
Remember me


Acute care surgery is undergoing a transformation, driven by advancements in technology and the pursuit of improved outcomes, efficiency, and safety. Among these innovations, robotic-assisted surgery has emerged as a powerful tool. While initially adopted in elective fields such as urology, gynecology, and colorectal surgery, robotics is now finding a role in the emergency operating room. This transition is fueled by increasing surgeon familiarity, growing institutional support, and recognition of the advantages that robotic systems offer including enhanced dexterity, tremor filtration, 3D visualization, and ergonomic benefits especially in high-stakes, time-sensitive scenarios [1].
Transitioning from occasional use to a fully operational 24/7 robotic acute care surgery program is a major undertaking. It’s not just about having a robot onsite but requires deliberate planning, interdepartmental coordination, and consistent institutional buy-in. Key challenges include ensuring adequate staff training across the board—from surgeons and anesthesiologists to scrub techs and nurses as well as establishing protocols for robot access, maintenance, and real-time availability of trained personnel [2].
These logistical and operational hurdles have prevented many centers from offering continuous robotic access in acute care settings. However, as evidence supporting minimally invasive techniques in emergent procedures grows, expanding robotic capabilities is no longer a futuristic concept, it’s increasingly becoming an expectation [3].
Additionally, patient and system-level expectations are evolving. Patients now seek care that minimizes pain, hospital stays, and complications, while healthcare systems aim for value-based outcomes. Robotic-assisted emergency surgeries have been associated with fewer surgical site infections, reduced opioid use, and faster recovery in select studies [4]. For providers, the ergonomic advantage of robotics especially during prolonged or off-hour procedures can reduce fatigue and musculoskeletal strain, promoting consistent performance and surgeon well-being [5].
In academic and high-volume centers, a 24/7 robotic program also enhances training opportunities, providing residents and fellows hands-on experience with robotic platforms in emergent scenarios. This exposure prepares the next generation of surgeons to meet the growing demand for robotic proficiency and supports system-level initiatives such as care standardization, quality improvement, and real-time data collection [6].
This paper outlines the key elements of building and sustaining a 24/7 robotic acute care surgery program. We will explore the rationale, logistical considerations, team training, workflow optimization, and institutional factors necessary for success. Insights from early adopters and practical solutions to common barriers will also be highlighted.
Role for Robotics in Acute Care SurgeryThe use of robotic technology in acute care surgery is more than a technical upgrade, it’s a strategic evolution aimed at improving outcomes in emergency settings. While robotics has been widely established in elective surgery, its integration into acute care environments has proven both feasible and advantageous [7].
In the emergency setting, robotic platforms significantly enhance a surgeon’s technical capabilities. The system’s wristed instruments, expanded range of motion, and stable three-dimensional visualization are particularly valuable when navigating complex, inflamed, or distorted anatomy—common in cases such as incarcerated hernias, perforated diverticulitis, and acute cholecystitis.
While laparoscopic emergent hernia repair has been established as a safe procedure in the acute setting, data regarding robotic emergent hernia repair is very sparse [8]. A 2021 study by Bou-Ayash et al. which included 19 incarcerated hernia patients, reported that robotic emergent hernia repairs were associated with shorter hospital stays and low complication rates [9]. In another study by Kudsi et al., from 2013 to 2019 which included 35 patients undergoing robotic emergent ventral hernia repair, open repair hernia repairs was associated with a four-fold increased risk for development of complications, despite longer operative times with robotic approach [10].
Similarly, Curfman et al. found that robotic surgery for diverticulitis resulted in lower anastomotic leak rates, ICU admission rates, decreased overall length of stay compared to open procedures, whereas when compared to laparoscopic the only difference was fewer anastomotic leak and conversion to open rates [11].
The current literature presents varying perspectives regarding cholecystectomy. In a study by Klein et al. involving 260 patients, robotic cholecystectomy was associated with shorter operative times in grade B and grade C cholecystitis (based on the Parkland scale) compared to the laparoscopic approach, with similar rates of conversion to open surgery [12]. Similarly, a retrospective study by William et al., utilizing the National Surgical Quality Improvement Program (NSQIP) database, found that robotic cholecystectomy was associated with shorter hospital stays and reduced 90-day readmission rates [13]. However, multiple meta-analyses and systematic reviews comparing the two techniques for benign gallbladder disease, including both cholecystitis and cholelithiasis, have yet to demonstrate consistent clinical advantages of robotic over laparoscopic cholecystectomy [14,15,16].
In a 2025 retrospective study which on robotic acute care surgery, which included cholecystectomy, hernia repairs, appendectomy, sigmoid colectomy and adhesiolysis concluded that robotic techniques can be implemented safely with potential benefits to both the surgeon and the patient [7]. Another similar study by Lunardi et al., which looked at three emergent procedures; cholecystectomy, hernia repair and colectomy found that robotic surgery might be associated with shorter post-operative stays and lower conversion rates to open surgery [17].
Although appendicitis is one of the most common acute general surgical condition, few studies have examined the role of robotic appendectomy. Studies by Rifai et al. and Becker et al. concluded that while robotic appendectomy is associated with longer operative times and higher costs, it may reduce postoperative length of stay and lower the rate of conversion to open surgery [18, 19].
Robotic surgery has significantly expanded the eligibility criteria for minimally invasive procedures, particularly benefiting patients with obesity, prior surgeries, or complex anatomical challenges.
Traditional surgical approaches often pose increased risks for obese patients, including higher rates of surgical site infections (SSIs) and wound complications as well as increased surgeon fatigue due to the fulcrum effect. Robotic-assisted techniques have been shown to mitigate these risks. A study by Oberholzer et al. demonstrated that robotic kidney transplantation in obese patients resulted in lower infection rate compared to the open surgery control group, despite the robotic group having a higher average BMI [20]. Similarly, research on robotic rectal surgery indicated that the approach is as safe and effective in obese patients as in non-obese individuals, with comparable complication rates and pathologic outcomes [21]. In a case report on robotic cholecystectomy in a super obese patients, the authors discuss the difficulty of performing a conventional laparoscopic procedure in this subset of patient population and how robotics is a viable alternative [22].
In patients with prior abdominal surgeries, robotic systems offer enhanced dexterity and superior visualization, facilitating safer and more precise dissections. A study by Ball et al. found that postoperative outcomes in patients undergoing robotic prostatectomy were comparable between those with a history of prior abdominal surgery and those without, highlighting the safety and feasibility of the robotic approach in this population [23].
Robotic platforms provide surgeons with improved precision when navigating complex anatomical regions and the current literature highlights that the primary technical advantages of robotic surgery over laparoscopy, lie in enhanced suturing and precise dissection. In the context of emergency robotic procedures, several complex maneuvers have been successfully performed including hiatoplasty, ventral hernia repair with suturing or mesh fixation, colonic and duodenal stump suturing and dissection of inflamed gallbladders or colons. These steps, often technically demanding during laparoscopy, are more easily facilitated with robotic assistance and are frequently cited as reasons for conversion to open surgery, an intervention associated with increased risk of postoperative complications [10, 24,25,26].
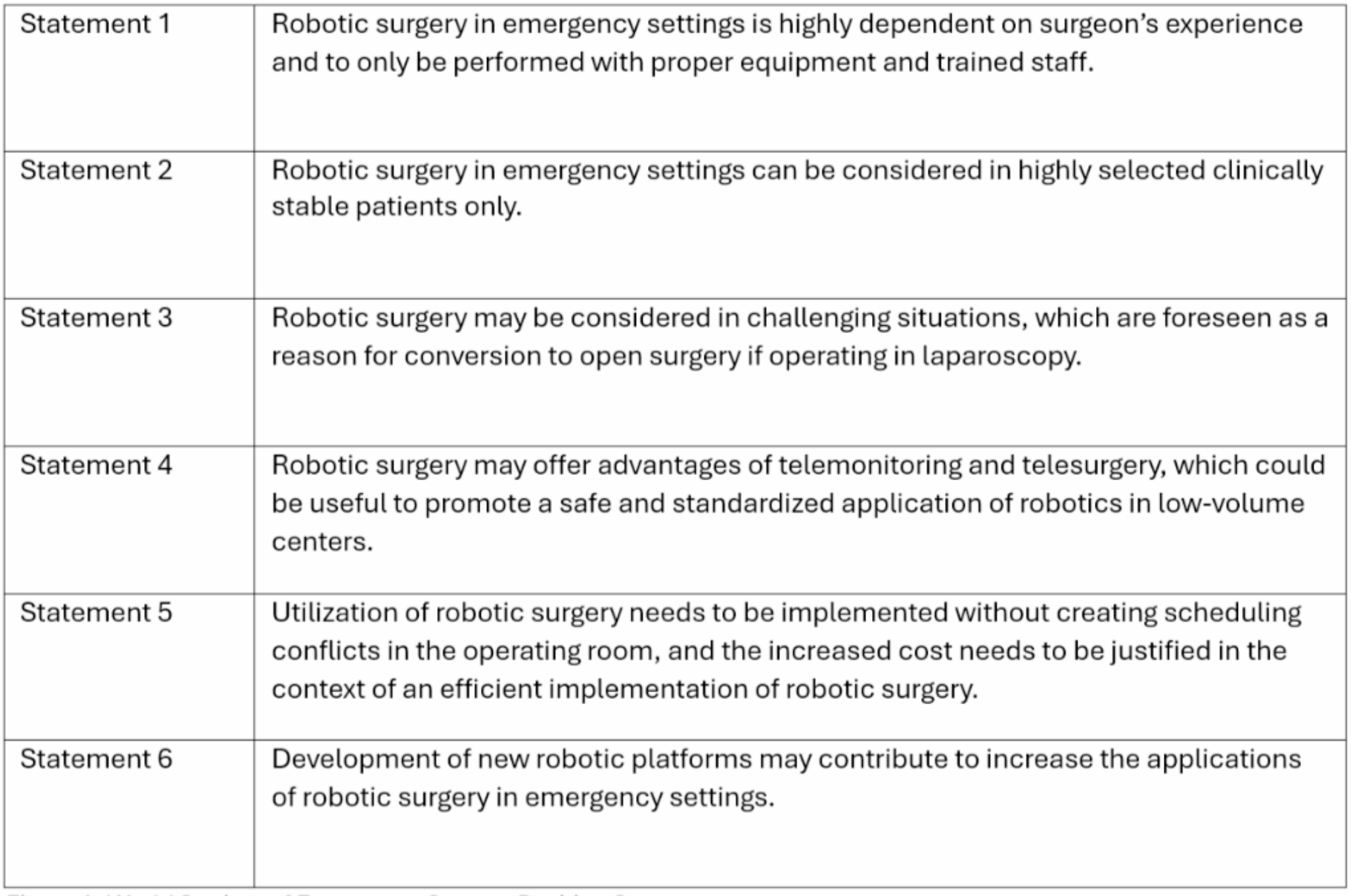
As summarized in Table 1, robotic surgery in emergency general surgery has been associated with favorable outcomes, including reduced postoperative stays, lower complication rates, and decreased conversion to open procedures across various study designs.
Table 1 Summary of studies evaluating robotic surgery in emergency general surgeryRobotic surgery also holds promise for expanding access to expert surgical care through tele-mentoring and tele-surgery, particularly in low-volume centers and resource-limited settings. Unlike laparoscopy, robotic platforms allow for in-person dual-console mentoring and, with advancements in internet technology, may soon enable real-time remote assistance and even operative control. This could significantly enhance surgical safety and standardization, especially in emergency settings where expertise is critical. Potential applications range from rural and underserved areas to extreme environments like space, military zones, or deep-sea operations. While challenges related to infrastructure, legal, and cybersecurity concerns remain, ongoing developments suggest a pivotal role for robotics in the future of telemedicine [27, 28].
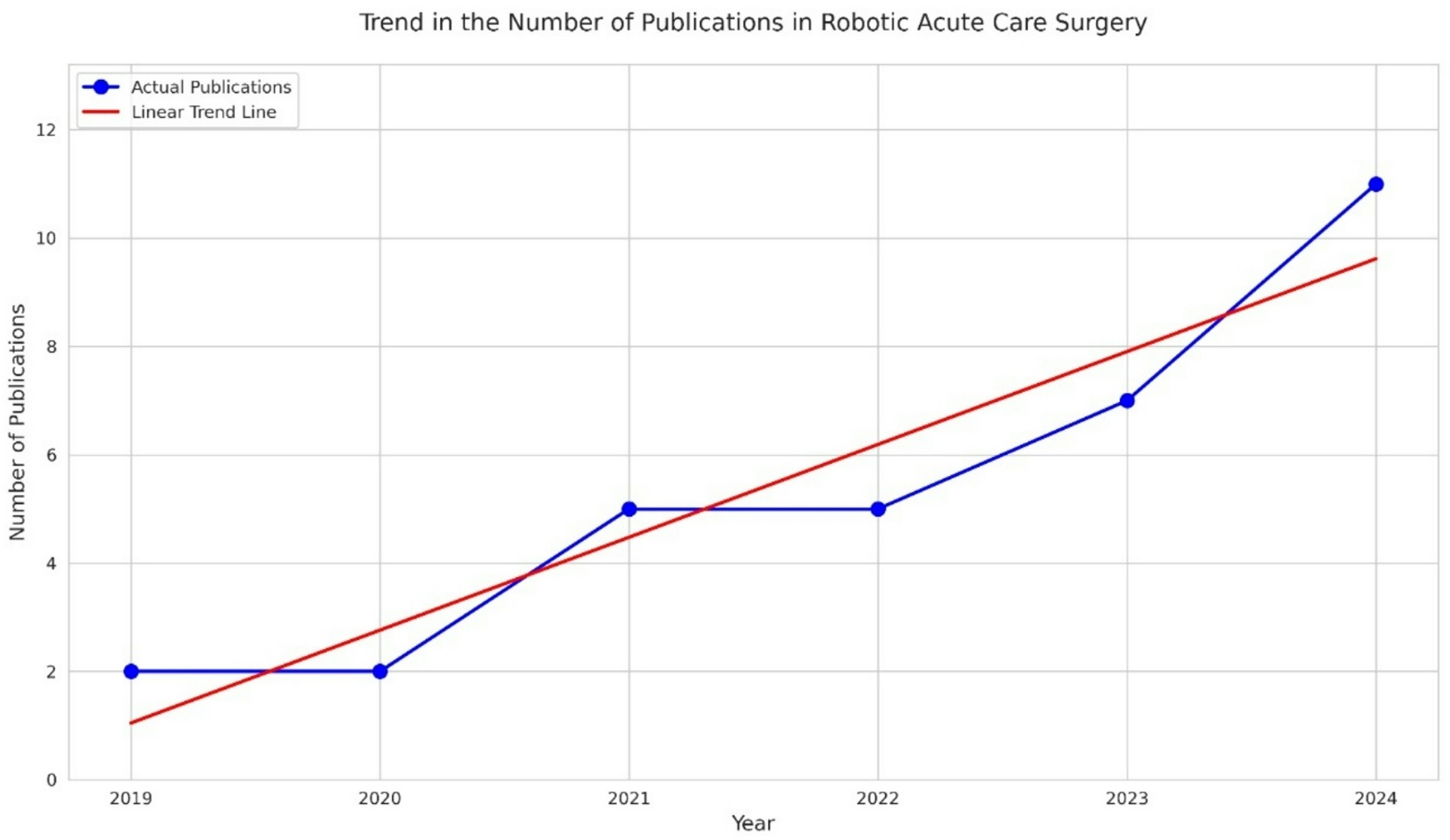
As demonstrated in Fig. 1, there has been a noticeable increase in the number of publications including related to robotic acute care surgery over the past few years, reflecting a growing interest among surgeons and institutions in applying robotic platforms beyond elective procedures.
Fig. 1
Annual Trends in Publications on Robotic Acute Care Surgical Procedures
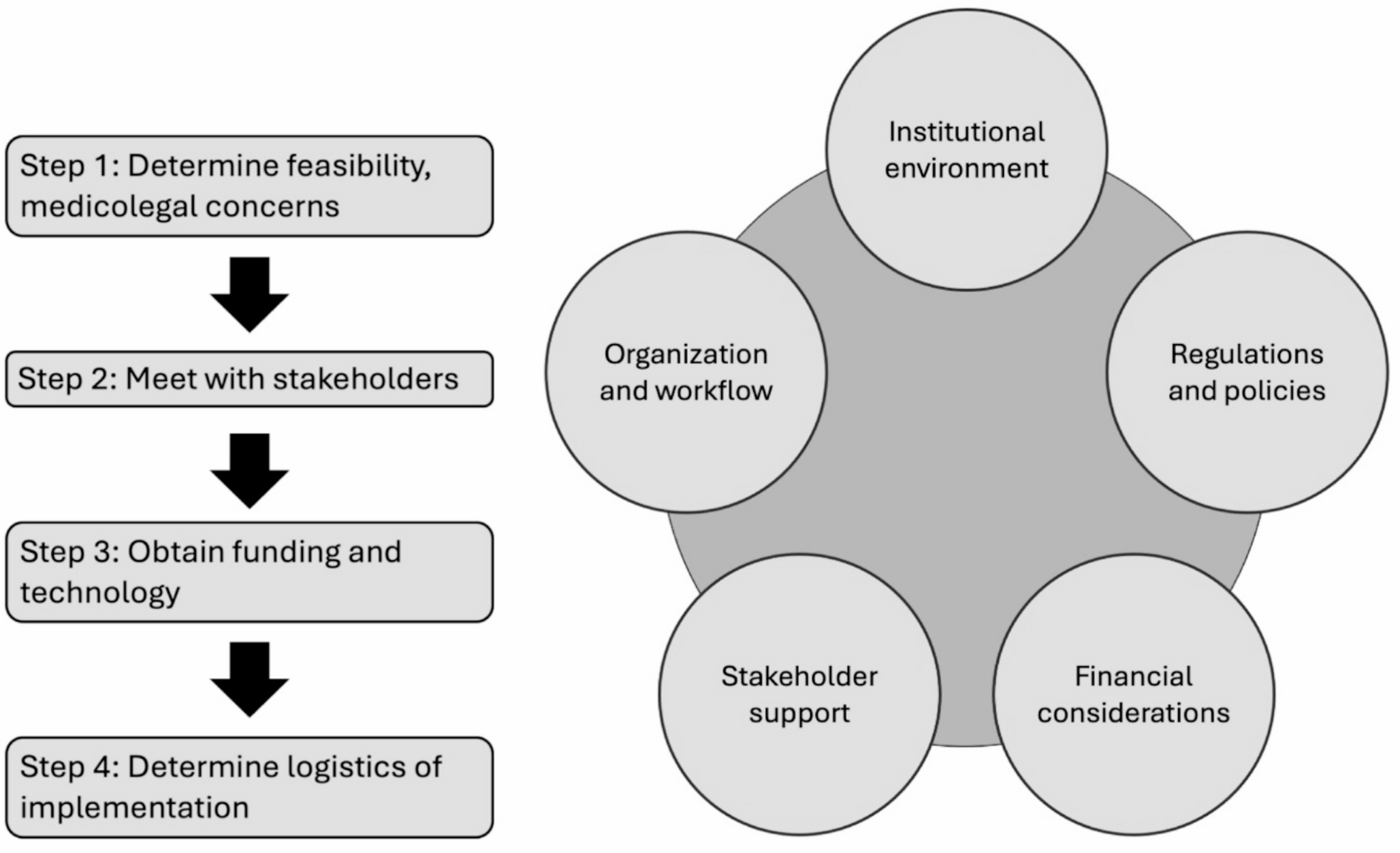
Initiating and Implementing a 24/7 Robotic Acute Care Surgery ProgramInitiating and maintaining a 24/7 robotic acute care surgery (ACS) program is a complex process that demands planning, infrastructure development, staff training, and financial sustainability. The evolution of robotic acute care surgery has been heralded by advancements in technology and increasing institutional interest, yet the successful implementation of such a program requires overcoming logistical and financial hurdles while ensuring stable patient outcomes. Following checkpoints need to be crossed over for a successful implementation (Table 2):
Table 2 Steps for implementing a 24/7 acute care surgery robotics programSecuring Institutional and Stakeholder EngagementThe first step in establishing a 24/7 robotic ACS program is securing engagement from institutional leadership and relevant stakeholders. A multidisciplinary team constituting leaders from all areas of surgical patient care needs to be formed. Insights from hospital administration, surgical leaders, anesthesiology, nursing, and central sterile services departments must align to establish strategic goals. Prior research highlights the importance of strong inter-departmental collaboration for a successful robotic ACS program [29, 30]. Programs have benefitted from the appointment of a surgeon leader who can actively engage high-level administration and demonstrate the need for introducing robotic surgery in ACS, both in terms of improved patient outcomes and gaining an institutional edge in the market. This leader can also initiate an open channel of communication between administration and the multidisciplinary task force to aid in the creation of a robotics program [31].
Infrastructure and Resource AllocationRobotic surgery requires more than just acquiring the platform itself. It requires thorough planning around operating room setup, staffing, and workflow integration. A dedicated robotic OR and reliable IT support for tele-mentoring, remote monitoring, and data integration are essential. Robotic surgery also requires changes in OR scheduling, equipment setup, and coordination among OR staff.
Leveraging existing hospital infrastructure can ease implementation, but success depends on close collaboration with perioperative leadership, OR directors, and robotic program coordinators. This collaboration helps secure consistent access to a robotic-equipped OR. Many programs use a phased approach, starting with limited hours and gradually expanding availability as staff experience and case volume grow [29]. A robotics coordinator can manage supplies, staff training, equipment maintenance, and workflow efficiency [29]. Trained OR staff and on-site representatives from Intuitive Inc. offer hands-on support, troubleshooting, and real-time guidance. As the program matures, additional training for after-hours staff and 24/7 technical support ensure the robotic service remains consistently available.
Training and Competency DevelopmentInitial training for surgeons typically involves guided simulation-based sessions organized by Intuitive Inc on a robotic console. These virtual reality simulations, which are part of a large library of procedure training exercises available, allow for the surgeon to become comfortable controlling the robotic arms and instruments prior to performing their first cases on patients. Additional training options include wet labs, held at various Intuitive Surgical campuses where pig models are utilized to further develop the surgeon’s familiarity with the robotic surgery platform by allowing surgeons to perform cholecystectomies, inguinal hernias, and ventral hernia repairs on these models. Once the surgeon is comfortable and ready to begin operating on patients in a clinical setting, proctors who are trained surgeons either from the home institution or provided by the company will offer direct mentorship during operative cases [29]. Depending on institutional policies agreed upon, the number of proctored cases may vary between institutions.
One study showed that training individual surgeons, rather than all at once, reduces financial burdens on institutions and minimizes disruptions to patient care [31]. Gradually involving surgeons in elective cases before transitioning to acute care helps build confidence for both the surgeons and their patients [29, 31]. In addition to the surgeon training, technology training pathways are available through Intuitive Surgical for OR nurses, patient-side assists, and robotics coordinators and several institutions have adopted these structured training programs, ensuring a cohesive and well-prepared surgical team [30]. Maintaining competency through regular assessments and continued education ensures that skills do not degrade over time, with programs that invest in these pathways seeing improvements in surgical outcomes [31].
The introduction of a robotics curriculum in acute care surgery fellowships is another important strategy for developing a skilled workforce. Modifying the curriculum to suit the trainee’s level of experience during residency has shown promise in ensuring that fellows receive appropriate training [32]. This early exposure enables fellows to gain essential robotic skills that are foundational for their future roles, facilitating a smoother transition into the workforce and enhancing their confidence in handling both elective and acute care robotic cases.
Establishing a 24/7 Robotic Surgery Call SystemEnsuring around-the-clock availability can be challenging, particularly in the early stages of program development. One approach is implementing a tiered call system, where multiple surgeons are trained in robotic techniques to provide backup and flexibility for urgent cases [30, 31]. Cross-training surgeons in both robotic and conventional methods is also effective, ensuring no delays in care due to robotic platform unavailability or surgical expertise gaps.
Some institutions have found success by starting with a volunteer call model during the initial phases of the program. Gage et al. launched a three-month trial period where robotic cases were carefully selected, and participation was limited to interested surgeons, anesthesiologists, nursing staff, and a representative from Intuitive, Inc. This volunteer-based team was on-call to respond when appropriate cases arose. The gradual, peer-driven expansion of robotic expertise ultimately increased program capacity and improved overall system readiness for un-scheduled procedures [30].
Performance MonitoringThe sustainability of a 24/7 robotic ACS program depends on the robustness of a performance monitoring system. This system should collect data on various metrics, such as complication rates, surgical outcomes, length of stay, and conversion rates from robotic to open surgery. This can help in identifying areas for improvement and enable ongoing refinement of the program [29]. A system of constant evaluation for the appropriateness of case selection has to be established to ensure appropriate utilization of resources and optimal patient care.
Cost OptimizationThe upfront investment in robotic platforms, ongoing maintenance costs, and the need for specialized training all contribute to increased expenditures. However, evidence from established programs suggests that these initial costs can be offset over time. Effectively integrated robotic programs have been linked to lower complication rates, reduced lengths of hospital stay, and enhanced surgical efficiency [33, 34], all of which can help drive long-term cost savings.
While early phases of implementation often involve longer operative times and higher costs, data show that with experience, operative times typically decrease. In some cases where costs remain high, it is often due to the increasing complexity of the procedures being performed, rather than inefficiency [35]. Programs tend to progress toward managing more complex patients like those with significant comorbidities, once robotic proficiency is established, which can influence cost metrics.
Challenges in Implementation and MaintenanceDespite the advantages of robotic ACS, challenges persist, particularly around financial investment, workforce requirements, and integrating robotic systems into existing hospital workflows. The high capital costs of robotic systems remain a significant barrier to implementation, especially for hospitals with limited financial resources. To overcome this, hospitals can consider phased adoption strategies, where they gradually increase their robotic surgery volume as the program becomes more established. Another key challenge is ensuring a sufficient number of trained surgeons to staff the program around the clock. To address this, institutions can employ tiered scheduling models and shared robotic platforms to optimize resource allocation and prevent burnout among staff.
Workflow integration is also a challenge, as robotic surgery requires changes to the typical operative processes. These changes need to be managed carefully to avoid disruptions. For example, adjustments must be made to the way instruments and supplies are handled in the operating room to accommodate robotic platforms. Furthermore, not every ACS case is appropriate for robotic surgery, so establishing clear triage protocols is crucial for determining when to use robotic technology and when to rely on traditional methods.
Future Directions and InnovationsLooking to the future, robotic ACS programs will continue to evolve as technological advancements and new research emerge. One area of innovation is the integration of artificial intelligence (AI) into robotic surgery platforms. AI can support surgeons by providing real-time decision-making tools, improving precision and reducing the likelihood of errors. Additionally, augmented reality (AR) and tele-mentoring are poised to enhance the training and deployment of robotic surgery, allowing for remote collaboration and expertise-sharing. As these technologies develop, they will likely reduce the need for in-person robotic specialists, making robotic surgery more accessible to hospitals in remote or underserved areas.
Moreover, expanding training pathways is a promising direction for increasing the adoption of robotic surgery. Incorporating robotic surgery into surgical residency programs and acute care fellowships will help train the next generation of surgeons to use robotic systems from the outset of their careers. This early exposure will reduce the learning curve and improve the efficiency and effectiveness of future robotic ACS programs.
The financial models surrounding robotic surgery will also continue to evolve. Value-based care models, which focus on rewarding healthcare providers based on patient outcomes rather than the volume of procedures performed, are expected to play a larger role in determining the feasibility of robotic ACS programs. These models encourage hospitals and surgeons to focus on improving patient health outcomes rather than simply performing more surgeries.
Comments (0)