 36.1 months in PD-L1-negative patients compared with 28.3 months in PD-L1-positive patients, demonstrating a statistically significant difference (p = 0.03). These findings suggested the enhanced efficacy of AFTV therapy in patients with PD-L1-negative disease. Nonetheless, even in PD-L1-positive patients, AFTV therapy contributed to improved prognosis compared with that in untreated patients, albeit with reduced efficacy, suggesting that PD-L1 status may influence the therapeutic response to AFTV.
Combined p53 and PD-L1 status and AFTV efficacyWe further classified 78 patients with wild-type IDH GBM who had complete p53 and PD-L1 expression data into four subgroups based on their p53 and PD-L1 immunostaining status: p53 + /PD-L1 + , p53 + /PD-L1 − , p53 − /PD-L1 + , and p53 − /PD-L1 − . A log-rank test for overall comparison among the four groups revealed a borderline difference in PFS (p = 0.06) and a similar trend in OS (p = 0.1) (Fig. 4e). Notably, direct comparison of the p53 − /PD-L1 − subgroup, which showed the most favorable outcome, and the p53 + /PD-L1 + subgroup, which showed the poorest, demonstrated significant differences in survival. The median PFS was 20.9 months in the p53 − /PD-L1 − subgroup and 9.8 months in the p53 + /PD-L1 + subgroup (p = 0.04). The median OS was 35.3 months in the p53 − /PD-L1 − subgroup and 24.5 months in the p53 + /PD-L1 + subgroup (p = 0.03), suggesting that the absence of both p53 overexpression and PD-L1 expression is associated with improved therapeutic response to AFTV.
Evaluation of the immune microenvironmentWe also evaluated the immune microenvironment in both PD-L1-positive (n = 34) and PD-L1-negative (n = 63) groups. We found that CD3-positive T-cells and CD8-positive cytotoxic T-cells infiltrated the peritumoral area in both groups. CD4-positive helper T-cells were scarce, with 22.7% (5/22) of patients in the PD-L1-positive group and 5.4% (2/37) in the PD-L1-negative group (p = 0.09). CD8-positive cytotoxic T-cell infiltration was comparable between the groups and was observed in 95.5% (21/22) of PD-L1-positive and 94.6% (35/37) of PD-L1-negative (p = 1.00) patients. Macrophage infiltration (CD68-positive) was confirmed in all cases regardless of PD-L1 expression.
The distribution of immune cells in PD-L1-positive tumors showed a trend toward increased CD4-positive cells but did not differ significantly from that in PD-L1-negative tumors. Figure 5 shows representative immunohistochemical staining patterns of PD-L1-positive tumors.
Fig. 5
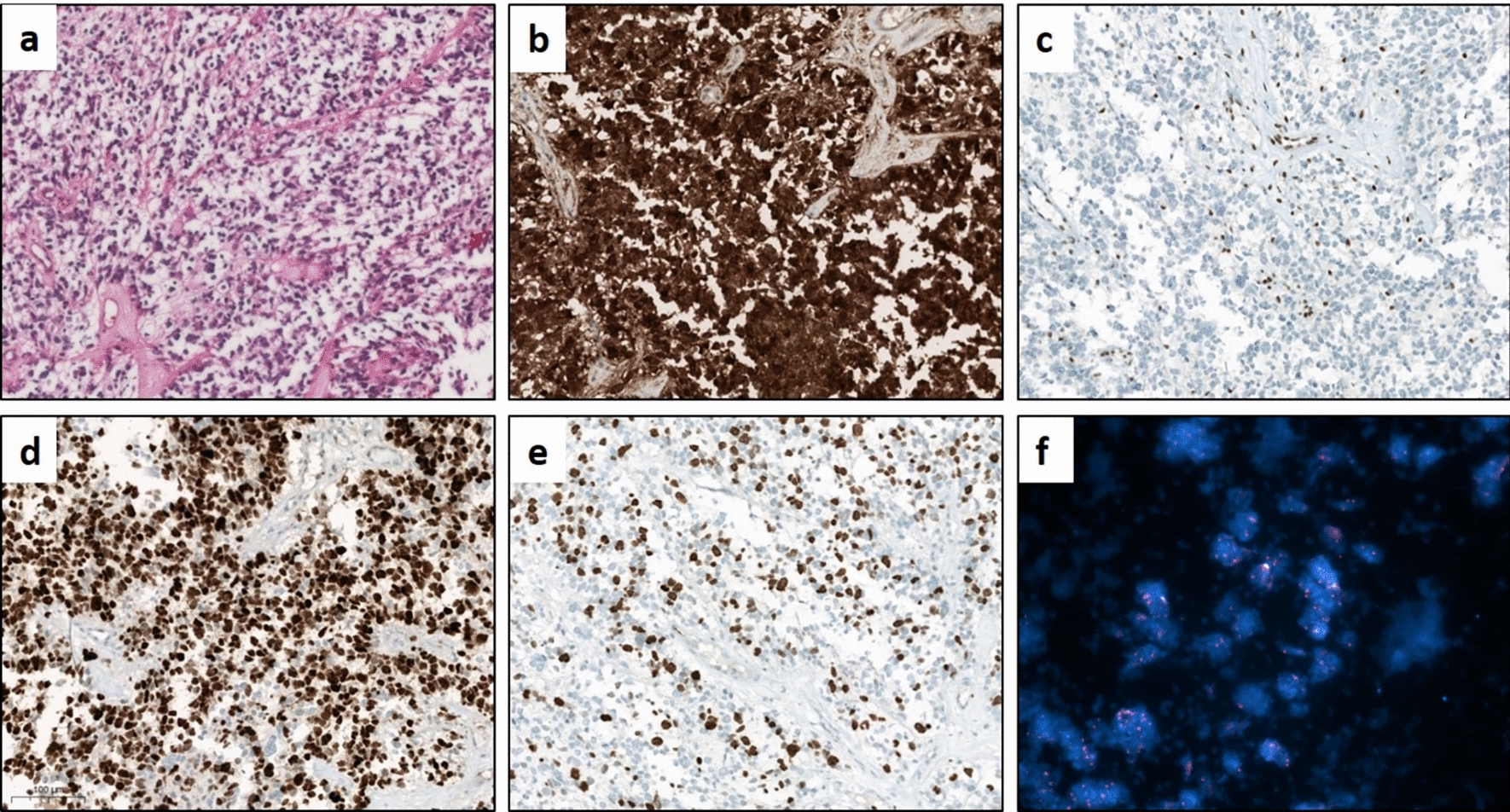
Representative immunohistochemical staining patterns in a PD-L1-positive glioblastoma case. a Hematoxylin and eosin (H&E) staining showing characteristic glioblastoma histopathology. b PD-L1 immunohistochemistry demonstrating strong membranous positivity. c CD68 immunostaining confirming macrophage infiltration. d CD3 immunostaining indicating T-cell infiltration. e CD4 immunostaining showing a lack of helper T-cell activity. f CD8 immunostaining demonstrating cytotoxic T-cell infiltration in the peritumoral area. CD3-positive and CD8-positive T cells were present, while CD4-positive helper T cells were rarely observed. A similar distribution of immune cells was noted in PD-L1-negative cases
Comments (0)