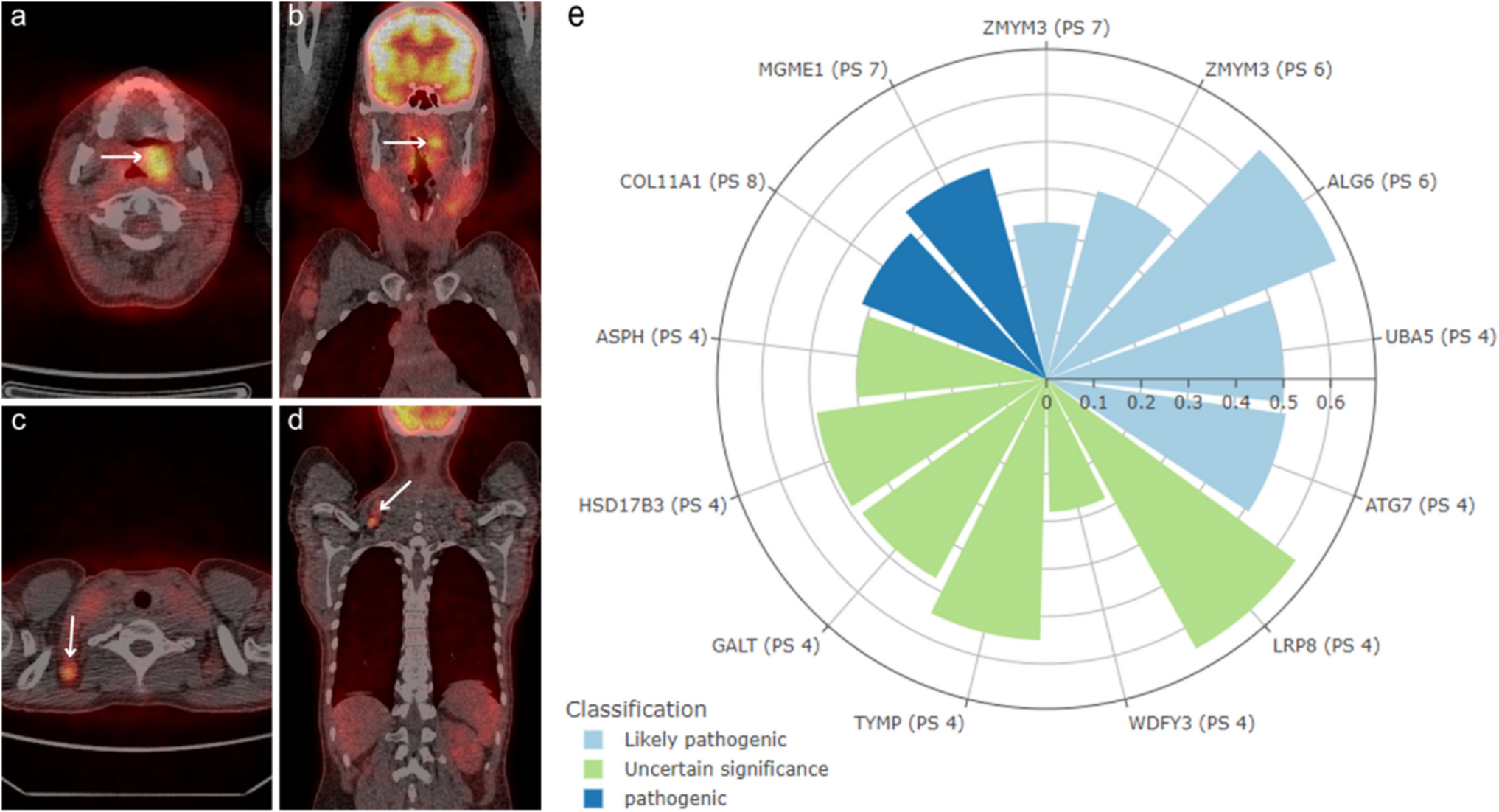
A possible mechanism of B-CLL cells’ transformation to a more aggressive form is the acquisition of transforming genetic aberrations. The most common mutations that can lead to RT are those observed in TP53, NOTCH1, c-MYC, and subset 8 stereotype (Al-Sawaf et al. 2021; Filip and Mraz 2020). In the presented atypical B-CLL patient, based on WGS, we identified two variants classified as pathogenic (COL11A1, MGME1), and five likely pathogenic (ALG6, UBA5, ATG7, and two ZMYM3 variants). The lack of TP53 mutation may be favorable as mutations in this gene are generally related to poor prognosis of B-CLL (Al-Sawaf et al. 2021). However, the presence of del 17p is another factor indicating an adverse prognosis (Al-Sawaf et al. 2021). We did not identify other mutations frequently reported in B-CLL, i.e., SF3B1, IGLL5, NOTCH1, and ATM (Robbe et al. 2022). Out of the genes that are recurrently mutated in B-CLL and lead to developing RT (Robbe et al. 2022), we detected only ZMYM3, BIRC3, and MGA. However, the last two variants (MGA p.Ser736Leu, c.2207C > T, and BIRC3 p.Arg434fs, c.1299_1300delAA) were not highly scored by the eVai prioritization algorithm.
The presence of the ZMYM3 mutations was confirmed in 2–4% of patients with B-CLL (Rodríguez-Sánchez et al. 2023). The recent study results suggested that ZMYM3 dysfunction can cooperate with NOTCH1 signaling mutations in B-CLL evolution. This is supported by the observation that ZMYM3 mutated patients also harbored mutations in the NOTCH pathway genes, either in NOTCH1 or its negative regulators MED12, FBXW7, and SPEN. Moreover, ZMYM3-mutated cells are resistant to apoptosis due to lower expression of caspases and increased level of anti-apoptotic proteins (BCL2, MCL1, BCL-XL). Therefore, the presence of mutations in ZMYM3 may potentially predict the sensitivity of B-CLL cells to anti-BCL2 therapy (e.g., venetoclax). ZMYM3’s role in RT may also be explained by the fact that ZMYM3 mutations impair DNA damage response by disturbing the cell cycle arrest in G2/M phase after irradiation (Rodríguez-Sánchez et al. 2023). The presence of two mutations with serious biological consequences in ZMYM3 gene, already related to B-CLL, supports the putative role of ZMYM3 in RT. However, it requires further studies.
Abnormalities of autophagy-related genes (e.g., ATG7) may be another possible mechanism of B-CLL evolution to a more aggressive disease form. ATG7 promotes autophagy, cell cycle arrest, and apoptosis mediated by the tumor suppressor p53 (Lee et al. 2012), and represses the pro-apoptotic activity of caspase 9 (Han et al. 2014). ATG7’s role in invasion and metastasis processes, unrelated to the protein’s function in the autophagy process, was also reported (Long et al. 2022). Other authors underlined the therapeutic potential of inhibiting BCR-mediated autophagy pathways in more effective B-CLL cell killing (Smith et al. 2020).
There is no available data about the impact of pathogenic variants of COL11A1 and MGME1, likely-pathogenic variants of ALG6, UBA5, and VUS of HSD17B3, ASPH, GALT, TYMP, WDFY3, and LRP8 on the course of B-CLL. However, MGME1 mutations were observed in B-CLL fludarabine resistance (Pandzic et al. 2016).
Finally, even though variants in BIRC3 and MGA were not highly scored by eVai prioritization algorithm, they could play a supporting role in developing RT in our patient. The frequency of deleterious mutations in BIRC3 is estimated as 2–10% of newly diagnosed B-CLL patients (Rossi et al. 2012; Xia et al. 2015), but in fludarabine-refractory patients, it is increased to 25% (Rossi et al. 2012). It was also shown that RT predominantly developed during Bruton tyrosine kinase inhibitors (BTKi) therapy among patients with mutations in SF3B1, TP53, BTK, ATM, and BIRC3. Other analyses indicate that the disruption of BIRC3 leads to the persistent activation of NF-κB signaling, which explains the poor prognosis and resistance to FCR treatment among B-CLL patients (Rossi et al. 2012; Tausch et al. 2020; Favini 2020). BIRC3 mutations remain an independent risk factor for shorter progression-free survival and OS but they do not reduce the effectiveness of venetoclax treatment (Favini 2020).
Loss of function mutations or deletions in MGA are observed in 36% in RT cases, indicating a significant yet unknown role in the transformation of B-CLL to RT (Iyer et al. 2024). The research on mice showed that RT could result from the MGA deletion, which leads to mitochondria structure change and hyperactive mitochondrial activity in B cell lines by the higher number of cellular reactive oxygen forms, increased mitochondrial DNA copy number, higher ATP production, and elevated oxidative phosphorylation (Iyer et al. 2024).
Taking into account the genetic heterogeneity of CLL and RT, WGS seems to be an optimal method of choice in future diagnostics. Using gene panels, we may miss mutations which appear in other genes, not included in the panels. Decreasing costs of WGS in the last 20 years makes it now more comparable to the costs of exome or even panel sequencing. The WGS library preparation procedure is simpler than exome or panel library preparation, whereas the sequencing time is similar. In the case of WGS, the most challenging may be data analysis, but due to implementation of standard protocols and IVD-certified software tools which are already available, this problem should be overcome soon.
Regarding the limitations of the study, it has to be mentioned, we were able to sequence only one sample from the patient, collected at the time of RT. The biological material from the first CLL diagnosis and from the control tissue (not affected by the disease) was not available. Therefore, we were unable to assess the clonal evolution of the disease or distinguish germline from somatic mutations.
In conclusion, we presented the first case of aCLL transformation to DLBCL, successfully treated with alloHSCT. WGS of RT enabled the identification of mutations in the already known genes implicated in B-CLL, such as ZMYM3, as well as in the genes not previously associated with this disease, e.g., COL11A1, MGME1, or ATG7. Therefore, assessing the complete genetic profile of B-CLL cells is worth considering for introduction into a routine procedure at the time of B-CLL diagnosis and in any case of suspected RT. The contribution of particular genetic factors should be explored further.



Comments (0)