
Remember me


The trauma bay is often the first point of contact for a trauma patient entering a hospital system. During a trauma activation a multidisciplinary team of emergency medicine and trauma physicians as well as nursing staff receive handoff from pre-hospital personnel all the while rapidly, and systematically evaluating and stabilizing the patient at hand, Fig. 1. The role of the resuscitation leader has many colloquial terms including trauma “captain” and trauma “team leader.” Having a designated trauma leader is an important strategy for synchronizing the team, and maintaining communication and processes [1]. This complex, high-stakes environment requires organization and standardization on multiple levels. Ford et al.’s 2016 review of the literature noted that strong leadership improves processes of care in trauma resuscitation including speed and completion of the initial evaluation [2].
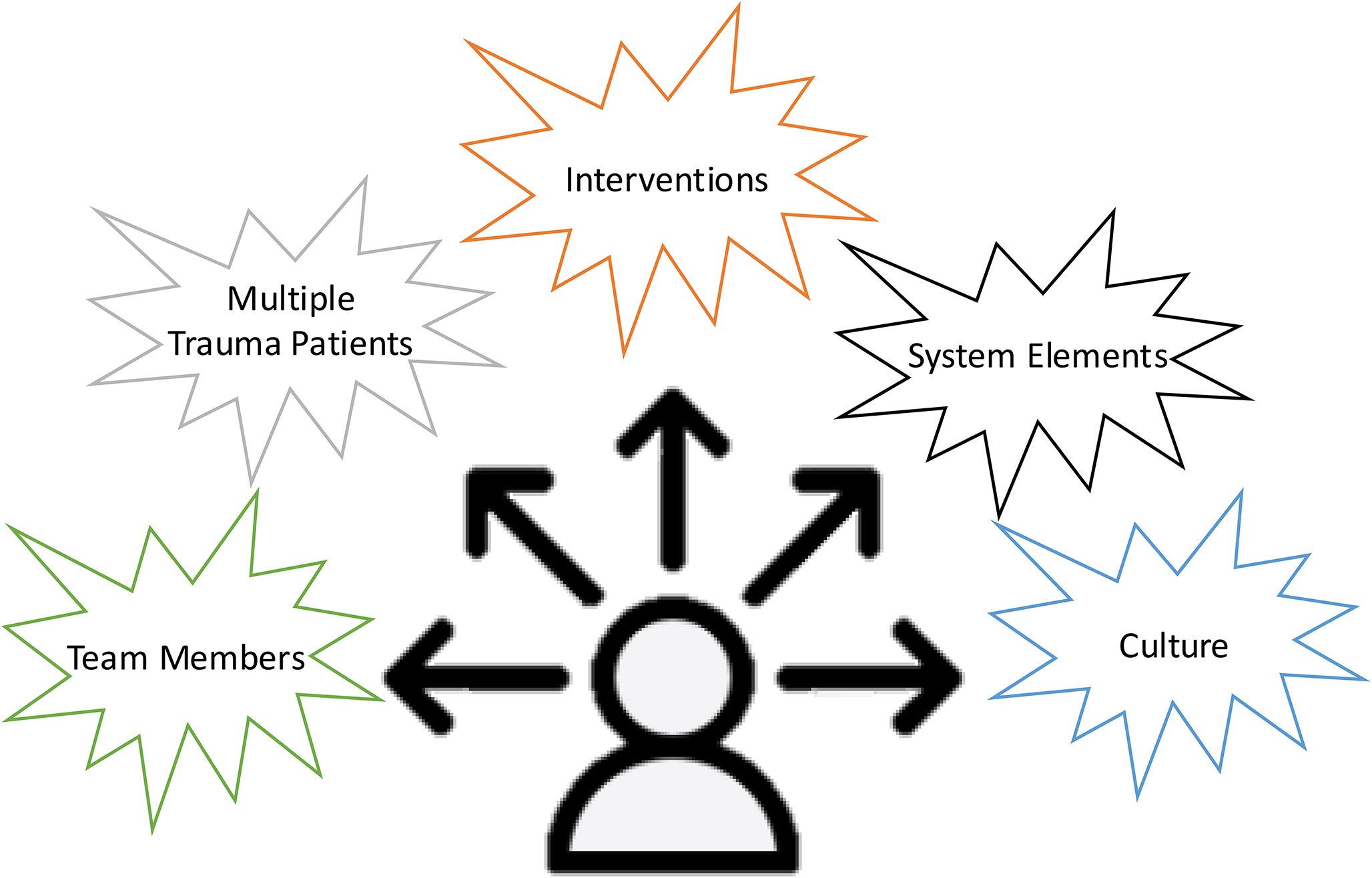
Fig. 1
Multiple competing factors a trauma team leader must coordinate and organize to progress their patients’ care
Leadership training is increasingly being incorporated into trauma courses and simulation-based training [1]. The American College of Surgeons (ACS) Committee on Trauma developed the Advanced Trauma Life Support (ATLS) program to provide a safe and reliable method for immediate management of injured patients [3]. In ATLS, leadership is noted as a crucial skill for coordinating the trauma team. Leadership is a multi-faceted, nontechnical skill that includes several competencies: effective communication, efficiency, decision-making, and resource management skills [3]. The ability to lead for some is a natural trait, but ultimately these skills can be learned and refined.
The current manuscript seeks to summarize the importance of leadership in the trauma bay and more specifically aims to evaluate: leadership styles, leadership assessment tools, professionalism, the concepts of command and control and systems-based practice, and leadership education. This work includes relevant literature as well as a summary of the authors’ experiences.
Leadership StylesLeadership in healthcare comes in many forms. The optimal style of leadership used is influenced by team make-up and experience, and a patient’s clinical status. A few overarching leadership styles seen in the trauma bay include transactional, transformational, and passive leadership.
Transactional leadership is based on exchanges between the leader and team members in which team members are rewarded for meeting specific performance criteria. The use of closed-loop communication is a prime example, which will be discussed in more detail in the systems-based practice section. The trauma team leader assesses the trauma patient’s clinical status upon arrival and provides clear instruction for various tasks to be completed throughout the resuscitation. The team members are not necessarily expected to think innovatively [2]. Ford et al.’s review describes this form of leadership as directive [2]. Directive leaders help team members resolve task and role ambiguity, and provide external monitoring and feedback on their performance. This form of leadership allows the team to execute decisions more quickly. In the trauma bay, directive leadership is most effective when Injury Severity Score (ISS) is high or teams are inexperienced [2].
Alternatively, transformational leadership inspires and motivates followers in ways that go beyond rewards. This type of leadership increases the followers’ intrinsic motivation through the explanation of the leader’s goals [4]. In the trauma context, this is the leader you watch as a medical student, junior resident, or fellow whom you want to emulate. This leader inspires you to provide exceptional care and they help you understand how the trauma bay and trauma system at large function effectively. Taking this concept a step further, empowerment leadership described by Ford et al. encourages self-reliance and psychological empowerment. These leaders empower their teams and support them in reaching their goals, providing guidance, and creating a culture of trust. Empowering leadership is most effective when ISS is low or teams are more experienced [2].
While transactional and transformational leadership can positively influence a trauma team and progress patient care, passive leadership can be quite dangerous. Passive leadership can lead to confusion and a lack of direction. This ultimately can spiral into a lack of engagement by team members and increase stress. Aaron’s qualitative review of health professions found more positive leadership ratings were associated with more positive attitudes towards adopting evidence-based practice [4].
Leadership Assessment ToolsTrauma team performance has been shown to impact patient outcomes and has been evaluated in prior work using various assessment tools, several of which are summarized in Table 1 [1, 5,6,7,8,9]. Using the Campbell Leadership Descriptor Survey tool [6] and a convenience sample of trauma resuscitations, Sakran et al. found that trauma resuscitations perceived as having strong attending physician leadership had faster times to completion of the secondary survey and disposition to CT scan [7]. This leadership evaluation tool uses 9 elements: vision, management, empowerment, diplomacy, feedback, innovation, creativity, style, energy, and overall leadership capacity, and a Likert scale of 1 to 4. The evaluators used a score of 1 for a statement that they felt definitely did not describe the actions of the attending surgeon and a score of 4 was used for statements the evaluators thought definitely described the attending surgeon [7].
Another evaluation tool developed by Steinmann et al., Non-Technical Skills for Trauma (T-NOTECHS), was modified for specific use in trauma [8]. The modified T-NOTECHS instrument is a validated tool analyzing five domains: leadership, cooperation and resource management, communication, assessment and decision making, and situation awareness [5, 8, 10]. Each domain ranges from 1 to 5 with “1” representing disorderly and incomplete, while “5” represents clearly defined leadership [8]. Recently, Maiga et al. performed a retrospective review of a multicenter study looking at team performance and its impact on the time to the next phase of care using the modified T-NOTECHS tool with trauma video review. The authors found strong leadership and better team performance are associated with faster transitions to next phase of care in hypotensive trauma patients [5].
In 2021, Leenstra et al. translated their previously developed, extensive Taxonomy of Trauma Leadership Skills (TTLS) [9] into a practical, short, observation tool that is tailored to the vocabulary of clinician instructors and their workflow and workload during simulation-based training [1]. This updated tool streamlines the prior 3 level structure including 37 skill elements and 67 examples into 2 phases with 4–5 elements each. It shares with previous trauma team assessment tools an emphasis on the leader’s tasks in structuring and briefing the team; coordinating actions and information; and facilitating team problem solving, but, importantly, the TTLS-SHORT adds a level of specificity by providing a number of supplemental, concrete descriptions of how the team leader can fulfill these tasks [1].
Table 1 Leadership evaluation toolsProfessionalismJust as the style of leadership and approach sets the tone for the team in the trauma bay, professionalism can significantly impact team culture. The foundation a trauma team leader forms to create a collegial work environment sets the tone for every patient encounter. Professionalism supports the delivery of safe, effective, patient-centered, and equitable clinical care. It creates a culture that allows team members to speak-up and voice suggestions and concerns. The basic tenets of medical professionalism are deeply embedded in the historical context via oaths [11].
Recently, Cooper et al. performed a retrospective cohort study using data from 9 Level 1 trauma centers from a national database of unsolicited patient complaints between 2012 and 2017. The exposure of interest was care by 1 or more high-risk services, defined as teams with a greater proportion of physicians with high numbers of patient complaints. Among the greater than 70,000 patients in the cohort, 13.4% experienced the primary outcome of complications or death. Trauma patients who received care from at least 1 service with a high proportion of physicians modeling unprofessional behavior were at an increased risk of complications or death [12]. This work demonstrates that professionalism in healthcare is critical to uphold in the setting of a multidisciplinary team, specifically the high-stakes environment of the trauma bay.
Command and ControlWhile traditionally hierarchical leadership structures have come under scrutiny [13], high performing teams ultimately do require a singular leader under whom information flows towards and decisions flow down from. The primary responsibility of the trauma team leader is to command and control the resuscitation. The term “command and control” stems from the military and is used to describe a group of organizational processes employed to complete missions. In the trauma bay, that mission is successful resuscitation and it relies upon the skill sets of multiple individuals under the direction of the trauma leader with each individual team member working towards the common goal. Command and control processes do not place unilateral control in a singular person but rather a singular role. This requires mastery of relevant medical knowledge, coordination of information from pre-hospital medical services and real-time physiologic data, clinical decision-making, and coordination of multidisciplinary care.
Command and control constitute high level non-technical skills that must be developed through concerted effort and leadership skills training as this is not inherently a natural strength for some physicians. There are four key elements to command and control: authority, responsibility, decision-making, and leadership. While traditionally associated with military and aviation settings, command and control frameworks have been increasingly adapted to medical contexts to enhance efficiency and safety during critical events. Effective command and control structures help reduce ambiguity, streamline communication, and ensure accountability, which are essential for managing complex clinical situations [14]. However, strict adherence to a hierarchical structure can hinder the flow of vital information from team members to the trauma team leader, underscoring the need for balanced leadership that combines authority with openness to input.
Despite persistent myths of the adrenalin-junkie trauma surgeon, a key component of trauma resuscitation leadership is chaos reduction. The trauma team leader must foster an optimal environment to ensure team members are able to complete resuscitative tasks. The trauma bay has little margin for error and can be considered a high pressure situation. Delegation of tasks has been extensively studied in cardiopulmonary resuscitation (CPR) and code team performance [15,16,17,18]. Each role within the trauma resuscitation team has defined and/or designated tasks and it must be clear what tasks each role must accomplish. Ultimately, active resuscitation of traumatically injured patients requires a delicate balance amongst the team members to achieve successful, high-quality clinical outcomes.
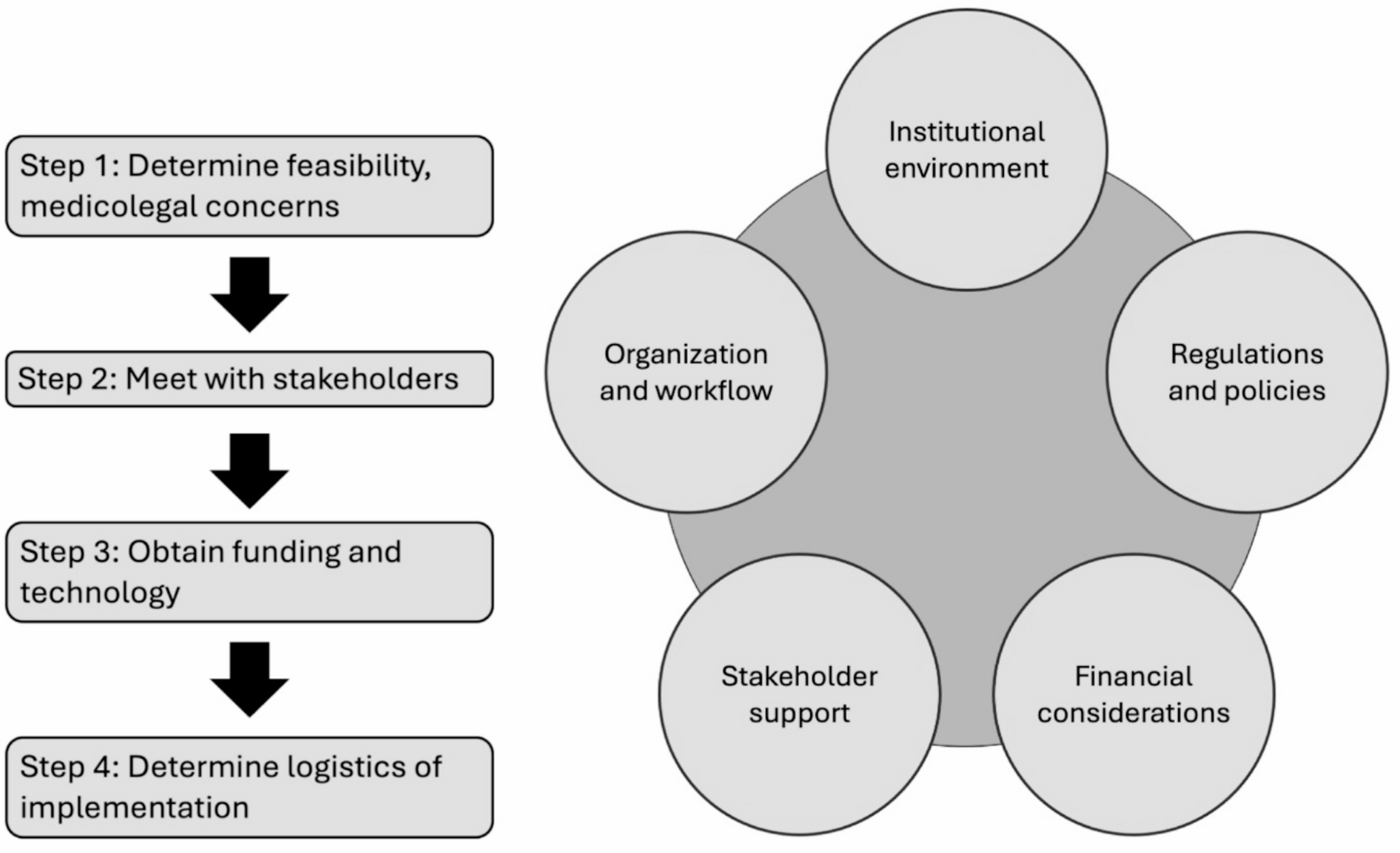
Systems-based PracticeTransitioning to a large scale perspective, the trauma team leader must conform to the resources and constraints of the hospital system in which they are practicing. The resources and systems available in a mature Level 1 trauma system are substantially different than the resources and processes of a Level 3 trauma facility. A foundational concept of ATLS is triaging patients to a higher level of care if management of their injuries requires it. Therefore, effective trauma team leadership acknowledges the limitations of their system. For example, emergency access to blood products for resuscitation varies widely across the United States and hospital systems. Resuscitation that exhausts the resources of the local system can be catastrophic for the patient.
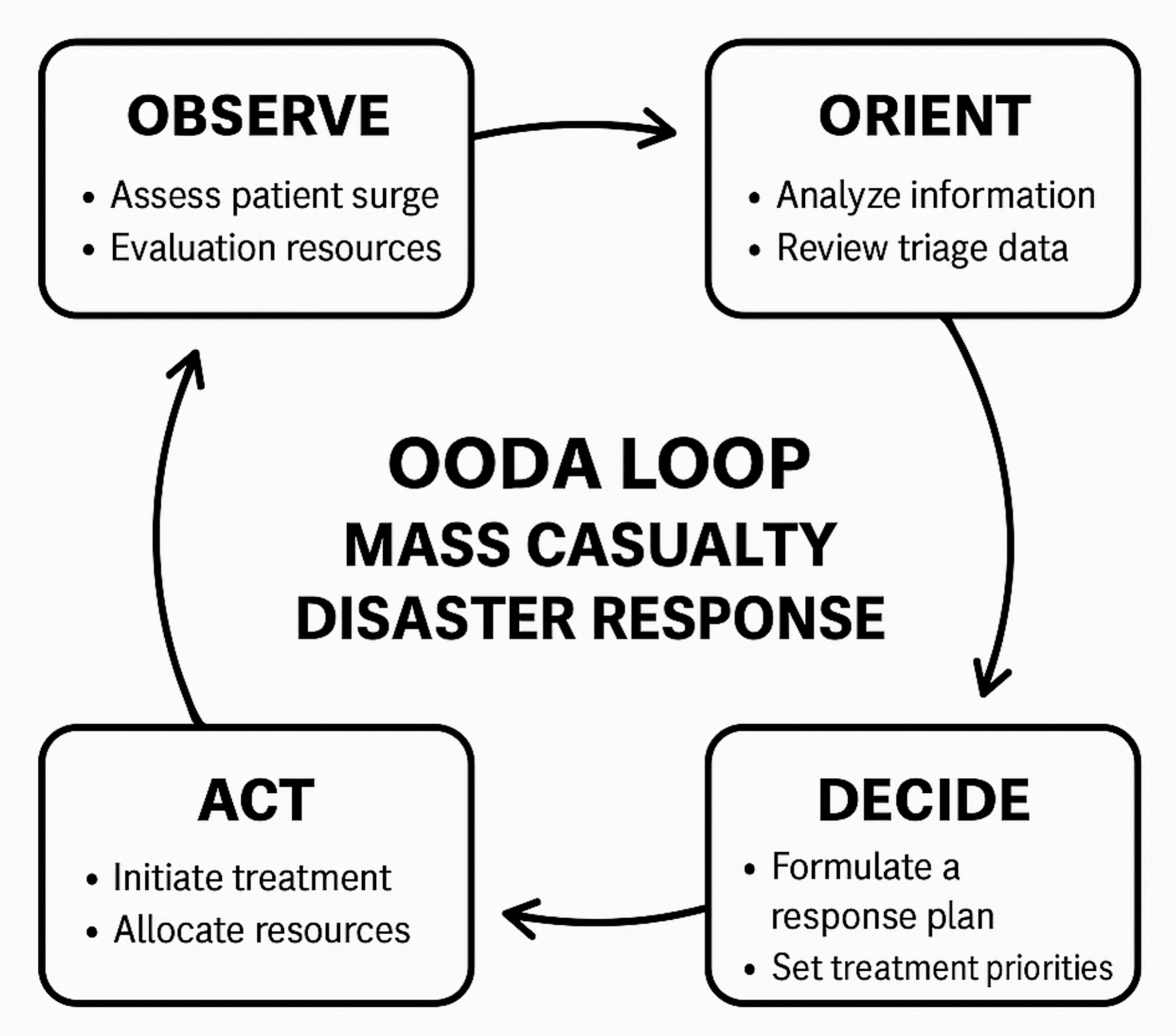
A recent qualitative analysis of leadership during the COVID-19 disaster response identified leadership that created a common operational picture positively impacted decision-making [19]. Often termed a shared mental model, this thought process enables coordinated action and effective communication in high-stakes environments. A shared mental model refers to a common understanding among team members regarding tasks, equipment, roles, and situational dynamics, allowing individuals to anticipate resuscitation needs and actions without explicit communication. In resuscitation, having a common cognitive alignment enhances decision-making speed and accuracy, reduces errors, and supports adaptive performance under pressure. Several studies have demonstrated that teams with well-developed shared mental models demonstrate superior situational awareness, improved task execution, and enhanced patient safety outcomes [15, 20]. Johnsen et al. analyzed video recordings of trauma teams and found a positive correlation between trauma leaders who created a better shared mental model and high quality medical management [21]. A shared mental model creates a roadmap for the resuscitation team. This requires clear communication from the trauma team leader, but also input of pertinent information from the team members.
A key aspect of creating a shared mental model is setting the stage for resuscitation with a pre-brief when able. The structure and information contained within the pre-brief can vary by program or institution. A pre-brief consists of a round-robin introduction of team members by name and role. The trauma team leader then summarizes the available information about the patient communicated by the pre-hospital provider call-in. Any potential deviations from standard protocols or limitations in therapeutic interventions are discussed pro-actively. For example, the trauma team leader may emphasize to the resuscitation team that a patient with a gunshot wound to the head and exposed brain matter is not a candidate for a resuscitative thoracotomy should they progress to traumatic cardiac arrest. This helps create a framework for the team members and eliminates unnecessary preparations by the team.
Clear communication underpins both command and control and systems-based practice. Closed-loop communication is a structured method of information exchange that enhances clarity, accountability, and task completion in medical settings, particularly during emergencies, code responses, and trauma resuscitations. Closed-loop communication involves three key steps: the sender issues a clear, concise order or message; the intended receiver repeats the message back to confirm understanding; and the receiver communicates completion of the task. In time-sensitive and high-pressure situations when it is imperative that orders are heard, understood, and acknowledged, closed-loop communication reduces the risk of errors associated with miscommunication—a leading cause of adverse events in healthcare [22]. Evidence shows that teams trained in closed-loop communication demonstrate improved coordination, faster response times, and improved patient outcomes [23]. Leadership that utilizes close-loop communication in the trauma bay should be considered best practice.
Leadership EducationAs we have discussed thus far, trauma leader traits and actions – leadership style, professionalism, command and control, and system-based practice - impact how a trauma scenario unfolds [24]. Effective leadership training is a crucial component in preparing physicians to handle complex challenges and responsibilities inherent in trauma [25]. This preparation needs to be thoughtful and realistic. Simulation and trauma video review are powerful technologies that present rapidly expanding opportunities for this training and exposure. For instance, an early study by Hoff et al. evaluated the identified command-physician on resuscitation performance using trauma video review. The authors found an identified command-physician enhanced trauma resuscitation performance [26].
In the world of simulation, Cassidy et al. evaluated interdisciplinary trauma simulation scenarios to understand the role of simulation and its impact on the overall culture of trauma-related care. They concluded simulation can allow for leadership strategy practice in a safe, collaborative learning environment [24]. Additionally, Park et al. performed a prospective, observational study at their Level 1 trauma center looking at the impact of implementation of a trauma procedural skill and simulation program to train and evaluate postgraduate year 1–5 residents. This included leadership skills with granular assessment. A total of 40 residents participated and overall score increased over time [27]. These are just a few recent examples of the exciting work being done in this space.
Putting It into PracticeUltimately, effective leadership is paramount to a trauma team’s success and progression of the trauma patient’s care. It is imperative that individual team members and the trauma system as a whole dedicate time and effort to leadership training and education. Additionally, providing feedback on trauma bay leadership performance to all future/current team leaders is crucial to improving this important non-technical skill. Effective feedback can be completed via many platforms including: real-time debriefing after a trauma activation, a quick evaluation tool specific to leadership skills [28], simulation, and/or trauma video review. Leadership is a skill, whether innate or learned, but it is clear leadership in trauma requires dedicated effort and a multifaceted approach is likely best.
Comments (0)